Research Article
A Preliminary Study on NPHS2 Gene Polymorphism (R229Q) in Diabetic Nephropathy Patients from South India
Parveen Jahan*
Corresponding author: Parveen Jahan, Department of Genetics & Biotechnology, Osmania University, Hyderabad, AP, India,; E-mail: dr_parveenjahan@yahoo.co.in
Citation: Mahwish UN, Jaffer AT, Mughni Chisti GM, Siraj M, Raju SB, et al. A Preliminary Study on NPHS2 Gene Polymorphism (R229Q) in Diabetic Nephropathy Patients from South India. J Cell Sci Molecul Biol. 2014;1(2): 108.
Copyright © 2014 Parveen Jahan et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Cell Science & Molecular Biology | Volume: 1, Issue: 2
Submission: 27/06/2014; Accepted: 29/06/2014; Published: 31/07/2014
Abstract
Background: Diabetic nephropathy is a major microvascular complication of type 2 diabetes leading to end stage renal disease. Mutations in NPHS2, encoding podocin have been identified in childhood onset focal segmental glomerulosclerosis, but have not been well characterised in diabetic kidney disease.
Aim: The present study was aimed to investigate the role of R229Q polymorphism of NPHS2 gene in type 2 diabetic patients with and without nephropathy from Andhra Pradesh, south India.
Methodology: We enrolled a total of 300 diabetic patients with nephropathy (150) and without nephropathy (150) to screen for R229Q polymorphism. Genotyping of the SNP was carried out by PCR-RFLP method.
Results: Overall frequency of the mutant allele A was found to be 0.24 in patients with type 2 diabetes and 0.30 in those with diabetic nephropathy, suggesting a lack of association of this polymorphism with susceptibility to diabetic nephropathy. Furthermore, patients carrying the mutant genotypes (GA,AA) with elevated levels of HbA1c were found to have poor kidney function parameters, illustrating the role of this polymorphism in the severity of diabetic nephropathy.
Conclusion: This is the first report from Andhra Pradesh, India pertaining to R229Q polymorphism of NPHS2 gene in type 2 diabetes. We put forth the notion that R229Q polymorphism of NPHS2 is influential in the severity of diabetic nephropathy rather than its susceptibility. Individuals with poor glycemic control and R229Q mutant genotype are at a higher risk of developing nephropathy in the studied population. This study has significance in the increasingscenario of diabetes and its complications. Large scale studies are needed that will shed light on gene and environment interactions and the role of this polymorphism in the severity of disease.
Keywords: Type 2 diabetes; Diabetic nephropathy; NPHS2; Podocin; Proteinuria; Genetic polymorphism
Introduction
Type 2 diabetes (T2D) is a metabolic disorder characterized by thepresence of hyperglycemia, insulin resistance and insulin deficiency. It is increasing at an alarming rate as a global health care problem [1,2]. Worldwide prevalence of diabetes in adults was 5.1% in 2003 and is predicted to increase to 6.3% by the year 2025 [3]. Longstanding diabetes is associated with several diabetic complications such as retinopathy, neuropathy, nephropathy and cardiovascular diseases. Forty percent of all the diabetic cases are known to be coupled with severe late vascular complications such a diabetic nephropathy (DN) [4]. Indian studies report the incidence of DN among T2D to be 5-9% and a leading cause of chronic renal failure [5]. Type 2 diabetic nephropathy (T2DN) is a progressive renal angiopathy of glomerular capillaries, characterised by nephrotic syndrome and diffuse glomerulosclerosis [6]. Associated clinical features of DN are persistent albuminuria, raised arterial blood pressure and a relentless decline in glomerular filtration rate (GFR) [7]. It is known that genetic and common environmental factors such as greater duration of diabetes, hypertension, poor metabolic control, smoking, obesity and hyperlipidemia predispose the diabetic patients to complications including diabetic nephropathy [8]. However, the cause for variation in the type of complications in different diabetic patients is not clear.
Recently, it has been demonstrated that injury to podocytes causes a decrease in their number thus leading to proteinuria and glomerulosclerosis [9]. Podocin, an integral membrane podocyte specific protein expressed in kidney, localised at slit diaphragm (SD) is required for the structural organization and regulation of the glomerular filtration barrier [10,11]. Both experimental models and human diseases have shown that alterations in the SD assembly lead to proteinuria. It is established that reduction in podocyte number is central to the development and progression of diabetic glomerulosclerosis [12,13].
