HPV Inflammation Mediates IL-6 throughSTAT3 Signaling Pathway in Different Grades of Cervical Cancer
Dayalu Naik SL1-3, Vadlapudi Kumar2, Rama Joshi4 and Alok C Bharti1
1Division of Immunology, Institute of Cytology and Preventive Oncology, Noida, India
2Department of Biochemistry, Kuvempu University-P.G. Centre (Davangere University) Shivagangothri, Davangere-577002, Karnataka, India
3Deportment of Phytochemistry Regional Medical Research Center (ICMR), Neharu Nagar, Belagavi, Karnataka-590010
4Deportment of Gynae-Oncologist, Fortis Memorial Research Institute, Gurgaon, 122002
Corresponding author: Dayalu Naik SL, Division of Immunology, Institute of Cytology and Preventive Oncology,Noida, India; Deportment of Phytochemistry Regional Medical Research Center (ICMR), Neharu Nagar, Belagavi, Karnataka-590010.
Citation: Dayalu Naik SL, Kumar V, Joshi R, Bharti AC. HPV Inflammation Mediate IL-6 through STAT3 Signaling Pathway in Different Grades of Cervical Cancer. J Cancer Res Molecul Med. 2016;3(1): 103.
Copyright © 2016 Dayalu Naik SL, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Cancer Research and Molecular Medicine | Volume: 3, Issue: 1
Submission: Submission: 28/07/2016; Accepted: 22/08/2016; Published: 27/08/2016
Abstract
Over the past decade, high-risk of Human papilloma virus (HPV) impair of immune function, Interlukine-6 (IL-6) is proinflammatory cytokines promotes the growth cervical cancer through Signal transducer and activator of transcription 3 (STAT3) dependent mechanisms. Current study was designed the circulating cytokine level, Tissue biopsy mRNA gene expression by RT-PCR of IL-6, similarly the expression of STAT3 and pSTAT3 from 100 patients of pre cancer and cancer of the uterine cervix compare with 16 controls were studied. Whereas In the precancerous group have 54.4%, 43.9% 56.1% and 68.4%. In cervical cancer 79.1%, 72.1%, 72.1%, 27.9%and 83.7% the difference of two groups was significant correlation. It is interesting that the pattern of the investigated parameters indicates the difference in the pathological grade of precancerous and cervical cancer patients.
Introduction
Cervical is cancer, caused by human papilloma virus (HPV), is the fourth most important common cancer in worldwide. Nearly 5,2,762new cases of the uterine cervix are diagnosed, the mortality rate is 2,6,5672 per annum [1], Whereas in Indian scenario cervical cancer is the second most cancer in women at age 15-44 years, 1,22,844 new cases are registered per year and it has got the highest mortality rate 67,477 compared to in South Asia (ICO Information). HPV harbors in pre-malignancy of the uterine cervix [2], however, the molecular mechanism of cervical cancer is not clear. Several studies indicate that, qualitative as well as quantitative alterations in cytokines are the result impairments of immune function [3]. Soluble inflammatory mediator such as soluble interleukin-6 (IL-6), is a multifunctional cytokine plays an important role in a wide range of biological activities in different types of cells including tumor cells. Mediated by the IL-6 receptor-system IL-6/IL-6R/gp130 complex triggers Janus- Activated Kinase (JAK)/STAT [4]. Therefore increasing expression of IL-6/STAT signaling pathway associated with cancer progression. Abundant evidence demonstrated that, deregulated overexpression were associated cancer progression [5,6]. Elevated levels of IL-6 were seen in multiple epithelial tumor, on the other hand simultaneously increases the STAT family, which is also produced by a variety of cell types including tumor cells, and elevated levels have been reported in patients with several kinds of malignant disease such ascolorectal carcinoma [7], prostate cancer [8], breast cancer [9], liver cancer [10],pancreatic cancer, etc [11]. Based on these evidences, in the present study we measured in a cross-sectional design, cervical mRNA expression of IL-6 cytokine involved in STAT3 and pSTAT3 signaling pathway in a stage-specific manner of HPV induced cervical cancer samples.
