Research Article
IGF2 ApaI 'G' Allele, a Significant Risk Factor for Uterine Fibroids with Putative Association with High BMI
Sireesha Vaidya1, Noor Ahmad Shaik2, Srinivas Chava3, K. Prabhakar Rao1, Vijayalaxmi Kodati4, Y.R.Ahuja4 and Q.Hasan5*
Corresponding author: Q. Hasan, Department Of Genetics and Molecular Medicine, Kamineni Hospitals, L.B.Nagar,Telangana, 500 074, Hyderabad, India
Citation: Citation: Vaidya S, Shaik NA, Chava S, Rao KP, Vijayalaxmi K, et al. IGF2 ApaI 'G' Allele, a Significant Risk Factor for Uterine Fibroids with Putative Association with 02 High BMI. J Cell Sci Molecul Biol. 2017;3(1): 116.
Copyright © 2015 Sujay Ghosh et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Submission: 05/12/2016; Accepted: 02/01/2017; Published: 27/01/2017
Abstract
Uterine Leiomyomas (UL's) or fibroids are the most common pelvic tumor in women and the estimated incidence is 20%-40% during their reproductive years. The gene expression profile of UL has been examined, particularly in comparison to adjacent myometrium and several differentially regulated genes were identified, this includes Insulin-like Growth Factor-2 (IGF2), which was found to be upregulatedsignificantly. IGF2 is a well-established cell proliferation factor and a recent study described it as a fibroid specific marker. The IGF2 ApaI polymorphism in the gene was evaluated in the present study. The 'G' allele was found to be significantly associated with uterine leiomyomas (OR = 3.56; 95% CI (2.454 - 0 5.172), p < 0.0001). The risk ratio for developing uterine fibroid for individuals with GG genotype was found to be almost four fold when compared to AA or AG genotype in the evaluated population group. Furthermore, 13% (3/23) of obese individuals i.e patients with BMI > 30 kg/m2 as per WHO criteria were either homozygous or heterozygous for IGF2 'G' allele indicating its possible association with high BMI in UL cases.
Introduction
Uterine leiomyomata (UL), are the most common benign pelvic gynecological tumors. The estimated lifetime risk of uterine fibroids in a woman by the age of 45 years is more than 60% [1]. Based on the fact that 20-30% women in reproductive age group have symptomatic fibroid uterus [2], it is estimated that at least 15-25 million women will be suffering from a fibroid uterus at given time (Ministry of Health and Family Welfare, Govt. of India). Women present with prolonged or heavy menstrual bleeding, pelvic pressure or pain and in rare cases, reproductive dysfunction which requires medical attention [3]. Known risk factors for development of uterine fibroids include nulliparity, early menarche and increased frequency of menses, history of dysmenorrhea, family history of uterine fibroids, ethnicity, obesity and age. To date, the pathogenesis of UL is not well understood because of the disease heterogeneity and multifactorial involvement [4,5]. Earlier work from various groups including ours supports the concept that ovarian sex steroid hormones, growth factors, apoptosis-related and mitochondrial factors may play critical roles in the regulation of leiomyoma growth [6-10].
Insulin-like Growth Factor 2 (IGF 2), a circulating peptidehormone with high degree of amino acid sequence homology to insulin is well known for its contribution in mammalian cell growth due to its regulatory influence on cell division, differentiation and metabolism [11]. IGF2 may also play a role in intrauterine programming predisposing to different disease in postnatal life[12,13]. IGF2 has been identified as a fibroid-specific marker and its expression levels were found to be increased in leiomyomas when compared to adjacent myometrium [14,15]. According to GWASstudies this region was found to be associated with UL in Asian population [5].
Several reports have shown that specific polymorphisms of IGF2are associated with weight and obese phenotype [16-20] and are also related to cardiovascular risk factors such as fat mass distribution [21] and hypertension [22,23]. IGF-2 ApaI (rs680) polymorphism located in 3' UTR region was demonstrated as a risk factor for renal complications in Diabetes Mellitus cases. Moreover, increased IGF2 expression in association with this polymorphism in obesity and PCOS cases was noted earlier [16,24]. However, its association with risk of uterine leiomyomata remains speculative with contradictory reports[25,26]. Therefore, in the present study, we sought to determine the association of IGF2 ApaI to the risk of UL among patients of South Indian population.
