Research Article
Sen and Torque Teno Virus: Putative agents of Non-A-E Viral Hepatitis
Shafqat Jahan1, Meher Rizvi2, Mohd Azam2, Fatima Khan2*, Asfia Sultan2, Indu Shukla2, Abida Malik2, M R Ajmal3
1Department of Microbiology, Deen Dayal Upadhyay, Delhi, India
2Department of Microbiology, Jawaharlal Nehru Medical College, AMU, Aligarh, India
3Department of Medicine, Jawaharlal Nehru Medical College, AMU, Aligarh, India
Corresponding author: Dr. Meher Rizvi, Assistant Professor, Department of Microbiology, JNMCH, AMU, Aligarh, Tel:7060317021, India; E-mail: rizvimeher@yahoo.co.in
Citation: Jahan S, Rizvi M, Azam M, Khan F, Sultan A, et al. Sen and Torque Teno Virus: Putative agents of Non-A-E Viral Hepatitis. J Immunol VaccineTechnol. 2015;1(1): 104.
Copyright © 2014 Jahan S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Immunology and Vaccine Technology | Volume: 1, Issue: 1
Submission: 20/06/2015; Accepted: 27/07/2015; Published: 06/08/2015
Abstract
Introduction: The past few decades have witnessed formidable advances in the characterization of hepatotropic viruses of humans. A proportion ofacute and chronic hepatitis cases still remain that cannot be ascribed to Hepatitis A-E viruses or to other viruses like certain Enteroviruses, Adenoviruses,Parvovirus B19 etc. The TTV and the SEN viruses are often present in the serum of individuals at high risk of infection with bloodborne viruses. Knowledgeon TTV and SEN-V is growing fast, but many fundamental aspects remain to be elucidated. This study was undertaken to study the prevalence of TTV andSEN virus in patients with acute and chronic liver disease and to assess their role in liver disorders.
Methodology: The study was conducted in Jawaharlal Nehru Medical College and hospital over a period of two years. 135 patients of liver disorderwere included in the study. Screened was done for HAV, HCV, HEV IgM antibodies and HBV (anti HBsAg) by ELISA. Detection of TTV and SEN-V wasdone by nested PCR.
Statistical analysis: Statistical analysis was performed with the IBM SPSS Statistics 19.
Result: HBV was detected in 62(46%) cases. 34(25.2%) were positive for SEN virus, 20(15%) had TTV, 5(3.7%) had HEV, 3(2.2%) had HCV and1(0.7%) had HAV infection. TTV was detected in 1(3.3%) healthy control while SEN-V was not detected in any of the healthy controls. Isotype SEN-H wasdetected in 58% of SEN-V patients and SEN-D in 38%. AVH was the most common presentation of TTV (60%) and SEN-V (64.7%). Clinically fever andicterus were consistent findings along with ascitis and abdominal discomfort. MELD score was greater than normal almost unvaryingly in all these patients.
Conclusion: Our study points to a greater potential of SEN-V in causing hepatitis compared to TTV.
Keywords: Torque Teno Virus; SEN- Virus; Viral Hepatitis Non-A-E; Liver Disorders
Introduction
The past few decades have witnessed formidable advances inthe characterization of hepatotropic viruses of humans, with thediscovery of five major hepatitis viruses (A-E) and the developmentof sensitive detection methods for each. However, a relatively smallproportion of acute and chronic hepatitis cases still remain that cannot be ascribed to these viruses or to other viruses like certainEnteroviruses, Adenoviruses, Parvovirus B19 etc.
While attempting to shed light on these forms, Nishizawa et al.,in 1997 [1], first identified Torque Teno Virus (TTV) in Japanesepatients who exhibited elevated alanine amino-transaminase (ALT)levels following transfusions. It is a single stranded DNA virus belonging to the Anelloviridae family [2]. At least four genotypes havebeen described, of which genotype 1 is the most prevalent [3]. Thevirus has a global distribution.