Materials and Methods
Clinical specimen collection
This prospective randomized study was performed in cancer centers of Dharmshila Hospital, New Delhi between 2007-2012 with enrolment of patients until December 2011. All patients gave their written informed consent before enrolment. Abnormal colposcopy regions comprising white focal lesions characterized by an atypical transformation zone were selected for the punch-tissue 5mm biopsies, were collected immediately into cold 1x phosphate buffer saline (PBS). The tissues were divided into three portions, one portion was fixed in formalin for histologic analysis, the other was snapfrozen in liquid nitrogen and stored at -70 °C for RNA extraction for the analysis of cytokines expression and the other for the presence of HPV DNA analysis. Simultaneously 5ml heparinized blood was taken from the same patient, immediately plasma was separated and stored at -20 °C until further analysis.
PCR Analysis for HPV typing
High molecular weight genomic DNA was isolated from all tissue biopsies by phenol-chloroform extraction procedure [12]. The PCR for detection of DNA of HPV types 16 and 18 were carried outusing type-specific primers. All tissue biopsies were tested for HPV type using a pair of consensus primers (Table 1) designed for the sequences located within the conserved L1 ORF of HPV genome. PCR was performed in a 25 μl reaction mix containing 100 ng DNA, PCR buffer with magnesium chloride at final concentration 1.5 mM, 125 μM of each dNTPs, 5 pmol of each oligonucleotide primer and 0.5U Taq DNA polymerase were used. The temperature profile used for amplification constituted an initial denaturation 95 °C for 5 min followed by 35 cycles with denaturation at 95 °C for 30 sec, annealing at 55 °C for 30 sec and extension at 72 °C for 1min which was extended for 4 min in the final cycle. Amplification of β-globin gene which served as the internal control was carried out along with HPV.
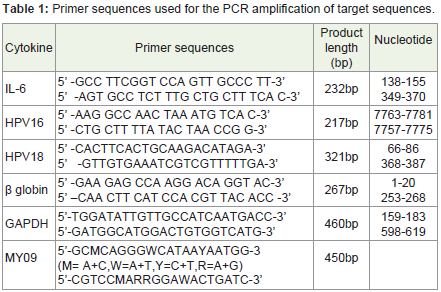
Table 1: Primer sequences used for the PCR amplification of target sequences.
Cytokine (IL-6) Quantification by ELISA
Blood samples were collected from cases and controls before initiation of any systemic treatment including radiotheapy. Serum samples were collected from 43 patients with cervical carcinoma, 57 patients with the least risky type cervical intraepithelial neoplasia, (also known as mild cervical dysplasia(clasification) (CIN I), moderate dysplasia (CIN II) and severe dysplasia (CIN III) ) and 16 from healthy control, the quantitation of cytokine IL-6 levels were estimated by enzymatic method, were measured at 450-570 nm by standard coupled enzymatic procedure, in duplicate according to the manufacturer’s instruction (Biolegend San Diego USA and e-bioscience San Diego USA) by using Gene-5 ELISA reader.
Quantitative PCR (RT-PCR) analysis
RNA isolation: Nucleic acids, DNA, and RNA were isolated from pre-cancer, cancerous and control tissues using phenol-chloroform isolation method and TRI reagent (Sigma-Aldrich, USA). RNA purity was checked by UV-spectrophotometry at 260 nm, Integrity was confirmed by visualization of 28S and 18S bands on 1% agarose gel and stored immediately at -70 °C until test was carried out.
