Review Article
Non-Polio Enterovirus D68 (EV-D68):Implications and Therapeutic Challenges
Farrukh Naz, Adria Hasan, Roohi, Snober S. Mir*
Department of Bioengineering, Integral University, Lucknow, India
Corresponding author: Snober S Mir, Associate Professor, Department of Bioengineering, Integral University, Lucknow,India.; E-mail: smir@iul.ac.in, snobermir@gmail.com
Citation: Naz F, Hasan A, Roohi, Mir SS. Non-Polio Enterovirus D68 (EV-D68): Implications and Therapeutic Challenges. J Enzymol Metabol. 2016;2(1):106.
Copyright © 2016 Snober SM, etal. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Enzymology and Metabolism | Volume: 2, Issue: 1
Submission: 07/05/2016; Accepted: 07/05/2016; Published: 13/06/2016
Abstract
Enterovirus D68 (EV-D68) is being reported as a cause of respiratory illness across USA along with some parts of Canada. Nonpolio EV-D68 has been associated with respiratory illness followed by acute flaccid paralysis in children which clearly suggests that thereshould be appropriate screening and treatment of EV-D68 virus. Thus, this review aims to highlight recent research on EV-D68 virus alongwith its symptoms, diagnosis, possible therapy and associated challenges.
Keywords: Enterovirus; EV-D68; Respiratory illness; Pleconril
Introduction
Enterovirus is positive strand single stranded RNA virusbelonging to family picornavirus. The genome of enterovirus is madeup of approximately 7500 bases [1]. So far, 71 human serotypes ofenterovirus have been established by antibody neutralization tests [2].The illustration of human enterovirus according to their species andserotypes is given below in Figure 1.
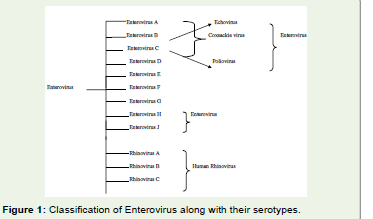
Figure 1: Classification of Enterovirus along with their serotypes.
Enteroviruses are the most common microorganisms affectingmillions of humans all over the world. These viruses are generallyfound either in the respiratory tract or stool of the infectedperson. Although polio is the most common disease caused byenterovirus, now many other diseases are also caused by them.Some of these include nonspecific febrile illness, Pericarditis and/or myocarditis, Acute hemorrhagic conjunctivitis, Herpangina,aseptic meningitis, myocarditis, severe neonatal sepsis-like disease,and acute flaccid paralysis [3].
In this review our focus is on Human Enterovirus D68 (EVD68).In 1962, EV-D68 was isolated from samples of four children inCalifornia who were suffering from bronchiolitis and pneumonia [4].
EV-D68 and human rhinovirus are biologically similar due toits acid-labile nature and also because of association of EV-D68 withrespiratory disease, 26 isolates of EV-D68 were reported from 1970 to2005 in USA [5]. However, outbreaks of EV-D68 have been reportedin Japan, Netherlands and some areas of USA for the past three yearsadding EV-D68 as a new respiratory pathogen [6-8].
Enterovirus D68 mostly cause respiratory tract infection inchildren. Structure of Enterovirus consists of icosahedra which isapproximately 30nm in diameter. Enteroviruses divide well at 37 °C,under acidic conditions (pH 3.0) although EV-D68 grows optimallyat 33 °C and cannot tolerate an acidic environment [9]. Virus canenter the upper respiratory tract of a person either through directinhalation of aerosolized particles or by transmission of contaminatedmaterial through the transfer of infected material from environment.As soon as the virus reaches the upper respiratory tract and attachesitself to the epithelial cells of the mucosal surfaces, it starts to spread Figure 2 Figure 3.
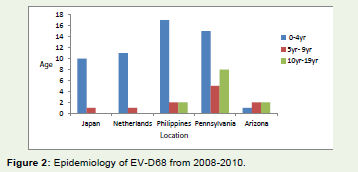
Figure 2: Epidemiology of EV-D68 from 2008-2010.