Podocin encoded by NPHS2 gene spans approximately 25kb and is located on chromosome 1q25.2 containing 8 exons and 7 introns. It is a 42kD protein of stomatin family with 383-amino acids forming a hairpin structure with two cytoplasmic ends at the carboxy and amino terminus [14,15]. A large number of mutations have been reported in this gene in primary steroid resistant nephrotic syndrome (SRNS) [16]. Replacement of nucleotide (G to A) at position 755 in exon 5 (rs61747728) results in an arginine (R) to glutamine (Q) substitution at codon 229 [12]. R229Q one of the common variant of podocin is associated with lower binding affinity to nephrin affecting the stability of the functional unit. Hence this polymorphism is a likely candidate for the genetic susceptibility to diseases presenting with proteinuria. This mutation has been extensively studied in various populations in relation to kidney disorders [17-21]. The current study was aimed to investigate the distribution of R229Q polymorphism in T2D patients with and without nephropathy from Andhra Pradesh, India.
Materials and Methods
Sampling and data collection
The study group comprised a total of 300 T2D patients diagnosed by endocrinologist and nephrologist, of whom 150 were clinically identified with nephropathy (T2DN) and 150 patients without diabetic nephropathy (T2D) from three hospitals of Hyderabad, India. Demographic, anthropometric details like age,gender, height, weight, waist and hip measurements, family history of disease and duration of diabetes were recorded in a well-designed proforma. Body mass index (BMI) and waist to hip (W/H) ratio was calculated as given elsewhere [22]. Clinically diagnosed T2D patients with nephropathy and no other cause of renal disease were taken as T2DN patients. Inclusion criteria for T2D were subjects with longstanding diabetes for a period of 10 years with no history of hypertension prior to the development of diabetes. Venous blood was drawn and distributed in vaccutainers containing EDTA and clot activator. Clot activator tube was allowed to stand for one hour to obtain serum. Serum was transferred in eppendorf tube and stored at -20°C until analysis. The present study was carried out in accordance with Helsinki Declaration and ethical clearance was obtained from Ethics committee of Osmania University, Hyderabad, India. Informed consent was obtained from all the participating patients prior to sample collection.
Biochemical analysis
Biochemical details of fasting blood sugar (FBS), post lunch blood sugar (PLBS) were obtained from the medical records of the hospitals. Glomerular filtration rate (GFR) was calculated using Cockroft Gault formula [8]. Glycosylated hemoglobin (HbA1c) levels were estimated with a Nycocard reader (Axis-Sheild, Norway). Serum creatinine concentrations were determined by modified Jaffe’s method; serum albumin and blood urea were estimated using Bromocrisol green and urease method, respectively following manufacturers protocol (Span Diagnostics, India).
Genetic analysis
Genomic DNA was isolated from peripheral blood leukocytes using DNA extraction kits (Hi-media, India) as per instructions of the manufacturer and stored at -20°C until further use. Genotyping of R229Q polymorphism occurring within exon 5 of NPHS2gene was performed by PCR-RFLP method using specific primers (5’-GGATTTACCACAGGATTAAGTTGTGCA-3’ and 5’-AGCTATGAGCTCCCA AAGGGATGG-3’) [17]. PCR was accomplished in a total volume of 10μl containing 100ng of genomic DNA, 1μl of buffer, 0.25μl of d NTP’S, 0.18μl of forward and reverse primers each, 0.25μl of Taq polymerase [Labpro, India]. PCR amplification was carried out in an Eppendorf thermocycler under the following conditions; initial denaturation at 95°C for 5 min, denaturation at 94°C for 30 sec, annealing at 58°C for 45 sec, extension at 72°C for 5 min. The amplicons were digested overnight with ClaI enzyme which recognizes the sequence AT^CG_AT, at 37°C for genotyping. The G755A missense substitution results in a loss of ClaI site, mutant R229Q alleles gives a product of 545 bp as they miss the ClaI site, whereas the normal allele gives a digested product of 364 and 181 bp bands. Each batch of restriction digestion contained a positive control (confirmed G allele) to avoid mistyping. 10% of the samples were randomly picked and re-genotyped to give consistent results. The products were resolved on 2% agarose gel and analysed in a gel documentation unit (Figure 1).