Real time RT-PCR
Expression of IL-6 mRNA, was analyzed by RT-PCR amplification, cDNA was synthesized from 0.1-5 μg of total RNA using 10 ng/μl random hexamers, 0.4U/μl ribonuclease inhibitor, 1mM of each dNTPs and 2.5U/μl of Moloney murine leukemia virus reverse transcriptase (all reagents are from Fermentas, Thermo Scientific, USA). IL-6 RT-PCR amplification was performed by adding 2μl of cDNA sample to a final volume of reaction mixture, 25μl containing 10x PCR buffer 5 mM each dNTPs, MgCl2 (25 mM) Taq DNA polymerase (2.0U/ml) and 2nM of each primers in each PCR reaction cycle. Negative control, contain no cDNA samples in the reaction mixture. Amplification cycles performed in Eppendorf PCRthermal cycler, initially denatured at 94 °C for 4 min, annealed at 55 °C for 30 sec followed by extension at 72 °C for 30 sec, repeated upto 35 cycles. 10-15 μl of amplified product was run on 2% agarose gel. The primers used for IL-6, MY09, HPV16, 18, GAPDH and β-actin (Table 1) were purchased from Sigma-Aldrich, USA. All primers were checked against the available Genbank Database accessions to ensure the no cross reactivity with other human sequences.
Immunohistochemistry
Respective tissue blocks were cut into 3 to 4 μm thick sections, de-paraffinized with xylene and then rehydrate into distilled water through the gradient alcohol. Antigen retrieval was carried out by autoclaving slides into sodium citrate (pH 6.0) for 25 min, then tissue sections were incubated in freshly prepared solution of methanol and 3% hydrogen peroxide to block endogenous peroxidase activity, followed by incubation in normal mouse serum to block non-specific binding. Tissue sections were incubated with 1:100 dilution of primary monoclonal antibody against STAT3 and pSTAT3 oncoprotein (Santa Cruz Biotechnology). The sections were incubated with primary antibody in a humid chamber at room temperature for 60 min, the slides were washed three times in phosphate buffered solution and further incubated with a biotinylated secondary antibody for 30 min at room temperature, antigen antibody complex were detected by substrate 3 3’ diaminobenzidine hydrochloride (Sigma Aldrich) (0.1%) in a freshly prepared solution of PBS with (0.05% hydrogen peroxide). The slides were counterstained with hematoxylin and then examined by light microscopy using 40X.
Statistical Analysis
The data analysis were performed using SPSS software 14.0 for windows (SPSS INC, Chicago, IL). The analysis of variance (ANOVA) was applied for comparisons between mean age of cancer pre-cancer and normal. Chi square and Fisher Exact test was employed to see the association among different histopathological grades of tissue biopsies. Spearman’s correlation was carried out to look into the relationship between molecular markers. p<0.05 was considered as statistically significant.
Results
The present study was designed to permit viral load high risk HPV16 and 18 types most frequently found in different grades of cervical intraepithelial neoplasia (CIN I to CIN III) and cervical tumors (Ca Cx). The mean age ± SD of pre-cancer, cancer and controls were 45.22±9.73, 55.88±9.72 and 40.88±11.03 years respectively. The differences in the mean age amongst the groups were found to be statistically significant (P<0.001). Type specific detection of HPV DNA analysed according to histology diagnoses and results are tabulated (Table 2). DNA sample was isolated from 116 samples. The data (Table 3) shows the frequencies of HPV 16 DNA increased along with degree of epthelial lision in different grads of pre-cancer were 06 out of 14 CINI, 12 out of 18CINII, 19 out of 25 CINIII and 37 out of 43 in CaCx lesion and control 16. the most prevalancetype observed in CIN and SCC groups. 42.9%, 66.7%, 66.7%, and 86.0%, (P<0.001), followed by HPV18 0%, 0%, 24% and 25.6% (P=0.007) were found respectivly. Forther statistically copairsum with pre-cancer with caner HPV16 64.9% and 86.0% ware P=0.017 similarly HPV18 10.5% and 25.6% ware P=0.047.