In 1999, a previously unidentified DNA virus was detected in theblood of a human immunodeficiency virus (HIV) infected injectiondrug user and named SEN virus (SENV). SENV is distantly relatedto the large TTV family [4]. SENV earlier belonged to the familyCircoviridae, genus Anellovirus, a group of small, single-stranded,non-enveloped circular DNA viruses. SENV, TTV and TTV-like miniviruses TUS01, SANBAN and YONBAN may have evolved from acommon ancestor [5]. Recent changes in nomenclature have classifiedAnelloviruses capable of causing human infection into alpha torquevirus (Torque Teno virus, TTV), beta torque virus (Torque Teno-likemini virus, TTMV) and gamma torque virus (torque teno-like midivirus, TTMDV) genera of the other Anelloviridae family of viruses[6]. SENV has a strong association with transfusion transmitted nonA-E hepatitis [7]. The prevalence of SEN virus in serum samples ofotherwise healthy persons in different geographical regions rangesfrom 1.8% in the United States to 28.6% in Japan [8-10]. As many as30% of blood transfusion recipients have SEN virus in their serum[4], with a significant association between transfusion volume andthe occurrence of SEN virus infection [8]. Eight genetic variants ofthe virus (A-H) have been described, each differing from the othersby more than 25% of the total nucleotide sequence [11] but only twoof these variants (SEN virus-D and SEN virus-H) have a significantassociation with transfusion-transmitted hepatitis and chronic liverdisease [11].
The TT virus has been detected in the serum of patients with non-A-E fulminant hepatitis, chronic hepatitis, cirrhosis and HCC [12].Despite its presence in the serum of individuals with a number ofconditions and in a variety of circumstances, there is no unequivocalevidence that TTV causes hepatitis [13]. Knowledge on TTV andSEN-V is growing fast, but many fundamental aspects remain to beelucidated. This study was undertaken to study the prevalence of TTVand SEN virus in patients with acute and chronic liver disease and toassess their role in liver disorders.
Material and Methods
A prospective study was carried out on individuals presentingwith clinical hepatitis at Jawaharlal Nehru Medical College andhospital, AMU, Aligarh during January 2010 to June 2011.
Study Group
A total of 135 patients of liver disorder [90 acute viral hepatitis(AVH) cases, 18(13.3%) chronic viral hepatitis (CVH), 9(6.7%)fulminant hepatic failure (FHF) cases, 17(12.6%) liver cirrhosis (LC)cases and 1(0.7%) hepatocellular carcinoma (HCC)] were includedin the study. Patients with autoimmune liver disease, drug-inducedhepatitis and alcoholic liver injury were excluded. The cases wererecruited from Gastroenterology clinic and wards after informedconsent. All the cases were subjected to detailed history, clinicalexamination and investigations. The study protocol was approvedby the Institutional Ethical Committee of Jawaharlal Nehru MedicalCollege.
Model end stage liver disease (MELD) score was calculated.Formula for calculating MELD score was as follows: MELD Score =10 {0.957 LN (S. creatinine mg/dl) + 0.378 LN (T bilirubin mg/dl)+ 1.12 LN (International normalized ratio) + 0.643}[14]. The fourMELD levels were: greater than or equal to 25, 24-19, 18-11, less thanor equal to 10 on the basis of which patients were classified as severe,modertae, mild and normal. The results were further confirmedusing the MELD calculator at http://www.unos.org/resources/MELDcalculator [15].
Healthy Controls
The control group comprised of 30 healthy voluntary blooddonors of comparable age among which 22 (73.3%) were men and8 (26.7%) women; mean age being 37 years ± 3.8.1 These individualswere negative for HBsAg as well as for anti-HCV and anti-HIVantibodies.
Serological investigations
Blood samples (10 ml) were collected in DNAase free containers,taking all aseptic precautions. Serum was separated and stored at-80 °C until use. All the patients were screened for IgM anti-HAVantibodies (DRG International Inc., USA), HBsAg (SD Bio standarddiagnostic,India), IgManti-HCV antibodies (J. Mitra& Co. Pvt. Ltd.,India), IgM anti-HEV antibodies (M.B.S.S.R.L.Medical BiologicalService, Milano).
Other Investigations
Liver function and kidney function tests along with prothrombintime and international normalized ratio (INR) were performed.Specific investigations like ultrasonographic examination of liver,upper GI endoscopy and liver biopsy were performed whereverfeasible.
