Review Article
Role of Conformation Sensitive Gel Electrophoresis in Identifying Mutations in Glanzmann’s Thrombasthenia Patients
Meganathan Kannan
Corresponding author: Meganathan Kannan, Assistant Professor, Department of Life Sciences, School of Basic and AppliedSciences, Central University of Tamil Nadu, Thiruvarur, India,; E-mail: meganathank@cutn.ac.in; kannanmd77@gmail.com
Citation: Kannan M. Role of Conformation Sensitive Gel Electrophoresis in Identifying Mutations in Glanzmann’s Thrombasthenia Patients. J Cell Sci Molecul Biol. 2014;1(1): 104.
Copyright © 2014 Meganathan Kannan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Cell Science & Molecular Biology | Volume: 1, Issue: 1
Abstract
Glanzmann’s Thrombasthenia (GT) is an inherited platelet function disorder due to a defect in platelet glycoprotein αIIb and / or β3. For the detection of unknown mutations affecting the genes αIIb and β3, screening techniques followed by sequencing are in use. Mutation screenings, such as Single Stranded Conformation Polymorphism (SSCP), Denaturing Gradient Gel Electrophoresis (DGGE) andConformation Sensitive Gel Electrophoresis (CSGE) are useful methods in analyzing patients group in a larger volume. The phenotypic variability of hematological disorders can be explained using these techniques. However, low cost and high detection efficiency techniques are preferred, particularly, in developing countries. In our experience, we studied a platelet function disorder in a larger volume using the technique, CSGE, which is comparatively an efficient, low cost and high throughput for the mutation screening in a larger volume. The study included 45 GT patients to analyze the mutation in the genes ITGA2B and ITGB3 which code for αIIb and β3 respectively. Mutation screening, followed by sequencing, revealed mutations in 80% unrelated GT patiets. In our experience, CSGE is helpful in finding the mutations in GT patients.
Keywords: Mutation screening; CSGE; Glanzmann’s Thrombasthenia
Introduction
Mutation screening is an economic approach in the DNA analysis that enables mutation detection, proper genetic counseling, carrier detection and prenatal diagnosis in inherited bleeding disorders. Glanzmann’s Thrombasthenia (GT) is an autosomal recessive inheritance with a world- wide distribution [1-5]. The clinical complications in GT include lifelong bleeding with easy bruising, epistaxis, menorrhagia and gastrointestinal bleeding [6,7]. GT is caused by mutations in the genes ITGA2B and ITGB3, which encode αIIb or β3 respectively that result in qualitative or quantitative abnormalities of the platelet membrane proteins [8-13]. GT occurs in high frequency in certain ethnic populations with an increased incidence of consanguinity such as in Indians, Iranians, Iraqi Jews, Palastinian and Jordanian Arabs and French Gypsies. A nationwide survey in Japan identified 192 GT patients in 1991 [14]. The highest frequency of GT is found in the Iraqi-Jewish population in which 700 cases have been analyzed for molecular defects [15]. A review of 177 patients with GT has been reported that include 12 GT patients from United States, 55 patients were from Israel and Jordan, and 42 from South India [7]. In certain ethnic groups, such as South Indian Hindus, Iraqi Jews, French gypsies and Jordanian nomadic tribes, thrombasthenia may actually be a common hereditary hemorrhagic disorder. GT is relatively frequent in some highly inbred populations such as Indians [16]. The high incidence of this disorder suggests the need of cost-effective, high efficient screening techniques in analyzing the genetic defect. Mutation screenings, such as Single Stranded Conformation Polymorphism (SSCP), Denaturing Gradient Gel Electrophoresis (DGGE) and Conformation Sensitive Gel Electrophoresis (CSGE) are the appropriate techniques especially when analyzing patients group in a larger volume.
Single Stranded Conformation Polymorphism (SSCP) is a technique based on polymorphic differences in strand mobility result from the effects of primary sequence changes on the folded structure of a single strand of DNA [17,18]. The primary sequence changes alter the intramolecular interactions that generate a three-dimensional folded structure [19]. The molecules may thus move at a different rate through a non-denaturing gel. SSCP involves the amplification by PCR of a discreet segment of genomic DNA, denaturing the doublestranded DNA into single strands and analysis on a non-denaturing polyacrylamide gel. SSCP has been used to analyze genetic mutations in patients with Glanzmann’s Thrombasthenia [20-23]. Though the method is simple to perform, it is time consuming and less sensitive to pick up genetic variations. This technique has the overall sensitivity of 70%. However, a study from western part of India reported that, along with other mutation screening, the SSCP failed to identify mutations in 50% (12 out of 22 GT patients) of the GT patients [24]. There are multiple conditions of analysis that can be applied to increase the sensitivity [25]. However, a major limitation for SSCP is fragment sizes which sometimes determine the sensitivity of the technique to detect mutations [26].