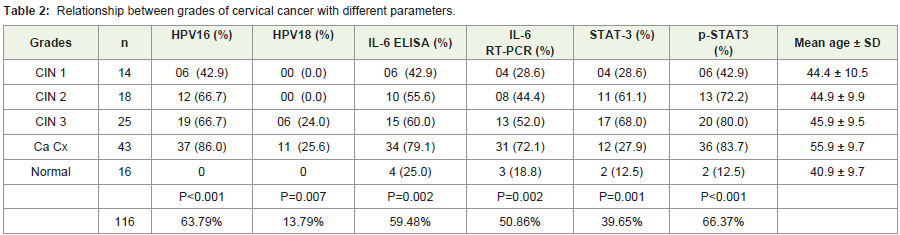
Table 2: Relationship between grades of cervical cancer with different parameters.

Table 3: Relationship between the pre-cancer and cancer in different parameters.
Forther of this study revealed that, concentration of increasedcirculating levels of IL-6 in pre-cancer and cancer cases, 42.9%, 55.6%,60.0% and 79.1% ware P=0.002 but when we analyze between the pre-cancer and cancer 54.4% and 79.1% respectively ware P=0.010. Results of the study are depicted as the mean standard deviation, range of values of serum IL-6 levels for different grades (Figure 1).It was observed that, mean IL-6 levels of pre-cancer (0.233 ± 0.28 pg/ml), cancer (0.380 ± 0.367 pg/ml) and control (0.034 ± 0.020 pg/ml) subjects were found to be higher as compared to patients with carcinoma of cervix subjects (P=0.002). Similar trend was noticed with mean difference between pre-cancer (mean 0.22 ± 0.28), cancer (mean 0.41 ± 0.36) and control (mean 0.034 ± 0.0207). These differences in the levels of IL-6 were found to be statistically significant (P<0.002), a value 0.07 pg/ml was considered as positive. Results of IL-6 mRNA expression measured in samples collected from the base line visits of 116 women, by quantitative RT-PCR suggest that, as compared to pre-cancer, cancer and controls there is a significance relation among different grades of cancer, 28.6%, 44.4%, 52.0%, 72.1% and control 18.8% (P=0.002), when compared to pre-cancer and cancer 43.9% and 72.1% respectively (P=0.005) (Figure 2). Among the patients with squamous cell carcinoma, 27 patient had well differentiated tumor, 9 had moderately differentiated and the rest of 7 cases belonged to poorly differentiated squamous cell carcinoma.
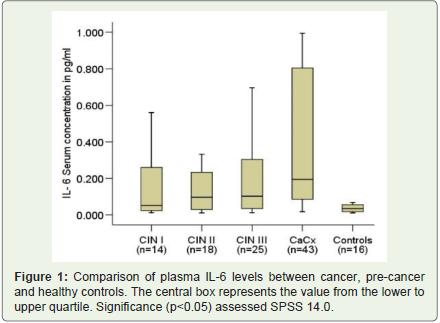
Figure 1: Comparison of plasma IL-6 levels between cancer, pre-cancer and healthy controls. The central box represents the value from the lower to upper quartile. Significance (p<0.05) assessed SPSS 14.0.
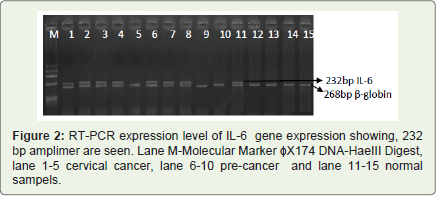
Figure 2: RT-PCR expression level of IL-6 gene expression showing, 232 bp amplimer are seen. Lane M-Molecular Marker ɸX174 DNA-HaeIII Digest, lane 1-5 cervical cancer, lane 6-10 pre-cancer and lane 11-15 normal sampels.
