Research Article
Prevalence of Human ImmunodeficiencyVirus Infection in Pregnant Women and Birth Outcome at Tertiary Care Centre in a North Indian Town
Abida Malik1, Hiba sami1,2, Parvez Anwar Khan1, Nazish Fatima1, Masihuddin siddiqui3
1Department of Microbiology, J.N.Medical College, Aligarh (U.P.), India
2Department of Microbiology, SRMSIMS, Bareilly, India
3Department of Medicine, J.N.Medical College, Aligarh (U.P.), India
Corresponding author: Dr. Hiba Sami, M.B.B.S., MD (Microbiology), Assistant Professor, SRMSIMS, Bareilly, Ph-7895239786, India; E-mail: hibasamizafar@gmail.com
Citation: Malik A, sami H, Khan PA, Fatima N, siddiqui M. Prevalence of Human Immunodeficiency Virus Infection in Pregnant Women and Birth Outcome at Tertiary Care Centre in a North Indian Town. J Immunol Vaccine Technol. 2015;1(1): 104.
Copyright © 2015 sami H, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Immunology and Vaccine Technology | Volume: 1, Issue: 1
Submission: 10/10/2015; Accepted: 25/11/2015; Published: 02/12/2015
Abstract
Background and objectives: There are an estimated 2.5 million HIV-infected persons in India. Limited data is available from India on HIV and birthoutcomes. Nearly 30% are women of reproductive age who are often diagnosed for the first time during pregnancy. With the prevalence of HIV in theantenatal clinics in many parts of India nearing 1% in 2008, measures to avert neonatal adverse outcomes in this population are important for child survival.The present study was done to determine the prevalence of HIV seropositivity in females attending ANC clinic and to study the birth outcome of HIV positivepregnant females.
Materials and Methods: Materials and Methods: A prospective study was carried out over a period of three years 2011-2013) from. The sample population included 6067pregnant women registered and counselled at the antenatal clinics of this hospital. All of them were screened for their HIV status and the HIV positivepregnant females were followed up to evaluate the birth outcome
Results: A total of 6067 pregnant females were screened for the presence of HIV in antenatal patients over three year period. Overall positivity rate wasfound to be 0.41% (25 females). Despite of all precautionary measure and use of Zidovudine mother to infant transmission was seen in 2 cases.
Conclusion: Early contact with heath care facilty, ART for the pregnant HIV positive mothers, proper follow up, use of Zidovudine intrapartum andpostpartum for mother and baby is associated with a better outcome of pregnancy, reduced mother to child transmission of HIV and a normal new born.
Keywords: HIV; ART; Zidovudine
Introduction
There are an estimated 2.5 million HIV-infected persons in India,at the end of 2010; an estimated 34 million people were living with AIDS worldwide [1]. India harbours the third largest number ofHIV infected individuals in the world [2]. Nearly 30% are womenof reproductive age who are often diagnosed for the first time duringpregnancy. The first documented HIV infection in India was among a cohort of sex workers in the southern State of Tamil Nadu, in 1986[3,4]. The virus since then has been spreading rapidly across thecountry. States with a high prevalence of HIV include Maharashtra,Tamil Nadu, Karnataka, Andhra Pradesh, Manipur, and Nagaland[1,3].There is limited data from India on HIV and birth outcomes.With the prevalence of HIV in the antenatal clinics in many parts ofIndia nearing 1% in 2008, measures to avert neonatal adverse outcomesin this population are important for child survival. Determining birthoutcomes among this population along with surveillance of cases ofmother-to-child transmission is the need of hour.
The present study was done to determine the prevalence of HIVseropositivity in females attending ANC clinic and to study the birthoutcome of HIV positive pregnant females.
Material and Methods
The study area and population: This study was carried out overa period of three years from January 2011 to December 2013 in theDepartment of Microbiology, Jawaharlal Nehru Medical College,Aligarh, India. The sample population included 6067 pregnant womenregistered and counselled at the antenatal clinics of this hospital.
Sample collection and processing: Informed consent wasobtained from each pregnant woman prior to sample collection. Fiveml venous blood sample was collected in a sterile plain containerfrom all pregnant women who came for testing. Blood was allowedto clot for 30 minutes at room temperature (25-30 °C) and serum wasseparated. The serum samples were tested within 24 hrs.
HIV serology and CD4 cell count: HIV infection was diagnosedusing three antigenically different kits as per the national HIV testingpolicy [9]. CD4 cell counts were determined by flow-cytometrytechnique by Partec CyFlow® Counter (Germany). The CD4 countswere stratified in accordance with the 1993 CDC (Centers for DiseaseControl) Revised Classification for HIV infection into 3 groups – >500, 200–500, and < 200 cells/mm3.