Figure 1: Gel picture illustrating R229Q genotypes. Lane 1=100bp ladder;Lane 2, 5, 8, 9= Heterozygous GA; Lane 3= Homozygous AA; Lane 4, 6, 7=Homozygous GG.
Statistical analysis
Statistical analysis was performed using SPSS (IBM version 21.0). Student’s t test was used to analyze differences in biochemical and anthropometric characteristics such as BMI, W/H ratio, FBS, PLBS, HbA1c, serum creatinine, serum albumin, blood urea, eGFR and mean duration of diabetes. Mean and standard errorwere calculated as required. We used chi square test to evaluate the differences in genotype and allele frequencies and their deviation from Hardy Weinberg Equilibrium (HWE) among the studied subjects. The association between genotypes and various factors was evaluated by calculating the Odds Ratio (OR) at 95% confidenceinterval (C.I). One way analysis of variance (ANOVA) was used to compare genotypes with continuous variables. Relationship between the risk factors with DN was assessed through multiple logistic regression analysis with adjusted OR at 95% confidence intervals. A two tailed value of p < 0.05 was regarded as statistically significant.
Results
The present study dealt with R229Q SNP detection in a total of 300 diabetic patients with nephropathy (T2DN) and without nephropathy (T2D). The mean ages of the T2DN and T2D were 58.73±8.42 and 58.47±9.62 years, respectively, at the time of sample collection. The mean duration of diabetes in T2DN and T2D patientswas 12.78±7.26 and 14.24±4.89 years respectively. Anthropometric and clinical characteristics of the subjects enrolled in the study are displayed in Table 1. The analysis showed mean W/H ratio, HbA1c, FBS, PLBS, serum creatinine, serum albumin, blood urea, eGFR levels differed significantly among T2DN and T2D patients (p< 0.05).
The percentage distribution of R229Q genotypes GG, GA and AA among T2DN group was 43.3%, 54.7% and 2% whereas in T2D group it was 53.3%, 46% and 0.6%. There was no association observed with respect to genotypes between the two groups (χ2 =2.5; p >0.05). The mutant allele (A) frequency was 0.24 in T2D and 0.30 in T2DN patients correspondingly and the difference was not statistically significant (p >0.05). Genotype frequencies demonstrated significant deviation from Hardy Weinberg Equilibrium in both the groups (Table 2). ANOVA was carried out in order to study the genetic association of R229Q genotypes with kidney function parameters. A significant association of this polymorphism with respect to eGFR, proteinuria and serum creatinine (p< 0.05) was observed among T2DN group (Figure 2). However, no relation was found with respect to these parameters in T2D group. Multiple Logistic regression analysis of R229Q polymorphism with respect to BMI, W/H ratio, serum creatinine, HbA1c, blood urea, serum albumin was performed and a significant association of mutant genotypes with HbA1c and serum albumin was noted in patients with T2DN (Table 3).
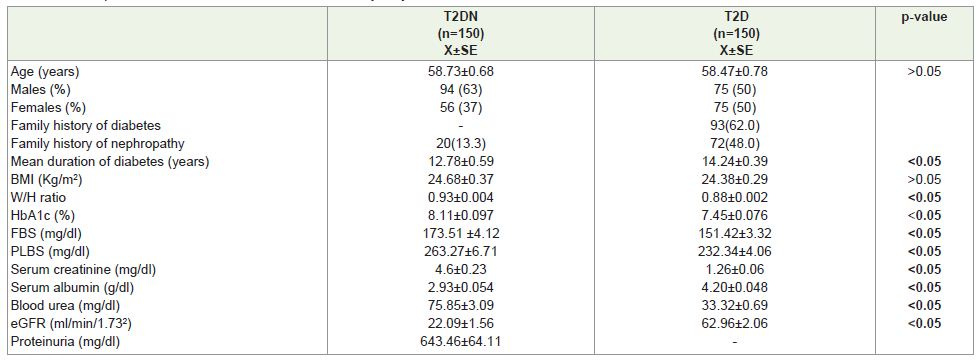
Table 1: Anthropometric and clinical features of the T2D study subjects.