In addition to these, the levels of IL-6 were compared and confirmed in activating STAT3 and p-STAT3 signaling pathway. Results of the investigations (Figure 3) suggest that, a significantrelation exists between expression of STAT3 and pSTAT3 in precancerand cancer. For STAT3 28.6%, 61.1%, 68.0%, 27.9% and control 12.5% (P=0.001), similarly for pSTAT3 42.9%, 72.2%, 80.0%, 83.7% and control 12.5% respectively (P<0.001). But when compared to pre-cancer in cancer STAT3 is 56.1% and 27.9% (P=0.005), whereas pSTAT3 is 68.4% and 83.7% were P<0.080 respectively. For STAT3 CIN 1 staining confined to the lower one third (Figure 3D), CIN 2 staining confined to the lower 2/3 of the epithelium, (Figure 3D),and SCC staining of malignant cells as compared to control (Figure 3E). STAT3 immuno-staining shows intense cytoplasmic staining that clearly highlights the lesion cells, but no nuclear positivity. Whereas P-STAT3 shows strong nuclear and cytoplasmic expression as compare to pre-cancer stage. In control sample neither STAT3 nor pSTAT3 was present in mature superficial squamous epithelial cells (Figure 3Eand Figure 3J). Further, a significant intra-relationship was found between the expression of STAT3 and pSTAT3 in cervical cancer.
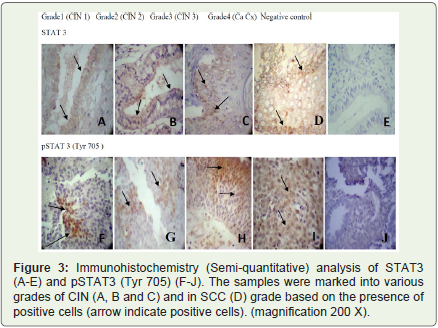
Figure 3: Immunohistochemistry (Semi-quantitative) analysis of STAT3 (A-E) and pSTAT3 (Tyr 705) (F-J). The samples were marked into various grades of CIN (A, B and C) and in SCC (D) grade based on the presence of positive cells (arrow indicate positive cells). (magnification 200 X).
We analyzed pair-wise comparison between pre-cancer versus cancermean P<0.01, pre-cancer versus control P<0.01 and cancer versus control P<0.001. Overall scenario was observed to be statistically significant. In the present study, it has been observed that, invasive carcinoma of the uterine cervix was increased in all the patients as compared to age matched control group.
Discussion
IL-6 acts as both pro-inflammatory and anti-inflammatory cytokine, primarily produced at sites of acute and chronic inflammation,where it is secreted into the serum and induces a transcriptionalinflammatory response through interleukin-6 receptor. Based on these facts, in the present study, we further investigated molecular mechanism by IL-6 in epithelial and sub-epithelial tissues in plasma, and mRNA levels by combined quantitative RT-PCR in relation to cervical cancer and pre-cancer associated with HPV16/18 in different stages (grades) of cervical cancer. The results of the study revealed that, an increased circulating levels of IL-6 were seen in cancer and pre-cancer stage as compared to controls. Contrary to the opinion that, higher levels of serum IL-6 is related to stress associated with ovarian cancer [13], but in the present study, it was observed that,any such effect of stress as evident by significantly higher levels of IL-6 in cervical cancer patients. In the present study results have shownthat, an increasing in the levels of serum IL-6 observed, followed by increase in the epithelial and sub-epithelial mRNA expression as confirmed by quantitative RT-PCR. Further results of the IHC for STAT3 and pSTAT3 expression in different grades of cervical cancer patients confirms that, there was increase in pSTAT3 levels, with increasing STAT3 levels. Findings of the previous studies as reported that, STAT3 signaling pathway is the most important in carcinoma of cervix. However the activation of STAT3 is poor prognosis of various cancers [14]. Some studies demonstrated that, STAT3 activation iscorrelated with improved overall survival [15]. But the findings of present study suggest that, activation of STAT3 lead to increased expression of pSTAT3 in cancer and pre-cancer as compared tocontrols.
The complex formation of IL-6-JAK-STAT3 signaling pathway plays an important role in transformation of non-differentiated cancer cells to cancer cells [16]. Therefore, several analysis suggest that, increased IL-6 levels play an important role in formationof cancer cells. It has been confirmed by some studies that, risk ofcervical cancer was positively and significantly associated with HPVinflammation, that leads to elevated levels of IL-6 [17]. In the present study it has been noticed that, increased serum IL-6 levels showed a bimodal distribution that may reflect in some patients that other concomitant conditions, particularly with HPV inflammation. In similar way the cohort study was established that, cervical cancer with HPV infection is significantly associated with the elevated levels of cytokine production [18]. In agreement with these findings, our results also confirm that, serum IL-6 levels in cervical cancer patients are 25-fold higher than healthy controls.