Parameters of birth outcome perinatal Characteristics:Obstetric and Perinatal Characteristics of mother includedGestational age at time of diagnosis of HIV , CD4 cell count atdiagnosis, Risk factor for transmission, HIV status of husband,Opportunistic infections and the preventive action take at thetime of delivery (Table 2). The birth outcome of HIV positivefemales included Elective abortion, Spontaneous abortion,Gestational age at delivery, Preterm delivery ,Mean birth weight,Early neonatal mortality, Mother to infant transmission (Table 4).
Results
A total of 6067 pregnant females were screened for the presenceof HIV in antenatal patients over three year period. Overall positivity rate was found to be 0.41% (Table 1). Their age range was 16-34 years(median 24 years). The majority (44%) were in the age group 21-24years, followed by 25-29 years (28%) (Figure 1).
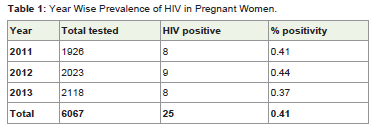
Table 1: Year Wise Prevalence of HIV in Pregnant Women.
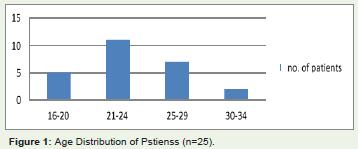
Figure 1: Age Distribution of Pstienss (n=25).
The Obstetric and Perinatal Characteristics of HIV positivefemales described in Table 2, out of total 25 HIV positive females 17were diagnosed in the first trimester, 6 females in second trimesterand 2 in the third trimester. Out of total 6067 females screened forHIV 61% had their first contact with the ANC in First trimester(Table 3, Figure 2). Husbands of 21(84%) females were tested positivefor HIV infection, and in these cases the mode of transmission wastaken as heterosexual.
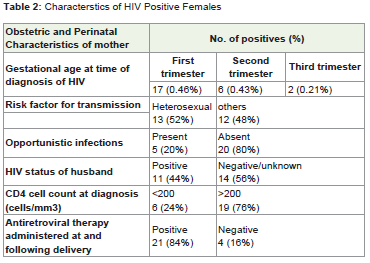
Table 2: Characterstics of HIV Positive Females.
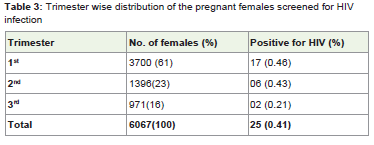
Table 3: Trimester wise distribution of the pregnant females screened for HIVinfection.
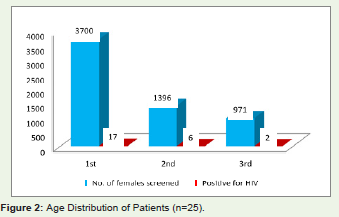
Figure 2: Distribution of Hepatitis A-E, TTV and SEN-V in patients with liver disorders.
The birth outcome of HIV infected pregnant women (Table 4),4 delivered dead fetes. The remaining 21 women gave birth to livebabies. Of these, 1 was a preterm delivery (35.2 weeks), and the restdelivered at term. There was no IUFD, spontaneous miscarriagesor maternal deaths. All live born infants received antiretroviralprophylaxis after. There was no an intra-uterine fetal death (IUFD),spontaneous miscarriages, or maternal mortality. despite of allprecautionary measure and use of Zidovudine mother to infanttransmission was seen in 2 cases.
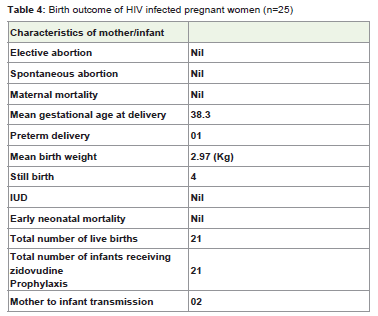
Table 4: Birth outcome of HIV infected pregnant women (n=25).
Discussion
Testing the HIV status of the females attending ANC providesan effortless opportunity not only for screening and prevent motherto-child transmission but also to sensitize and educate them aboutHIV/AIDS, family planning and preventive aspects of health care.
The present study although not representing in whole population in general, provides the insight of the prevalence of HIV positivityin the pregnant females attending ANC clinic. As expected the HIVpositivity of 0.41% in our study is higher than the overall prevalence(0.3%) in general Indian population as the study cohort includes themost vulnerable population in terms age and sexual practices. Alsobecause of the screening nature of the test rather than investigative.