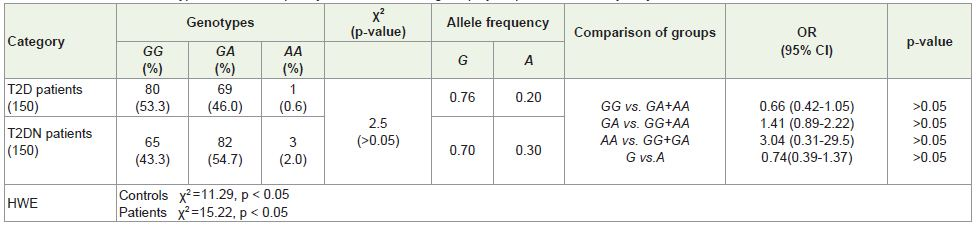
Table 2: Distribution of Genotype and allele frequency of NPHS2 R229Q gene polymorphism in the study subjects
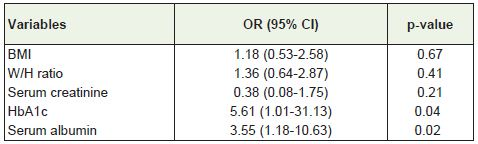
Table 3: Multiple logistic regression analysis for NPHS2 R229Q polymorphismwith respect to anthropometric and clinical features in T2DN patients.
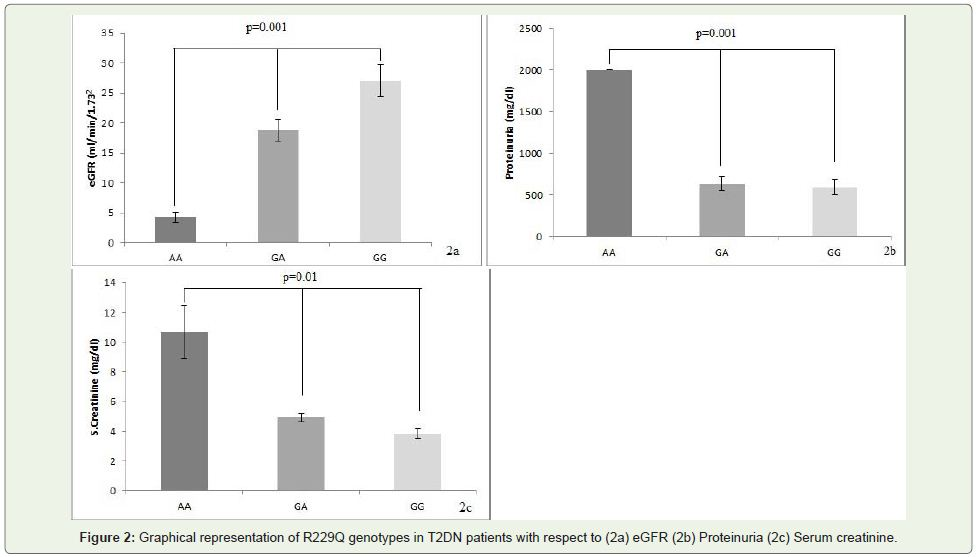
Figure 2: Graphical representation of R229Q genotypes in T2DN patients with respect to (2a) eGFR (2b) Proteinuria (2c) Serum creatinine.
Discussion
The present study is the first to look for the role of NPHS2 R229Q, a functional polymorphism in the susceptibility and severity of DN in type2 diabetic patients of Andhra Pradesh, India. A G755A substitution in exon 5 of NPHS2 gene (rs61747728) was not associated with susceptibility to DN in the studied population. However, the mutant genotypes were associated with severity upon interactionwith elevated levels of serum HbA1c. Diabetic nephropathy leading to end stage renal failure is a major cause of morbidity and mortality in patients with diabetes. Studies pertaining to familial clustering of DN suggest that genetic susceptibility plays a major role in the pathogenesis of nephropathy [23].