Further, we investigated immunohistochemistry analysis (IHC) of STAT3 and pSTAT3 expression that helps for the better understanding the progression of endometrial cancer and cervical cancer that involve the activation of multiple oncogenic pathway including the constitutive STAT3 pathway. Interestingly, in the present study, a significant relation was observed between over-expression of STAT3 in cervical cancer grading. Further, a significant relationship was found between the expression of STAT3 and pSTAT3 in cervical cancer. Recent studies suggest that, HPVinflammation in early stage protein IL-6 would activate the IL-6/STAT3 signaling pathway [19]. A highly significant correlation has been observed between the expression of the two proteins and the histological grade of the lesions. Even though activation of STAT3 in cervical cancer is still not clear, on the other hand a wide variation has been observed in the rate of immunopositivity of STAT3 which is activated by phosphorylation at Tyr 705 and Ser 727 [20], intracellular staining intensity of pSTAT3 was strong in 69.0% in cervical cancer [21]. Results of the present study also showed that, overall pSTAT3 positivity is 75% in pre-cancer and cancer (Figure 3). Therefore theconstitutive activation of STAT3 at Tyr705 residue may be involved in progression of the pre-malignant lesion and possibly early stage of pathogenesis of cervical cancer. pSTAT3 expression in cancer and pre-cancer lesions were significantly associated with histological grade. From the results of the study, it could be concluded that, increased expression of IL-6 activates STAT3 signaling pathway, serves as a principle mediator of the crosstalk between the tumor cells and the cells that constitute the tumor microenvironment, may be promoting an immunosuppressive microenvironment with tumorenhancing properties in cervical cancer.
References
- Globocan (2012) Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012. International Agency for Research on Cancer.
- Baldez da Silva MF, Guimaraes V, Silva MA, Medeiros do Amaral CM, Becak W, et al. (2012) HPV31 and HPV33 incidence in cervical samples from women in Recife, Brazil. Genet Mol Res 11: 462-466.
- Waldner MJ, Foersch S, Neurath MF (2012) Interleukin-6 - A Key Regulator of Colorectal Cancer Development. Int. J Bio Sci 8: 1248-1253.
- Kemp TJ, Hildesheim A, Garcia-Pineres A, Williams MC, Shearer GM, et al. (2010) Elevated systemic levels of inflammatory cytokines in older women with persistent cervical human papillomavirus infection. Cancer Epidemiol Biomarkers Prev 19: 1954-1959.
- Nagasaki T, Hara M, Nakanishi H, Takahashi H, Sato M, et al. (2014) Interleukin-6 released by colon cancer-associated fibroblasts is critical for tumour angiogenesis: anti-interleukin-6 receptor antibody suppressed angiogenesis and inhibited tumour–stroma interaction. Br J Cancer 110: 469-478.
- Rojas A, Liu G, Coleman I, Nelson PS, Zhang M, et al. (2011) IL-6 promotes prostate tumorigenesis and progression through autocrine cross-activation of IGF-IR. Oncogene 30: 2345-2355.
- Dethlefsen C, Hojfeldt G, Hojman P (2013) The role of intratumoral and systemic IL-6 in breast cancer. Breast Cancer Res Treat 138: 657-664.
- Ohishi W, Cologne JB, Fujiwara S, Suzuki G, Hayashi T, et al. (2014) Serum interleukin-6 associated with hepatocellular carcinoma risk: a nested case-control study. Int J Cancer 134: 154-163.
- Coward J, Kulbe H, Chakravarty P, Leader D, Vassileva V, et al. (2011) Interleukin-6 as a therapeutic target in human ovarian cancer. Clin Cancer Res 17: 6083-6096.