Methodology
Subjects and sampling
The present study was carried out on 150 patients (21 to 64years) diagnosed to have Uterine Leiomyomas (UL's) by clinical andultrasound examinations and one hundred and fifty age-matched healthy control women (without any evidences of gynecological problems and normal ultrasound). They were enrolled from different hospitals of Hyderabad and Secunderabad cities of South India. The study was approved by the institutional ethical committee prior to its commencement. The patient's clinical and demographic history including age, age at menarche, body weight, height, dietary habits, menstrual history, obstetric history and family history were documented in a specially designed clinical case sheet at the time of sampling. After obtaining informed consent, 2ml of Na-EDTA blood and leiomyoma and matched myometrium tissue biopsies (0.5-1cm thickness tissue) in normal saline from hysterectomised uteruses was collected from the study participants to carry out genetic analysis.
Nucleic acid isolation
The DNA isolation from blood and tissue specimens was donefollowing the routine salting-out method described earlier [6].
IGF-2 ApaI genotyping
In the present study, 300 DNA samples were processed for IGF2ApaI polymorphism using specific primers, i.e., forward - 5’CTT GGA CTT TGA GTC AAA TTG G 3’; Reverse - 5’GGT CGT GCC AAT TAC ATT TCA. A three-step PCR of 25μl reaction volume was carried out using thermal cycler (UV Gene, UK). Briefly, the PCR conditions included an initial denaturation at 94°C for 5min, followed by 35 cycles of denaturation at 94°C for 30sec, annealing at 60°C for 30sec, and extension at 72°C for 45sec with a final extension at 72°C for 5min [27]. Amplified PCR products of 292 bp were run on a 2%agarose gel, and their band images were analyzed with UV I Tech geldocumentation system (Cambridge, UK). Restriction digestion with ApaI enzyme was carried out to determine A (not digested by ApaI) and G alleles (digested by ApaI) by specific banding pattern on the gel i.e., 292 bp and 229 bp, respectively.
Statistical analysis
Statistical analyses were performed with Graphpad quick calc,version 6.0 (GraphPad Software Inc, USA) online statistical software.For each SNP, allele and genotype frequencies were computed in controls. Statistically significant difference in allele and genotypes was determined using Pearson's standard Chi-square test, odds ratio (OR) and 95% confidence interval (CI). Hardy Weinberg equilibrium was tested on a contingency table of observed versus predicted genotype distributions using a chi-squared test with one degree of freedom. A p-value of 0.05 was considered statistically significant.
Multifactor Dimensionality Reduction (MDR) analysis
MDR software application aids to determine which polymorphisms and which environmental factors are associated with common, complex diseases such as Uterine fibroids. This algorithm enables determining and characterizing interactions among multiplefactors. In the present study, MDR was applied to demographic characteristics and gene polymorphisms [28].
Results
Clinical analysis
Women with UL were in the age range of 21-64 years and themean age at hysterectomy was 41.36 ± 7.32 years. For controls, age range was 23-54 years (39.32 ± 6.01 years). Approximately, 80% (120/150) of women diagnosed with UL reported symptoms such as polymenorrhagia, passing clots, pelvic pain and pressure. The average body weight in cases of UL ranged from 30-95kg with mean BMI of 25.10 ± 6.17. It was found that obese women according to WHO criteria were more in cases than controls showing the difference to be statistically significant (p = 0.0015). Age at menarche ranged from8-16 years in women with fibroids and early age at menarche i.e., ≤ 11years was found in higher number of women with UL when compared to control group whereas later age at menarche (> 14 years) was seen only in cases with none in control group. Thus, both early and late menarche were found to be associated with fibroids. Co-morbidities such as hypertension, Type 2 DM also showed association with UL which was statistically significant. Multiple fibroids occurred in 70.3% patients while 29.7% were solitary tumors and 24.27% of UL [Figure 1].
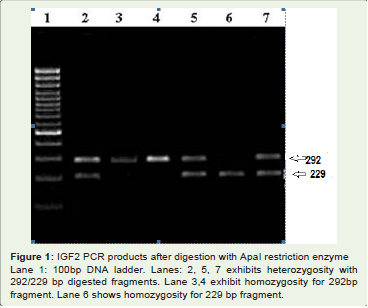
Figure 1: IGF2 PCR products after digestion with ApaI restriction enzyme Lane 1: 100bp DNA ladder. Lanes: 2, 5, 7 exhibits heterozygosity with 292/229 bp digested fragments. Lane 3,4 exhibit homozygosity for 292bp fragment. Lane 6 shows homozygosity for 229 bp fragment.
cases had large tumors with a size of > 72 mm. Fibroids are of five types based on their location of occurrence in uterus. The present data shows the occurrence of Intramural fibroids (IM) was more common(~ 61%) when compared to sub-serosal (SS), sub-mucosal (SM) orcervical fibroids.
