Angiomyxoma of the Vulva
Kant A*
Asian Institute of Medical Sciences, India
Corresponding author: Kant A, Asian Institute of Medical Sciences, Faridabad, India, Tel no: 96500099057/9910114284; Fax: +911294143716; E-mail: anita.kant@aimsindia.com
Citation: Kant A. Angiomyxoma of the Vulva. J Cancer Res Molecul Med. 2019;4(1): 105.
Copyright © 2019 Kant A. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Cancer Research and Molecular Medicine | Volume: 4, Issue: 1
Submission: 14/12/2018; Accepted: 28/01/2019; Published: 30/01/2019
Abstract
Angiomyxoma of vulva are bizarre perineal lesions of skin and mucosal membranes with subcutaneous involvement. These are rare, slow growing benign lesions of mesenchymal origin, affecting women of reproductive age and are associated with high risk of local recurrence. Although angiomyxoma have a tendency of recurrence after excision, but they tend to grow slowly with a low tendency to metastasize [1-4].
Case Report
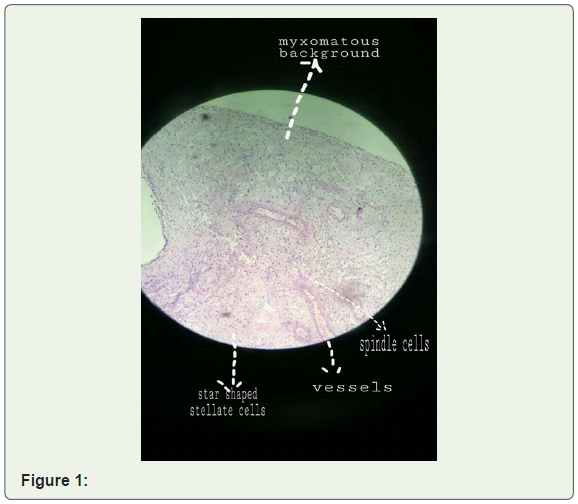
A 40 year old female P2L2 presented with complaint of dyspareunia since past 6 months. On clinical examination, locally multiple small mucosal polyps of approximately 1-1.5 cm were noted all around introitus on skin and on mucosal surface at 5,7,12 o clock position with surrounding peeling and superficial ulceration of the skin. Cervix and vagina were unremarkable on per speculum examination. She underwent complete excision of polyps from all sites. Base of polyps was vascular. Histopathology revealed angiomyxoma of vulva with stripped squamous epithelium with vascularized myxoid stroma, stellate cells, secondary inflammation and variable sized vessels; few multinucleated stromal cells are seen with reactive changes as seen in accompanied picture (Figure 1).
Discussion
In general, angiomyxoma are classified either as superficial (also known as cutaneous myxoma) or aggressive angiomyxoma. Macroscopically, aggressive angiomyxoma is a soft, well defined, sometimes polypoid mass, ranging in size from few centimeters to 20 cm or even more. The main feature is a shiny, homogenous, gelatinous appearance on gross sections. Microscopically, the tumor is composed of widely scattered spindled to stellate shaped cells with ill defined cytoplasm and small round to oval hyperchromatic nuclei with small centrally located nucleoli, embedded in a myxoid stroma. The latter is rich in collagen and often contains hemorrhagic foci. A defining special feature is presence of variably sized vessels that range from small thin walled capillaries to large vessels with secondary changes including perivascular hyalinization and medial hypertrophy. Superficial angiomyxoma may occur in setting of carney complex-an autosomal dominant genetic disorder. This lesion is observed predominantly in middle age adults. Clinically, most lesions appear as slowly growing polypoid cutaneous lesions and easily confused with a cyst, skin tag or neurofibroma. Aggressive angiomyxoma, although slow growing, behave aggressively by infiltrating the paravaginal and perirectal tissues and with very high rate of local recurrences. So differential diagnosis of aggressive angiomyxoma include angiofibroblastoma, myxoid neuro fibroma, myxoid liposarcoma, myxoid fibrosarcoma [3].
The main theory of angiomyxoma pathogenesis is that a primitive multipotent perivascular mesenchymal cell of lower female genital tract that has the capability of differentiating by various ways gives rise to the lesion. Some molecular studies have linked a consistent clonal aberration of chromosome 12, in the region 12q13-15, associated with rearrangement of the high mobility group protein isoform I-C [5].
However, there are no clearly established risk factors for vulvar superficial angiomyxoma and cause of tumor formation is also unknown. Tumor appears as well defined polyp and is not aggressive. If tumor is small no significant signs/symptoms or complications are noted. However, in some cases, it may present as pelvic pain and discomfort, urination difficulties and pain during sexual intercourse [2,5]. There are no geographical, racial or ethnic preferences for superficial angiomyxoma. It generally presents in slightly middle age females of 30-40 years. Tumor may be positive for ER and/or PR responding to hormonal therapy thus the cause may be linked to an abnormal hormonal influence.
Recurrences cannot be predicted from size or cellular activity of tumor. Recurrences have been reported from months to several years after excision.
Various methods have been used to treat recurrences. Hormonal treatments with tamoxifen, raloxifene or GnRH analogues have been used. Tumor resection with angiographic embolization may also be helpful to shrink tumor [2,3,6].
Radiation therapy and chemotherapy are considered less suitable options due to low mitotic activity of tumor.
Although recurrences are known to happen late but complications like emotional stress and concern, cosmetic concern, post surgical infection at wound site in repeated resections do occur, making counseling for long term follow up necessary.
References
- Bai HM, Yang JX, Huang HF, Cao DY, Chen J, et al. (2013) Individualized managing strategies of aggressive angiomyxoma of female genital tract and pelvis. Eur J Surg Oncol 39: 1101-1108.
- Chen H, Zhao H, Xie Y, Jin M (2017) Clinicopathological features and differential diagnosis of aggressive angiomyxoma of the female pelvis: 5 case reports and literature review. Medicine (Baltimore) 96: e6820.
- Orfanelli T, Kim CS, Vitez SF, Van Gurp J, Misra NA (2016) Case report of aggressive angiomyxomia in pregnancy: do hormones play a role? Case Rep Obstet Gynecol 2016: 6810368.
- Sato K, Ohira M, Shimizu S, Kuroda S, Ide K, et al. (2017) Aggressive angiomyxomia of the liver: a case report and literature review. Surg. Case Rep 3: 92.
- Sutton BJ, Laudadio J (2012) Aggressive angiomyxoma. Arch Pathol Lab Med 136: 217-221.
- Palomba S, Oppedisano R, Annunziata G, Zullo F, Amorosi A (2011) Leuprolide acetate depot plus high- dose raloxifene hydrochloride before and after surgery for recurrent vaginal aggressive angiomyxoma: a case report. Gynecol Oncol 123: 172-173.