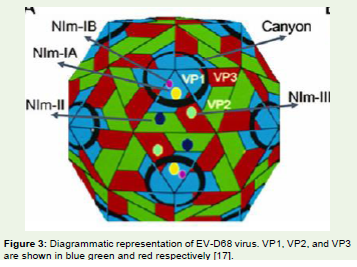
Figure 3: Diagrammatic representation of EV-D68 virus. VP1, VP2, and VP3are shown in blue green and red respectively [17].
Recently in USA, outbreak of EV-D68 was observed whichwas thought to cause respiratory problems. The state public healthlaboratories in USA asserted that in at least 49 states, 1,153, and in theDistrict of British Columbia, EV-D68 has caused respiratory illnessfrom mid-August 2014 to January 15, 2015. Most of the cases of EVD68were found in children who already suffered from asthma or anyother respiratory disease [10].
Another case was reported in British Columbia in which a 9year old patient suffered from acute flaccid paralysis of his left armfollowed by respiratory illness and fever. In this case also, EV-D68 wasthe causative agent which was isolated in nasopharyngeal specimenand intravenous immunoglobulin was used to treat the patient. Still,the patient did not recover the full function of his left arm. This caseclearly shows the importance to screen and treat polio and non-polioenteroviruses [11].
Disease Caused by Different Serotypes of Enterovirus
Coxsackie and echovirus: Coxsachie viruses mainly cause hand,mouth and foot diseases. More serious diseases can also be causedby Coxsackie B virus like myocarditis, pericarditis, pancreatitis, andmeningitis. Echoviruses can cause many viral infections and areusually found in intestine. Nervous disorders can be caused by thisvirus. The symptoms of this virus include fever, upper respiratorytract illness, and mild rash [12].
Enterovirus 71: This virus mainly causes mouth, hand, andfoot diseases but can also cause central nervous system disease [13].Isolation and characterization of EV71 was first done in Californiaform neurological cases [14]. It is still not known that how thehost response to EV71 infection but increases in mRNAs encodingchemokines, pro-apoptosis proteins, degradation of proteins, andcomplement proteins have been reported [15].
Poliovirus: Three serotypes of poliovirus have been reportednamely, PV1, PV2, and PV3. The difference between these serotypeslies in their caspid proteins. Polio virus affects spinal cord and causespoliomyelitis [16].
Structure of EV-D68: The protein shell of enterovirus also known as capsid is made up of four different viral proteins namely VP1,VP2, VP3 and VP4. The proteins VP1, VP2, and VP3 have “jelly rollâ€folding and are arranged in the capsid with pseudo T=3 icosahedralsymmetry where T is triangulation number. An extended peptide onthe inner surface of the capsid is formed by VP4. Enteroviruses alsoconsist of deep surface depression around each of twelve pentamericvertices. This deep surface depression also known as canyon is alsosaid to be the receptor binding site. The external surface of the virusconsists of exposed amino acids which can bind to the antibodies.This makes the virus accessible to specific receptor molecule that canbind to the canyon and can easily evade the host’s immune response[17].
Most contagious enteroviruses also have a “pocket factorâ€,usually a fatty acid in the VP1 site. Pocket factor also helps in thestabilization of the virus by filling the hydrophobic pocket of VP1.This leads to virus stabilization when it is being transferred to a newhost. Although, when the receptor molecule binds to the canyon, thefloor is depressed squeezing the binding pocket and throwing outthe pocket factor. Thus, when a virus attaches itself to the host cellsurface, it initiates uncoating leading to the loss of the genome intothe cell’s cytosol [17].
When the host cell is infected, the genome gets translated intoa single polyprotein. The virus encoding proteases further convertpolyprotein to form capsid proteins and nonstructural proteinswhich help in replication of the virus [18].
Symptoms of EV-D68 infection: Mild symptoms may beincluding runny nose, sneezing, cough, body and muscle aches. Severesymptoms may be including wheezing and difficulty breathing. EVD68causes respiratory illness, the virus can be found in an infectedperson’s respiratory secretions, such as saliva, nasal mucus [19].
Detection: A duplex real-time RT-PCR for rapid screening of EV-D68 was developed. The method targeted the 50 non-translatedregions (NTR) of the HEV genome at a location generally used forenterovirus detection [19].