- Sansone P, Bromberg J (2012) Targeting the Interleukin-6/Jak/Stat Pathway in Human Malignancies. J Clin Oncol 30: 1005-1014.
- Chang Q, Bournazou E, Sansone P, Berishaj M, Gao SP, et al. (2013) The IL-6/JAK/Stat3 feed-forward loop drives tumorigenesis and metastasis. Neoplasia 15: 848-862.
- Guo Y, Xu F, Lu T, Duan Z, Zhang Z (2012) Interleukin-6 signaling pathway in targeted therapy for cancer. Cancer Treat Rev 38: 904-910.
- Liu W, Xie S, Chen X, Rao X, Ren H, et al. (2014) Activation of the IL-6/JAK/STAT3 signaling pathway in human middle ear cholesteatoma epithelium. Int J Clin Exp Pathol 7: 709-715.
- Shukla S, Shishodia G, Mahata S, Hedau S, Pandey A, et al. (2010) Aberrant expression and constitutive activation of STAT3 in cervical carcinogenesis: implications in high-risk human papillomavirus infection. Mol Cancer 9: 282.
- Choi CH, Song SY, Kang H, Lee YY, Kim CJ, et al. (2010) Prognostic significance of p-STAT3 in patients with bulky cervical carcinoma undergoing neoadjuvant chemotherapy. J Obstetrics Gyn Res 36: 304-310.
- Nilsson MB, Armaiz-Pena G, Takahashi R, Lin YG, Trevino J, et al. (2007) Stress hormones regulate interleukin-6 expression by human ovarian carcinoma cells through a Src-dependent mechanism. J Biol Chem 282: 29919-29926.
- Huang X, Meng B, Iqbal J, Ding BB, Perry AM, et al. (2013) Activation of the STAT3 signaling pathway is associated with poor survival in diffuse large B-cell lymphoma treated with R-CHOP. J Clin Oncol 31: 4520-4528.
- Xiong H, Du W, Wang JL, Wang YC, Tang JT, et al. (2012) Constitutive activation of STAT3 is predictive of poor prognosis in human gastric cancer. J Mol Med (Berl). 90: 1037-1046.
- Arany I, Megyesi JK, Nelkin BD, Safirstein RL (2006) STAT3 attenuates EGFR-mediated ERK activation and cell survival during oxidant stress in mouse proximal tubular cells. Kidney Int 70: 669-674.
- Kim SY, Kang JW, Song X, Kim BK, Yoo YD, et al. (2013) Role of the IL-6-JAK1-STAT3-Oct-4 pathway in the conversion of non-stem cancer cells into cancer stem-like cells. Cell Signal 25: 961-969.
- Cheng YW, Lee H, Shiau MY, Wu TC, Huang TT, et al. (2008) Human papillomavirus type 16/18 up-regulates the expression of interleukin-6 and antiapoptotic Mcl-1 in non-small cell lung cancer. Clin Cancer Res 14: 4705-4712.
- Scott ME, Shvetsov YB, Thompson PJ, Hernandez BY, Zhu X, et al. (2013) Cervical cytokines and clearance of incident human papillomavirus infection: Hawaii HPV cohort study. Int J Cancer 133: 1187-1196.
- Shi TY, Zhu ML, He J, Wang MY, Li QX, et al. (2013) Polymorphisms of the Interleukin 6 gene contribute to cervical cancer susceptibility in Eastern Chinese women. Hum Genet 132: 301-312.
- Ren C, Cheng X, Lu B, Yang G (2013) Activation of interleukin-6/signal transducer and activator of transcription 3 by human papillomavirus early proteins 6 induces fibroblast senescence to promote cervical tumourigenesis through autocrine and paracrine pathways in tumour microenvironment. Eur J Cancer 49: 3889-3899.
- Schuringa JJ, Wierenga AT, Kruijer W, Vellenga E (2000) Constitutive Stat3, Tyr705, and Ser727 phosphorylation in acute myeloid leukemia cells caused by the autocrine secretion of interleukin-6. Blood 95: 3765-3770.