DNA Extraction
Total DNA from 100 μl serum was extracted by standard phenolchloroform isoamyl alcohol method [16]. The extracted DNA wassubjected to PCR for amplification of SEN V DNA and TTV DNAusing Labnic thermal cycler (MJ Research Inc., USA)
Detection of SEN virus and its genotypes SENV-D andSENV-H DNA
SEN virus-DNA (349 bp) was detected using nested-PCR proceduresspecific for the detection of specific sequences for SENvirus and its genotypes SENV-D (193bp) and SENV-H (118bp)[17]. The sequences of primers are as follows: SEN-V commonprimers: SP1-5’ TWCYCMAA CGACCAGCTAGACCT3’;SP2-5’GTTTGTGGTGAGCAGAACGGA3’. SENV-D primers:SP3-5’CTAAGCAGCCCTAACACTCATCCAG-3’; SP4-5’GCAGTTGACCG CAAAGTTAC AAGAG3’. SENV-H primers:SP5-5’TTTGGCTGCACCTTCTGGTT3’; SP6-5’ AGAAAT GATGGGTGAGTGTTAGGG3’.(W=A/T, Y=C/T, M=A/C)
The outer PCR for SEN-V was carried out with a reaction mixtureconsisting of 12.5 μl of 2x PCR master mix (MBI Fermentas, USA)containing 0,05 units/μlTaq DNA polymerase in reaction buffer, PCRbuffer, 4mM MgCl2, 0.4mM dATP, 0.4mM dCTP, 0.4mM dGTP and 0.4mM dTTP, 5 pmol concentration of SP1 and SP2 primers and 5μl DNA sample. The reactions consisted of preheating at 94 °C for4 min, 40 cycles of denaturation at 94 °C for 15 sec, annealing at 55°C for 50 sec, extension at 72 °C for 50 sec, and a final at 72 °C for7 min. The first nested PCR for SENV D was carried out with thesame reaction mixture with SP3 and SP4 primers and 5 μl outer PCRproduct. The second nested PCR for SENV H was carried out withthe same reaction mixture used as above with SP5 and SP6 primesand 5 μl outer PCR product. Cycling conditions were the same as forSEN-V for both SENV D and SENV H.
TTV DNA Detection
16S rRNA genes were targeted for amplification of TTV specificnucleic acid by nested PCR. Primers were synthesized from Operon,Germany (Genetix).
First set of primers wereNS1 5’-GGGTGCCGAAGGTGAGTTTAC-3’, NS2 5’-GCGGGGCACGAAGCACAGAAG-3’ while secondset of primers were: NS3 5’-AGTTTACACACCGAAGTCAAG-3’and NS4 5’-AGCACAGAAGCAAGATGATTA-3’ as described byBiagini et al., [18].
Fluorescent Antibody Test (FAT)
The first round PCR was carried out for 40 cycles with pre heatingof 96 °C for 2 min., each cycles consisting of denaturation at 94 °C for15 seco, primer annealing at 55 °C for 45 sec and extension at 72 °Cfor 45 sec, followed by an additional extension at 72 °C for 7 min in asolution containing NS1(5pmol), NS2(5pmol), DNA Template(5μl),nuclease free water (3μl), 2x PCR master mix (10μl).The secondround PCR was carried out for 40 cycles, each cycles consistingof denaturation at 94 °C for 15 sec, primer annealing at 50 °C for45 sec and extension at 72 °C for 45 sec, followed by an additionalextension at 72 °C for 7 min in a solution containing NS1 (5pmol),NS2 (5pmol), PCR Product (2μl), nuclease free water (6μl), 2x PCRmaster mix (10μl). The 2x PCR master mix contained the reagents asdescribed above.
Amplified PCR products (5 μl) were subjected to electrophoresisand visualized under Gel Documentation systems (Biorad, USA).
Statistical analysis
Statistical analysis was performed with the IBM SPSS Statistics19. Results were expressed as means ± standard deviation or aspercentages. Means were compared between groups by using the t–test, and frequency distributions were compared by using the chisquaretest. Wilcoxon sign ranked test and Mann Whitney U testwere the non parametric tests used for non-normally distributed data.