Our results showed mutant allele (A) frequency of 0.24 in T2D and 0.30 in T2DN group. A 10% difference between the two groups was seen with respect to the mutant genotypes (GA+AA) though the difference did not reach statistical significance; suggestive of no role of R229Q in the susceptibility to diabetic nephropathy. A small study from Tamil Nadu, India dealing with heterogenous group of chronic kidney diseases (glomerulonephritis= 37; diabetic nephritis= 24; interstitial nephritis= 9; hypertensive nephrosclerosis= 18; others =30) has reported A allele frequency to be 0.009 [21]. Another study from Czech population found R229Q polymorphism in 12% of Focal segmental glomerulosclerosis patients and 10% of controls (p>0.05). There was uneven R229Q allele distribution throughout different populations, such as South Americans, Europeans, European Americans, Asians and Africans [24]. This indicates that R229Q is a common polymorphism in certain populations.
A large study with heterogenous group of different renal phenotypes from Brazil by Pereria et al. reported an association between microalbuminuria with heterozygous (GA) individuals of this polymorphism [18]. In our analysis we explored the involvement of R229Q polymorphism with kidney function parameters in a homogenous population of diabetic individuals from Andhra Pradesh. Out of the 300 study subjects, only three T2DN and one T2D were found to have homozygous R229Q mutation. We observed a significant difference among the three genotypes with the highest mean ± SE with respect to proteinuria and serum creatinine while with lowest GFR in AA group followed by GA and then GG (Figure 2). Thus highlighting the possible role of R229Q and its association with poor kidney function. Our results indicate the role of A allele in single and double dose in the severity of the clinical conditions. Reiterova et al. reported that the heterozygosity of R229Q polymorphism was in higher prevalence in patients with progressive form of primary kidney disease compared to the stable form [24]. Hence, based on the above observations we suggest that the mutant podocin with lower binding affinity towards nephrin may contribute to the severity of diabetic nephropathy.
A significant association of the mutant genotype with HbA1c and serum albumin was observed in T2DN patients but not in T2D in our study population. A recent report suggests that a fluctuated level of HbA1c in diabetic individuals is a risk factor towards diabetic nephropathy [25]. The R229Q variant may require an additional hit in the form of hyperglycemic injury to act as a genetic risk factor for nephropathy to exert an adverse effect. It appears to be a good example of gene and environment interaction, wherein individuals carrying the mutant allele and a poor glycemic control are predisposed towards developing nephropathy.
Conclusion
The present study is a first of its kind analysing the association of R229Q in T2D patients from Andhra Pradesh, India. We put forth the notion that R229Q polymorphism of NPHS2 is influential in the severity of DN rather than its susceptibility. Individuals with poor glycemic control and R229Q mutant genotype are at a higher risk of developing nephropathy in the studied population. This study has significance in the increasing scenario of diabetes and its complications. However studies with larger populations are warranted which may throw light on the involvement of this common polymorphism in diabetic nephropathy.
Acknowledgement
The authors acknowledge OU-DST-PURSE for financial support in carrying out the study. We thank all the study subjects for their will full participation. Our special thanks to Dr. Prasanna Latha K and Md. Khalid Pasha for their contribution in drafting the manuscript.
References
- Goldenberg R, Punthakee Z (2013) Clinical practice guide lines. Definition, classification and Diagnosis of Diabetes, Prediabetes and Metabolic Syndrome. Canadian Diabetes Association Clinical Practice Guideline Expert Committee. Can J Diabetes 37: S8-S11.
- Hossain P, Kawar B, Nahas ME (2007) Obesity and Diabetes in the developing world-A growing challenge. N Engl J Med 356: 3.
- Sicree R, Shaw J, Zimmet P (2003) Diabetes and impaired glucose tolerance: In diabetes Atlas, Inter National Diabetes Federation Third Edition: Edited by Gan D. IDF, Belgium 15-72.
- United States Renal Data System (USRDS). Annual Data Report, Bethesda, MD; National Institute of Diabetes and Digestive and Kidney Diseases: National Institute of Health, U.S., Department of Health and Human Services: 2007.
- Appel G (2013) Detecting and controlling diabetic nephropathy: What do we know? Cleve Clin J Med 80: 209-217.
- Vishwanathan V (2004) Prevention of diabetic nephropathy: A diabetologist’s perspective. Indian J Nephrol 14: 157-162..