IGF2 ApaI genotyping analysis
Of the 150 individuals with uterine fibroids genotyped in the present study 39.3% were A/A, 44% were A/G and 16.7% were G/G while in controls the genotypes were 64% A/A, 33.4% A/G and 2.7% G/G [Table 2]. There was an association of UL with 'G'allele (OR = 3.56; 95% CI (2.454 - 5.172) and G/G genotype (OR = 7.30; 95% CI (2.473 - 21.55) when compared to controls.
MDR analysis of IGF2 ApaI polymorphism with clinicalvariables
The IGF2 ApaI A>G polymorphism when evaluated with thedemographic and clinical factors like diet, nulliparity, hypertension,BMI, age at menarche, Diabetes Mellitus by MDR analysis has shownmore or less independent role of these genetic variants in disease[Figure 2].
mostly redundant interaction with clinical variables showing negativeinteraction. IGF2 was showing synergistic interaction in the order ofhypertension, BMI, Age at menarche followed by Diet and T2DM andnulliparity was showing the most redundant interaction. The presentdata corroborates with the finding of putative association of high BMIwith G allele of IGF2 ApaI polymorphism [16,29] [Figure 2] [Table 1].
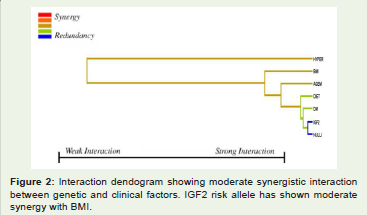
Figure 1: Interaction dendogram showing moderate synergistic interaction between genetic and clinical factors. IGF2 risk allele has shown moderate synergy with BMI.
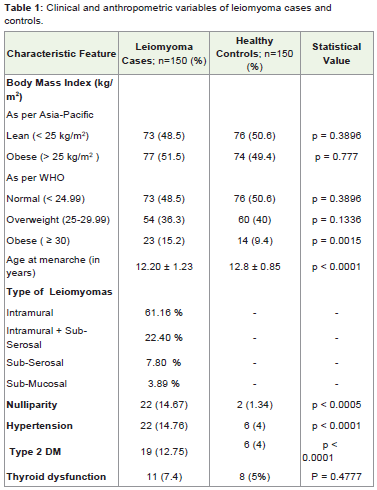
Table 1: Clinical and anthropometric variables of leiomyoma cases and controls.
Discussion
IGF2 is known to be involved in the pathogenesis of severalhuman tumors. It has proliferative activity in adult muscle, includingthose arising from smooth muscle [25]. The up-regulation of IGF2 was evident in leiomyomas compared to normal myometrium of uterus in several studies [14,15,28,30-35]. IGF2 shows growth stimulatory effect on Leiomyomas through mediation of ER-α and IGF-1R [36,37]. The 3’UTR region of IGF2 was associated with UL in a previous study [38].
IGF2 gene polymorphism was studied by Gloudemans et al. who were pioneers in this field and they showed differences between allelefrequencies in the ApaI polymorphism among Dutch patients with uterine leiomyomas and a matched unaffected control group [26].The IGF2 G allele was associated with increased IGF2 mRNA levels inleukocytes compared with the A alleles. It was hypothesized that thisfunctional polymorphism could result in increased IGF2 expression in liver Vafiadis et al. Vu et al. demonstrated a similar correlationin American women with uterine smooth muscle tumors. Based on these data, it was suggested that women homozygous for allele G are more prone to develop leiomyomas. In the present study, 'G' allele (presence of Apa I site) was found to be strongly associated with uterine leiomyomas showing Minor Allele Frequency G vs. A to be highly statistically significant (p < 0.0001). The risk ratio for developing uterine fibroids for GG genotyped individuals was found to be almost seven fold when compared to AA or AG individuals in the evaluated population group [Table 2].
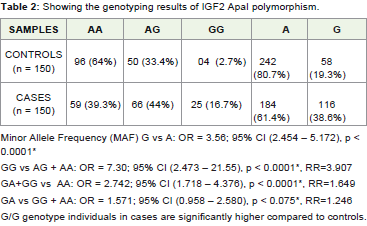
Table 2: Showing the genotyping results of IGF2 ApaI polymorphism.