Results
One-hundred and thirty five patients of liver disease, eitheradmitted in Medicine wards or attending the outpatient Departmentand Gastroenterology clinic, along with thirty healthy age and sexmatched controls were included in the study. The age distributionrevealed that maximum number 28.88% were in the age group 21-30years. The mean age distribution was 33.90±18.15 years in the studygroup and 40.2±6.42 years in controls. Overall male to female ratiowas 2.8:1.
Hepatitis A-E, TTV and SEN-V prevalence in patients with liver diseases and in healthy controls
HBV was most prevalent with 62(46%) cases. A statisticallysignificant number 34(25.18%, 95% CI: 20.1-30.3) were positivefor SEN virus (p< 0.01) (Figure 1). Prevalence of TTV was lower at20(15%, 95% CI: 10.8-19.2) (Figure 2). A much lower prevalence wasobserved for HEV 5(3.7%), 3(2.2%) for HCV and 1(0.7%) for HAV(Graph 1). TTV was detected in 1(3.3%) healthy control while SEN-Vwas not detected in any of the healthy controls.
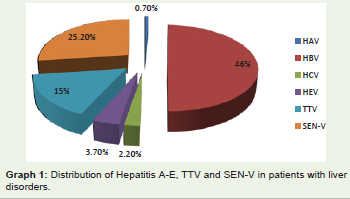
Graph 1: Distribution of Hepatitis A-E, TTV and SEN-V in patients with liver disorders.
Figure 1: Amplification of PCR products for SEN-V detection.
Figure 2: 2,3,5,6- Showing amplified TTV(295bp) DNA, 1- 100bp DNAladder,4-negative control.
Graph 2 shows the distribution of HBV, TTV and SEN-V amongthe different categories of liver diseases. Out of 62 HBV positivepatients, 32(51.6%) had AVH, 9(14.5%) had CVH, 14(22.6%) hadcirrhosis, 6(9.7%) had FHF and 1(1.6%) had HCC. Among 20 TTVpatients 60% were in the age group 20-40 years and most of them12(60%) suffered from AVH, 5(25%) had CVH, 2(10%) had cirrhosisand 1(5%) had FHF.
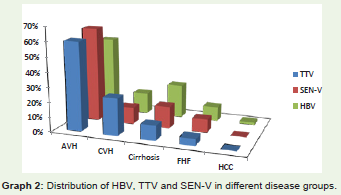
Graph 2: Distribution of HBV, TTV and SEN-V in different disease groups.
Among the 34 SEN-V positive patients 55.2% were in the agegroup 20-40 years. Most of the SENV positive patients had AVH22(64.7%), 4(11.4%) had CVH, 5(14.7%) had cirrhosis and 3(8.8%)from FHF (Graph 2 ). On genotyping, the prevalence of SEN-D andSEN-H isotypes was found to be 38% and 58% respectively (Figure 3,4). 85% of SEN-D positive patients had AVH, while 15% had CVH.Among SEN-H positive patients AVH was noted in 53% followed bycirrhosis, FHF and CVH in 26%, 16% and 5% respectively.
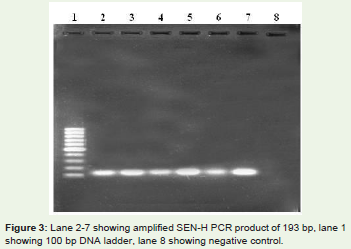
Figure 3: Lane 2-7 showing amplified SEN-H PCR product of 193 bp, lane 1showing 100 bp DNA ladder, lane 8 showing negative control.
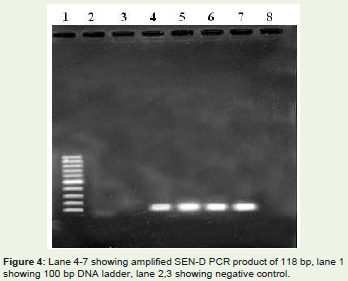
Figure 4: Lane 4-7 showing amplified SEN-D PCR product of 118 bp, lane 1showing 100 bp DNA ladder, lane 2,3 showing negative control.
Clinical and biochemical profile of patients with TTV andSEN-V infection
Amongst the TTV and SEN-V positive patients, fever was the most common presenting complaint (85% and 79% respectively).The other significant complaints on presentation were weight loss,abdominal discomfort and high coloured urine. On examination,icterus was present in 90% of TTV and 82% of SEN-V positivepatients. Ascitis and splenomegaly was more common in patientspositive for TTV (67% and 60% respectively) than the SEN-V positivepatients (26% and 12% respectively).