Proposed therapy for treatment of EV-D68 caused illness: Aflow of EV-D68 cases can be found in past few years and is said to bethe cause of respiratory illness in children. There has been spread ofEV-D68 in the past few years thought the world [20]. In august 2014there have occurred thousand of respiratory illness cases in the U.Samong children of which 1116 were caused by EV-D68.The virus isthe cause of neurological infection as well. Inspite of being big globalthreat, there is no vaccine or effective antiviral treatment [21]. OnOctober 4, 2014, one death due to enterovirus 68 in New Jersey, USAhas been reported. Pleconaril is being tested to treat cases of illnesscaused by EV-D68 [21]. A caspid binding compound, pleconarilwhich is an anti-rhinovirus drug is now being used to treat diseasecaused due to EV-D68. Pleconaril inhibits EV-D68 therefore it is apossible drug that prevents the outbreaks of EV-D68.
It is reported the crystal structures of EV-D68 forms a complexwith pleconaril, a capsid binding compound that had been developedas an anti-rhinovirus drugs. The hydrophobic drug binding pocket inviral protein 1(VP1) contained density that is reliable with a fatty acidof on 10 carbon atoms. This density could be displaced by pleconaril.It was also shown that pleconaril inhibits EV-D68 at a half maximaleffective concentration (EC50) of 430 nM and might, therefore, is apossible drug candidate to alleviate EV-D68 outbreaks [17].
The anti-EV-D68 activity of 2 capsid binding compounds,pirodavir and BTA-188, that had important anti-rhinovirus activitywere compared with pleconaril use plaque reduction assays in HeLacells. The 0.5 peak effective concentration, EC50, value of those2 compounds were found to be similar to previous results usingcytopathic inhibition assays against EV-D68 [22]. However, pleconarilwas found to be more potent against EV-D68 than pirodavir andBTA-188. The suppressive impact of pleconaril is comparable againstEV-D68, HRV16, and HRV14 however it is better than against EVA71.Therefore, pleconaril can be used as a potential drug againstintensive clinical cases for treatment of respiratory illness [23].Moreover, fluorescence-based thermal stability assays indicated thatonce EV-D68 was incubated with 10 μg/ml or 50 μg/ml pleconaril, 4°C higher temperatures were needed to unleash the RNA. Thereforepleconaril stabilizes EV-D68 capsids, preventing the virus fromuncoating its RNA. Thus, these data suggest that pleconaril can beused as a potential drug to treat illness caused by EV-D68 [17].
Conclusion
EV-D68 is a virus that causes respiratory illness in children.Although the first case of EV-D68 was reported in 1962, recently anoutbreak of EV-D68 was reported one of the major cases was of a 9 yearold boy in British Columbia, who suffered from partial paralysis dueto EV-D68. Apart from this case, there are other cases of respiratoryillness along with the association with neurological complications.Another factor which proves that this virus is lethal is that itsoccurrence has been observed in different countries over a period oftime suggesting that this virus can cause worldwide epidemic. Thus, itis necessary to screen EV-D68 in children as well as adults and to find possible drugs for its treatment. Continuous diagnosis of EV-D68 isimportant to prevent its outbreak. Furthermore, if a link is confirmedbetween EV-D68 and several other diseases (example: paralysis),finding new therapeutic advances for this disease is need of the hourto prevent mortality caused by EV-D68.
References
- Li L, He Y, Yang H, Zhu J, Xu X, et al. (2005) Genetic Characteristics of Human enterovirus 71 and coxsackievirus A16 circulating from 1999 to 2004 in Shenzhen, People's Republic of China. J Clin Microbiol 43: 3835-3839.
- Oberste MS, Maher K, Kilpatrick DR, Pallansch MA (1999) Molecular evolution of the human enteroviruses: correlation of serotype with VP1 sequence and application to picornavirus classification. J Virol 73: 1941-1948.
- Non-Polio Enterovirus Infections. CDC. 8 September 2014. Retrieved 9 September 2014.
- Schieble JH, Fox VL, Lennette EH (1967) A probable new human picornavirus associated with respiratory diseases. Am J Epidemiol 85: 297-310.