The data from the previous study Rainho et al., suggested the putative association between IGF2 ApaI polymorphism and BMI in women with uterine leiomyomas [25]. However, lack of statistical significance provides no support for the hypothesis that obese patients who are carriers of 'G' allele constitute a group more prone to leiomyoma development. The present study MDR analysis showed moderate synergistic interaction of IGF2 ApaI with BMI and 13% (3/23) of individuals who were either homozygous or heterozygous for 'G' allele have a higher BMI (≥ 30kg/m2) when compared to AA individuals. The data from 150 patients indicate the possible association between 'G' allele and obesity as per WHO criteria however, more studies need to be carried out in a large sample size.
References
- Okolo S (2008) Incidence, aetiology and epidemiology of uterine fibroids. ,Best Pract Res Clin Obstet Gynaecol 22: 571-588.
- Khan AT, Shehmar M, Gupta JK (2014) Uterine fibroids: current perspectives. Int J Womens Health., 6: 95-114.
- Bulun SE (2013) Uterine fibroids. N Engl J Med 369: 1344-1355.
- Peddada SD, Laughlin SK, Miner K, Guyon JP, Haneke K, et al. (2008) Growth of uterine leiomyomata among premenopausal black and white women. Proc Natl Acad Sci USA 105: 19887-19892.
- Cha PC, Takahashi A, Hosono N, Low SK, Kamatani N et al. (2011) A genome-wide association study identifies three loci associated with susceptibility to uterine fibroids. Nature Genetics 43: 447-450.
- Vaidya S, Shaik NA, Latha M, Chava S, Mohiuddin K, et al. (2012) No evidence for the role of somatic mutations and promoter hypermethylation of FH gene in the tumorigenesis of nonsyndromic uterine leiomyomas. Tumour Biol 33: 1411-1418.
- Shaik NA, Lone WG, Khan IA, Vaidya S, Rao KP, et al. (2011) Detection of somatic mutations and germline polymorphisms in mitochondrial DNA of uterine fibroids patients. Genet Test Mol Biomarkers 15: 537-541.
- Maruo T, Ohara N, Wang J, Matsuo H (2004) Sex steroidal regulation of uterine leiomyoma growth and apoptosis. Hum Reprod Update, 10: 207-220.
- Doherty L, Mutlu L, Sinclair D, Taylor H (2014) Uterine fibroids: clinical manifestations and contemporary management. Reproductive Sciences 21: 1067-1092.
- Kim JJ, Sefton EC (2012) The role of progesterone signaling in the pathogenesis of uterine leiomyoma. Mol Cell Endocrinol 358: 223-231.
- Chegini N (2010) Proinflammatory and profibrotic mediators: principal effectors of leiomyoma development as a fibrotic disorder. Semin Reprod Med 28: 345-346.
- Painter RC, De Rooij SR, Bossuyt PM, Osmond C, Barker DJ, et al. (2006) A possible link between prenatal exposure to famine and breast cancer: a preliminary study. Am J Hum Biol 18: 853-856.
- Heijmans BT, Tobi EW, Stein AD, Putter H, Blauw GJ, et al. (2008) Persistent epigenetic differences associated with prenatal exposure to famine in humans. Proc Natl Acad Sci USA 105: 17046-17049.
- Arslan AA, Gold LI, Mittal K, Suen TC, Belitskaya LI, et al. (2005) Gene expression studies provide clues to the pathogenesis of uterine leiomyoma: new evidence and a systematic review. Hum Reprod 20: 852-886.
- Di Tommaso S, Massari S, Malvasi A, Bozzetti MP, Tinelli A (2013) Gene expression analysis reveals an angiogenic profile in uterine leiomyoma pseudocapsule. Molecular Human Reproduction, 19: 380-387.
- O'Dell SD, Miller GJ, Cooper JA, Hindmarsh PC, Pringle PJ, et al. (1997) Apal polymorphism in insulin-like growth factor II (IGF2) gene and weight in middle-aged males.Int J Obes Relat Meta Disord 21: 822-825.
- Gaunt TR, Cooper JA, Miller GJ, Day IN, O'Dell SD. (2001) Positive associations between single nucleotide polymorphisms in the IGF2 gene region and body mass index in adult males. Hum Mol Genet 14: 1491-501.
- Le Stunff C, Fallin D, Bougnères P (2001) Paternal transmission of the very common class I INS VNTR alleles predisposes to childhood obesity. Nat Genet 29: 96-99.
- Gu D, O'Dell SD, Chen XH, Miller GJ, Day IN (2002) Evidence of multiple causal sites affecting weight in the IGF2-INS-TH region of human chromosome 11. Hum Genet 110: 173-181.