On analyzing liver function tests of the TTV positive patients,majority (60%) had deranged AST and ALT level. 70% of the patientshad deranged INR and MELD score greater than normal. Among theSEN-V positive patients 73.5% had deranged AST level and 79.4%had deranged ALT levels. INR was deranged in 76.5% patients andalmost all the SEN-V positive (97%) patients had MELD score higherthan normal (Table 1,2).
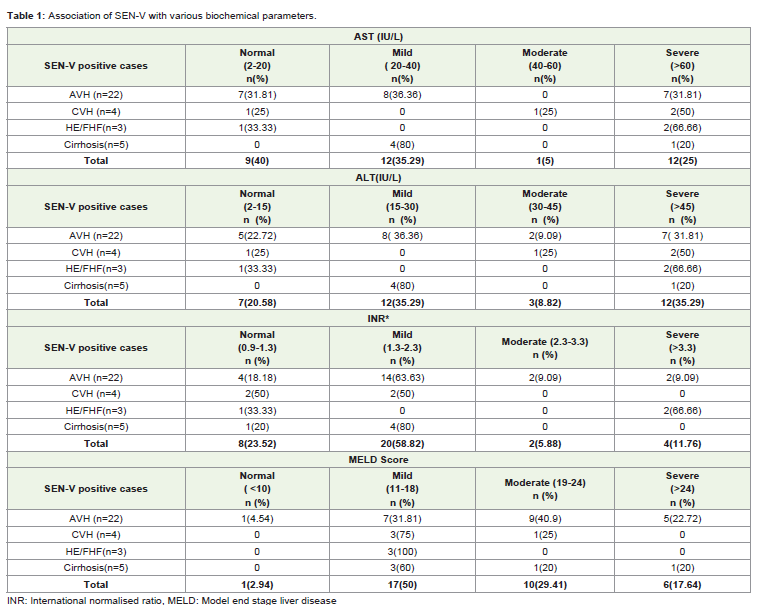
Table 1: Association of SEN-V with various biochemical parameters.
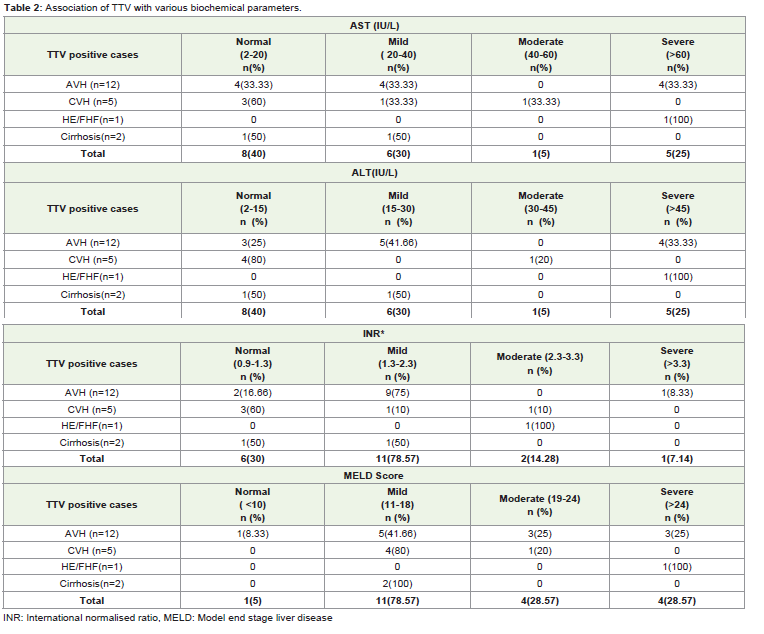
Table 2: Association of TTV with various biochemical parameters.
Co-infection of TTV and SEN-V with Hepatitis A-E
Co-infection of TTV and SEN-V was highest with HBV (55%/44%for SENV and TTV). HCV co-infection was found in 5% and 6%of TTV and SENV positive cases and for HEV it was 10% and 11%respectively. None of the TTV or SENV positive cases was co-infectedwith HAV. Co-infection of TTV with SENV was noted in 5(14.7%)patients (Table 3).