While analyzing the trend of HIV prevalence and the number offemales tested in the past 3 years (2011 to 2013). The change in theprevalence rate was not significant (0.41, 0.44, 0.37%), the gradualand persistent increase in the number of female attending the ANCand screened provides some solace.
The overall, HIV seroprevalence found in our study was 0.41%.Similar seroprevalence of 0.41% were noted by Sinha et al. in 2008[4,5]. A slight higher prevalence of 0.56% were noted by Mandal et al.in 2010, 0.77% by Parmeshwari et al. in 2009 and 0.72% by Nagdeo etal. in 2007 [6-8], in comparison, lower seroprevalence of 0.17% wereobserved by Chaudhari et al. in 2010, 0.35% by Joshi et al. in 2010[9,10].
In our study, the HIV infection was highest in the age group of21-21 years (41.86%) closely followed by 20 to 24 yrs (44%). Ukey etal. reported that HIV infection was highest in the age group of 19-24 years (46.94%) followed by 25-29 years (31.29%) [11]. It may bebecause of the fact that 20 to 29 years is the most sexually active agegroup. High prevalence in this group can be considered as forecastingof financial burden as well as loss of youth for the nation.HIVprevalence in younger age groups (15-24 years) is a useful proxy fortrends in HIV incidence. A declining trend among antenatal womenfrom Karnataka, Andhra Pradesh, Maharashtra and Tamil Nadu hasbeen described [12].
Our study indicates that the HIV status of the perinatal womendoes not apparently affect the birth outcome in terms of electiveabortions, miscarriages, IUFD, birth weight, preterm labour ormaternal mortality rate. This may be because most of the femaleswere tested early in pregnancy and were put on ART along with theproper intrapartum preventive measures. This fact stresses on thetimely ANC visits of pregnant females, starting early in the gestationalage. In one study conducted on young HIV-infected Indian pregnantwomen, researchers found those who received regular antiretroviraltherapy had no adverse pregnancy outcomes [13].
In conclusion, early contact with heath care facilty, ART for thepregnant HIV positive mothers, proper follow up, use of Zidovudineintrapartum and postpartum for mother and baby is associated witha better outcome of pregnancy, reduced mother to child transmissionof HIV and a normal new born.
References
- UNAIDS Data Tables-2011.
- http://unicef.in/
- John TJ, Babu PG, Jeyakumari HM, Simoes EAF (1987) Current prevalence and risk groups of HIV infection in Tamil Nadu, India. Lancet 1: 160-161.
- Simoes EA, Babu PG, Jeyakumari HM, John TJ (1993) The Initial detection of Human Immunodeficiency virus 1 and its subsequent spread in Prostitutes in Tamil Nadu, India. J Acquir Immune Defic Syndr 6: 1030-4.
- Sinha A, Roy M (2008) An ICMR task force study of Prevention of Parent to Child Transmission (PPTCT) service delivery in India. Indian J Public Health 52: 200-202.
- Mandal S, Bhattacharya RN, Chakraborty M, Pal PP, Roy SG, et al. (2010) Evaluation of the prevention of parent to child transmission program in a rural tertiary care hospital of West Bengal, India. Indian J Community Med 35: 491-494.
- Parameshwari S, Jacob MS, Vijayakumari J, Shalini D, Sushi MK, et al. (2009) A Program on Prevention of Mother to Child Transmission of HIV at Government Hospital, Tiruchengode taluk, Namakkal district. Indian J Community Med 34: 261-263.
- Nagdeo N, Thombare VR (2007) Prevention of parent-to-child transmission of HIV: an experience in rural population. Indian J Med Microbiol 25: 425.
- Chaudhuri S, Mundle M, Konar H, Das C, Talukdar A, et al. (2010) Utilization of therapeutic intervention to prevent mother to child transmission of HIV in a teaching hospital in Kolkata, India. J Obstet Gynaecol Res 36: 619-625.<
- Joshi U, Kadri A, Bhojiya S (2010) Prevention of parent to child transmission services and interventions - coverage and utilization: A cohort analysis in Gujarat, India. Indian J Sex Transm Dis 31: 92-98.
- Ukey PM, Akulwar SL, Powar RM (2005) Seroprevalence of human immunodeficiency virus infection in pregnancy in a tertiary care hospital. Indian J Med Sci 59: 382-387.
- Arora P, Kumar R, Bhattacharya M, Nagelkerke NJ, Jha P (2008) Trends in HIV incidence in India from 2000 to 2007. Lancet 372: 289-290.
- Chibber R, Khurranna A (2005) Birth outcomes in perinatally HIV infected adolescents and young adults in Manipur, India: Anew frontier. Arch Gynecol Obstet 271: 127-131.