- Zhang W, Maniatis N, Rodriguez S, Miller GJ, Day IN, et al. (2006) Refined association mapping for a quantitative trait: weight in the H19-IGF2-INS-TH region. Ann Hum Genet 70: 848-856.
- Rice T, Chagnon YC, Pérusse L, Borecki IB, Ukkola O, et al. (2002) A genomewide linkage scan for abdominal subcutaneous and visceral fat in black and white families: The HERITAGE Family Study. Diabetes 51: 848-855.
- RodrÃguez S, Gaunt TR, O'Dell SD, Chen XH, Gu D, et al. (2004) Haplotypic analyses of the IGF2-INS-TH gene cluster in relation to cardiovascular risk traits. Hum Mol Genet. 13: 715-725.
- Faienza MF, Santoro N, Lauciello R, Calabrò R, Giordani L, et al. (2010) IGF2 gene variants and risk of hypertension in obese children and adolescents. Pediatr Res 67: 340-344.
- San Millán JL, Cortón M, Villuendas G, Sancho J, Peral B, et al. (2004) Association of the polycystic ovary syndrome with genomic variants related to insulin resistance, type 2 diabetes mellitus, and obesity. J Clin Endocrinol Metab 89: 2640-2646.
- Gloudemans T, Pospiech I, Van der Ven LT, Lips CJ, Den Otter W, et al. (1993) An avaII restriction fragment length polymorphism in the insulin-like growth factor II gene and the occurrence of smooth muscle tumors. Cancer Res 53: 5754-5758.
- Shetty PJ, Movva S, Pasupuleti N, Vedicherlla B, Vattam KK, et al. (2011) Regulation of IGF2 transcript and protein expression by altered methylation in breast cancer. J Cancer Res Clin Oncol 137: 339-345.
- Ahn WS, Kim KW, Bae SM, Yoon JH, Lee JM, et al. (2003) Targeted cellular process profiling approach for uterine leiomyoma using cDNA microarray, proteomics and gene ontology analysis. Int J Exp Pathol 84: 267-279.
- Gaunt TR, Cooper JA, Miller GJ, Day IN, O'Dell SD. (2001) Positive associations between single nucleotide polymorphisms in the IGF2 gene region and body mass index in adult males. Hum Mol Genet 14: 1491-501.
- Tsibris JC, Segars J, Coppola D, Mane S, Wilbanks GD, et al. (2002). Insights from gene arrays on the development and growth regulation of uterine leiomyomata. Fertil Steril 78: 114-121.
- Wang H, Mahadevappa M, Yamamoto K, Wen Y, Chen B, et al. (2003) Distinctive proliferative phase differences in gene expression in human myometrium and leiomyomata. Fertil Steril 80: 266–276.
- Skubitz KM and Skubitz AP (2003) Differential gene expression in uterine leiomyoma. J Lab Clin Med 141: 297-308.
- Catherino W, Salama A, Potlog NC, Leppert P, Tsibris J (2004) Gene expression studies in leiomyomata: new directions for research. Semin Reprod Med 22: 83-90.
- Quade BJ, Wang TY, Sornberger K, Dal Cin P, Mutter GL, et al. (2004) Molecular pathogenesis of uterine smooth muscle tumors from transcriptional profiling. Genes Chromosomes Cancer 40: 97-108.
- Hoffman PJ, Milliken DB, Gregg LC, Davis RR, Gregg JP (2004) Molecular characterization of uterine fibroids and its implication for underlying mechanisms of pathogenesis. Fertil Steril 82: 639-649.
- Moore AB, Castro L, Yu L, Zheng X, Di X, et al. (2007) Stimulatory and inhibitory effects of genistein on human uterine leiomyoma cell proliferation are influenced by the concentration. Hum Reprod 22: 2623-2631.
- Di X, Yu L, Moore AB, Castro L, Zheng X, et al. (2008) A low concentration of genistein induces estrogen receptor-alpha and insulin-like growth factor-I receptorinteractions and proliferation in uterine leiomyoma cells. Hum Reprod 23: 1873-1883.
- Hsieh YY, Chang CC, Wang YK, Hsu KH, Chen CP, et al. (2010) Insulin-like growth factors II exon 9 and E-cadherin-Pml I but not myeloperoxidase promoter-463, urokinase-ApaL I nor xeroderma pigmentosum polymorphisms are associated with higher susceptibility to leiomyoma. Anticancer Res 30: 2203-2208.