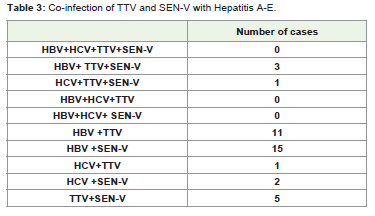
Table 3: Co-infection of TTV and SEN-V with Hepatitis A-E.
Discussion
Despite the five known hepatitis viruses (A-E) 5-30% patients stillpresent with acute and chronic hepatitis of unknown origin (NonA-E hepatitis). TTV and SEN-V are being considered as putativeagents of post-transfusion non A-E hepatitis [4,19]. However, theexact role of these viruses in the pathogenesis of liver diseases stillremains unclear.
TTV viremia is an extremely frequent occurrence in apparentlyhealthy individuals worldwide, a feature so unusual among virusesthat it has even been proposed that TTV might be a commensalvirus [20]. In our study, prevalence of TTV in liver disease patientswas 15% and 3.3% in healthy controls. A relative high prevalence ofTTV DNA in liver diseases, in comparison to the healthy personssuggests that TTV might play an important role in causation of liverdisease. Report by Irshad et al. [21] demonstrated little role of TTVin causation of liver diseases. Several studies have revealed high (1.9to 36%) TTV DNA prevalence in healthy control groups [22-24].Its prevalence in healthy populations in India is lower than thosepreviously reported for Turkish (51.6%), Japanish (92.0%) and Polish(78%) blood donors [21].
Prevalence of SEN-V in our study was higher (25.2%) than TTVamongst the liver disease patients while none of the controls wasfound positive for SEN-V. Prevalence of SEN-V reported in previousstudies, for SEN-V DNA ranged from 17 to 92% in patients with liverdisease [8]. The explanations for these differences are unknown, butthey may result from interactions between behavioral, social andbiological factors.
A notable finding among the TTV and SEN-V positive patientswas that they were associated with significant morbidity. Fever andicterus were a consistent finding in these patients, along with ascitisand abdominal discomfort. Most of the patients with TTV and/or SEN-V infection had raised ALT, AST and INR levels. MELD scorewas greater than normal almost unvaryingly in all these patients.Abnormality in the liver functions along with clinical manifestationspoint to a possible role of these viruses in the pathogenesis of liverdisorders. Such type of analysis has not been done in previous studies.
To assess the role of these two viruses in the causation of liverdisease we compared the clinical presentation of TTV and SEN-V toHBV. It was noted that the most common presentation of all the threeviruses was AVH (60%, 64.7% and 51.6% for TTV, SEN-V and HBVrespectively). A significant finding of our study was that CVH wasmore common in patients with TTV infection, while patients withSEN-V had higher rates of cirrhosis. However there may be other yetundiscovered viruses which may be actual cause of hepatitis and SENand TTV may be simply bystanders.
Conclusions
Our study points to a greater potential of SEN-V in causinghepatitis compared to TTV. SEN-D was associated with AVH whileSEN-H was more prevalent in CVH cases. In future longitudinalstudies with larger sample size will further elucidate the role of theseviruses in causation of AVH and CVH.
Acknowledgements
Authors are great full to Joint Director, Academic and Director of Indian Veterinary Research Institute for the support. This research work was in part funded under the Project “Niche area of Excellence on Vaccines and Diagnostics”.
References
- Nishizava T, Okomata H, Konishi K, Yoshizawa H, Miyakawa Y, et al. (1997) A novel DNA virus (TTV) associated with elevated transaminase levels in posttransfusion hepatitis of unknown etiology. Biochem Biophys Res Commun 241: 92- 97.
- 2.Jelcic I, Holtz-Wagenblattt A, Huzaiker A, Zurhausen H, De Villiers EM (2004) Isolation of multiple TT virus genotypes from spleen biopsy tissue from a Hodgkin's disease patient: genome re-organization and diversity in the hypervariable region. J Virol 8: 7498-7507.