- Khetsuriani N, Lamonte-Fowlkes A, Oberst S, Pallansch MA, Centers for Disease Control and Prevention (2006) Enterovirus surveillance-United States, 1970–2005. MMWR Surveill Summ 55: 1-20.
- Jacobson LM, Redd JT, Schneider E, Lu X, Chern SW, et al. (2012) Outbreak of lower respiratory tract illness associated with human enterovirus 68 among American Indian children. Pediatr Infect Dis J 31: 309-312.
- Hasegawa S, Hirano R, Okamoto-Nakagawa R, Ichiyama T, Shirabe K (2011) Enterovirus 68 infection in children with asthma attacks: virus-induced asthma in Japanese children. Allergy 66: 1618-1620.
- Imamura T, Fuji N, Suzuki A, Tamaki R, Saito M, et al. (2011) Enterovirus 68 among children with severe acute respiratory infection, the Philippines. Emerg Infect Dis 17: 1430-1435.
- Oberste MS, Maher K, Schnurr D, Flemister MR, Lovchik JC, et al. (2004) Enterovirus 68 is associated with respiratory illness and shares biological features with both the enteroviruses and the rhinoviruses. J Gen Virol 85: 2577-2584.
- Report from Centers for Disease Control and Prevention, USA.
- Sherwood MD, Gantt S, Connolly M, Dobson S (2014) Acute flaccid paralysis in a child infected with enterovirus D68: A case report. BCMJ 56: 495-498.
- Santti J, Heli H, Leena K, Timo H (2000) Molecular epidemiology and evolution of coxsackievirus A9. J Gen Virol 81: 1361-1372.
- Lin TY, Chu C, Chiu CH (2002) Lactoferrin inhibits enterovirus 71 infection of human embryonal rhabdomyosarcoma cells in vitro. J Infect Dis 186: 1161-4.
- Wang SY, Lin CL, Sun HC, Chen HY (1999) Laboratory Investigation of a Suspected Enterovirus 71 Outbreak in central Taiwan. Epidemiol Bull 215- 219.
- Shih SR, Stollar V, Lin JY, Chang SC, Chen GW, et al. (2004) Identification of genes involved in the host response to enterovirus 71 infection. J Neurovirol 10: 293-304.
- Paul JR (1971) A History of Poliomyelitis (Yale studies in the history of science and medicine). New Haven, Conn: Yale University Press.
- Liu Y, Sheng J, Fokine A, Meng G, Shin WH, et al. (2015) Structure and inhibition of EV-D68, a virus that causes respiratory illness in children. Science 347: 71-74.
- Merkle I, van Ooij MJ, van Kuppeveld FJ, Glaudemans DH, Galama JM, et al. (2002) Biological significance of a human enterovirus B-Specific RNA element in the 3′ Nontranslated region. J Virol 76: 9900-9909.
- Bragstad K, Jakobsen K, Rojahn AE, Skram MK, Vainio K, et al. (2015) High frequency of enterovirus D68 in children hospitalised with respiratory illness in Norway, autumn 2014. Influenza Other Respir Viruses 9: 59-63.
- Tokarz R, Firth C, Madhi SA, Howie SRC, Wu W, et al. (2012) Worldwide emergence of multiple clades of enterovirus 68. J Gen Virol 93: 1952-1958.
- Kreuter JD, Barnes A, McCarthy JE, Schwartzman JD, Oberste MS, et al. (2011) A fatal central nervous system enterovirus 68 infection. Arch Pathol Lab Med 135: 793-6.
- Barnard DL, Hubbard VD, Smee DF, Sidwell RW, Watson KGW, et al. (2004) In vitro activity of expanded-spectrum pyridazinyl oxime ethers related to pirodavir: novel capsid-binding inhibitors with potent antipicornavirus activity. Antimicrob Agents Chemother 48: 1766-1772.
- Hayden FG, Herrington DT, Coats TL, Kim K, Cooper EC, et al. (2003) Efficacy and safety of oral pleconaril for treatment of colds due to picornaviruses in adults: results of 2 double-blind, randomized, placebo-controlled trials. Clin Infect Dis 36: 1523-32.