- Latha T, Jaganmohan P, Subramanyam P (2012) Evaluation of Diabetic Nephropathy using selected biochemical markers in settiyar (Vysya) community of Nellore and Prakasam Districts of Andhra Pradesh. Advan Biol Res 6: 81-86.
- Dabla PK (2010) Renal function in diabetic nephropathy. World J Diabetes 20:48-56.
- Suztak K, Raff AC, Schiffer M, Bottinger EP (2006) Glucose -Induced Reactive Oxygen Species Causes Apoptosis of Podocyte and Podocyte Depletion at the Onset of Diabetic nephropathy. Diabetes 55: 225-233.
- Mundel P, Shankland SJ (2002) Podocyte biology and response to injury. J Am Soc Nephrol 13: 3005-3015.
- Jaffer AT, Ahmed WU, Raju DS Jahan P (2011) Foothold of NPHS2 mutations in primary nephrotic syndrome. J Postgrad Med 57: 4
- Caridi G, Perfumo F, and Ghiggeri GM (2005) NPHS2 (podocin) Mutations in Nephrotic syndrome. Clinical Spectrum and Fine Mechanism. Pediatr Res 57: 54R-61R.
- Petermann AT, Kroft R, Blonski M, Hiromura K, Vaughn M, et al. (2003) Podocytes that detach in experimental membranous nephropathy are viable. Kidney Int 64:1222-1231.
- Asra J, Unnisa W, DSB Raju, Parveen Jahan (2014) NPHS2 mutation analysis and primary nephrotic syndrome in southern Indians. Nephrology 19: 398-403.
- Tabassum A, Rajeshwari T, Soni N, DSB Raju, Mukesh Y, et al. (2014) Structural Characterization and Mutational Assessment of Podocin - a novel drug target to Nephrotic Syndrome -an Insilico approach. Interdiscip Sci Comput Life Sci 6: 32-39.
- Franceschini N, North KE, Kopp JB, McKenzie L, Winkler C (2006) NPHS2 gene, nephrotic syndrome and focal segmental glomerulosclerosis: a HuGE review. Genet Med 8: 63-75.
- Tsukaguchi H, Sudhakar A, Le TC, Nguyen T, Yao J, et al. (2002) NPHS2 mutations in late-onset focal segmental glomerulosclerosis: R229Q is a common disease associated allele. J Clin Invest 110: 1659-1666.
- Pereria AC, Pereria AB, Mota GF, Cunha RS, Herkenhoff FL, et al. (2004) NPHS2 R229Q functional variant is associated with micro albuminuria in the general population. Kidney Int 65:1026-1030.
- Anbazhagana K, Sampathkumar K, Ramakrishnan M, Gomathi P, Gomathi S, et al. (2009) Analysis of polymorphism in Renin Angiotensin System and other related genes in South Indian chronic kidney disease patients. Clin Chim Acta 406: 108-112.
- Tonna SJ, Needham A, Polu K, Uscinski A, Appel GB, et al. (2008) NPHS2 variation in focal and segmental glomerulosclerosis. BMC Nephrology 9: 13.
- McKenzie LM, Hendrickson SL, Briggs WA, Dart RA, Korbet SM, et al. (2007) NPHS2 Variation in Sporadic Focal Segmental Glomerulosclerosis. J Am Soc Nephrol 18: 2987-2995.
- Snehalatha C, Vishwanathan V, Ramachandran A (2003) Cut off values for normal anthropometric variables in Asian Indian Adult. Diabetes care 26: 1380-1384.
- Evens KG, George RA, Sharma K Ziyadeh FN, Spielman RS (2005) Assesement of 115 Candidate Genes for Diabetic Nephropathy by Transimission/Disequilibrium Test. Diabetes 54: 3305-3318.
- Reiterova J, Safrankova H, Obeidova L, Stekrova J, Maixnerova D, et al. (2012) Mutational analysis of the NPHS2 gene in Czech patients with idiopathic nephrotic syndrome. Folia Biol (parah) 58: 64-68.
- Fares JE, Kanna M, Chaaya M, Azar ST (2010) Fluctuations in glycosylated haemoglobin (HbA1c) as a predictor for the development of diabetic nephropathy in type1diabetic patients. Inter J Diabetes Mellitus 2: 10-14.