- Diniz-Mendez L, DeValle S, Niel C (2004) Genomic characterization of a Brazilian TT virus isolate closely related to SEN virus F. Mem Inst Oswaldo Cruz 99: 301-306.
- Matsumoto A, Yeo AET, Shih JW, Tanaka E, Kiyosawa K, et al. (1999) Transfusion-associated TT virus infection and its relationship to liver disease. Hepatology 30: 283-288.
- Hino S (2002) TTV, a new human virus with single stranded circular DNA genome. Rev Med Virol 12: 151-158.
- Biagini P (2009) Classification of TTV and related viruses (anelloviruses). Curr Top Microbiol Immunol 331: 21-33.
- Umemura T, Donahue P, Sottini A, et al. (2000) SEN virus infection and its relationship to transfusion-associated hepatitis. Anti vir Ther 5(Suppl ):11.
- Viazov S, Ross RS, Varenholz C, Lange R, Holtmann M, et al. (1998) Lack of evidence for an association between TT infection and severe liver disease. J Clin Virol 11: 183-187.
- Tanaka H, Okamoto H, Luengrojanakul F, Chainuvati T, Tsuda F, et al. (1998) Infection with an unenveloped DNA virus (TTV) associated with posttransfusion non-A to G hepatitis patients and healthy blood donors in Thailand. J Med Virol 28: 839-842.<
- Jeon MJ, Shin JH, Suh SP, Lim YC, Ryang DW (2003) TT virus and hepatitis G virus infections in Korean blood donors and patients with chronic liver disease. World J Gastroenterol 9: 741-744.
- Unemura T, Yeo AE, Sottini E, Moratto D, Tanaka Y, et al. (2001) SEN virus infection and its relationship to transfusion-associated hepatitis. Hepatology 33: 1303-1311.
- Mikuni M, Moriyama M, Tanaka N, Abe F, Arakawa Y (2002) SEN virus infection does not affect the progression of non-A to-E liver disease. J Med Virol 67: 624-629.
- Charlton M, Adjei P, Poerucha J, Zein N, Moore B, et al. (1998) TT virus infection in North American blood donors, patients with fulminant hepatic failure, and cryptogenic cirrhosis. Hepatology 28: 839-842.
- Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Therneau TM, et al. (2001) A model to predict survival in patients with end-stage liver disease. Hepatology 33: 464-470.
- MELD Calculator.
- Saiki RK, Gelfand DH, Stoffel S, Scharf SJ, Higuchi R, et al. (1988) Primer-directed enzymatic amplification of DNA with a thermostable DNA polymerase. Science 239: 487-491.
- Tang ZH, Chen XH, Yu YS, Zang GQ (2008) Prevalence and clinical significance of SEN virus infection in patients with non A-E hepatitis and volunteer blood donors in Shanghai. World J Gastroenterol 14: 4204-4208.
- Biagini P, Gallian P, Attoui H, Cantaloube JF, de Micco P, et al. (1999) Determination and phylogenetic analysis of partial sequences from TT virus isolates. J Gen Virol 80: 419-424.
- Abe K, Inami T, Asano K, Miyoshi C, Masaki N (1999) TT virus infection is widespread in the general populations from different geographical regions. J Clin Microbiol 37: 27-35.
- Simmonds P, Prescott LE, Logue C, Davidson F, Thomas AE, et al. (1999) TT-virus part of the normal human flora? J Infec Dis 180: 1748-1750.
- Irshad M, Sharma Y, Dhar I, Singh J, Joshi YK (2008) Torque teno virus: Its prevalence and isotypes in North India. World J Gastroenterol 14: 6044-6051.
- Naoumov NV, Petrova EP, Thomas MG, Williams R (1998) Presence of a newly described human DNA virus (TTV) in patients with liver disease. Lancet 352: 195-197.
- Ikeda H, Takasu M, Inoue K, Okamoto H, Miyakawa Y, et al. (1999) Infection with an unenveloped DNA virus (TTV) in patients with acute or chronic liver disease of unknown etiology and in those positive for hepatitis C virus RNA. J Hepatol 30: 205-212.
- Saback FL, Gomes SA, de Paula VS, da Silva RRS, Lewis-Ximmenez LL, et al. (1999) Age-specific prevalence and transmission of TT virus. J Med Virol 59: 318-322.