Denaturing Gradient Gel Electrophoresis (DGGE) is a technique involves the amplification of DNA by PCR followed by electrophoresis through a gradient of increasing concentration of a denaturing agent (such as urea or formamide) or temperature leading to a partial melting of the double stranded DNA around the Tm of the mutated region. This results in an abrupt decrease in the mobility of the DNAfragment [27-32]. This assay requires the presence of both a wild-type allele and a mutant allele is and therefore very sensitive in identifying heterozygous carriers. In the literature, it has been reported that DGGE sensitivity is comparatively better than SSCP with a fragment length of up to 600 bp. This correlated with a report from France in which the investigators used DGGE for identifying sequence alterations in genes, that code glycoprotein IIb and IIIa, from 20 GT patients [33]. They identified mutations in 16 out of 20 GT patients (80%). Though the sensitivity of DGGE in detecting mutations of GT is better than SSCP, DGGE has the disadvantages of relatively lowthroughput in terms of sample analysis, complex primer design to include GC clamps in terms of extensive optimization and high cost in terms of special equipment.
Conformation Sensitive Gel Electrophoresis (CSGE) is a mutation-screening technique based on the principle of heteroduplex formation. This method relies on the differential migration of DNA heteroduplex in comparison with homoduplex and is rapid and non-radioactive [34]. Patient’s DNA band is analyzed on the basis of appearance of additional or abnormal bands in comparison to the normal controls. An extensive visual examination of the CSGE gel is essential to compare all samples with the wide type DNA band. Samples containing additional/abnormal bands are further sequenced to determine the nature and position of the mutations or nucleotide change. The sequences are manually compared with the wild type sequence. CSGE is high efficient, low cost and its sensitivity is also higher than SSCP, hence can be used routinely. For fragments in the size range of 200–800 bp, sensitivity of 88% has been detected, and a reduction in the maximum size of the fragment has been associated with an increase in the detection rate [35,36]. Table 1 describes about the sensitivity of screening techniques in patients with Glanzmann’s Thrombasgthenia.
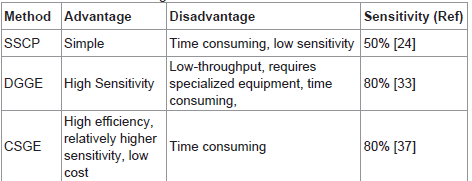
Table 1: Mutation screening in Glanzmann’s Thrombasthenia.
Mutation screening in Glanzmann’s Thrombasthenia: Ourexperience with CSGE
Previously, for the detection of mutations affecting αIIb and β3 genes, screening method like Single Stranded Conformation Polymorphism (SSCP) has been applied in most of the developing countries like India, but showed less sensitivity in mutation identification. Though other techniques like DGGE and dHPLC are high sensitive, because they require specialized equipment and high cost, we chose CSGE which is an enhanced method of mutation screening at low cost, to analyze the mutational defect in patients with Glanzmann Thrombasthenia. Nucleotide changes in either of ITGA2B or ITGB3 gene was screened first by CSGE followed by sequencing of defective exons. The study included 45 GT patients with an age ranging from 5 months to 46 years. GT was diagnosed in these patients on the basis of clinical and hematological parameters. CSGE involved DNA amplification by PCR, heteroduplex formation and gel run on Conformation Sensitive Gel Electrophoresis for all the 30 exons and promoter of the ITGA2B and 15 exons and promoter of ITGB3. 4 out of 45 GT patients did not show band shift in any of the exons of the ITGA2B and ITGB3. A total of 25 exons of ITGA2B and 12 exons of ITGB3 showed band sift by CSGE. 5 out of 30 exons (Exons 2,3,7,27 and 29) of ITGA2B and 3 out of 15 exons (Exons 4,8 and 11) of ITGB3 showed no band shift. Table 2 describes about the band shift identified by CSGE [38].
Sequencing revealed mutations in 36 of 45 (80%) unrelated GT patients. Of these, 22 patients (48.8%) showed defect in ITGA2B and 14 patients (31.1%) showed defect in ITGB3. In 9 out of 45 (20%) GT patients, no gene alterations were identified, however, their hematological tests including platelet aggregation and flow cytometryrevealed that they were definite GT. GT patients with no possible causative mutations were may be due to defect in a regulatory element affecting the transcription of the genes ITGA2B and ITGB3 [39]. CSGE also plays an important role in the detection of carrier status in families of GT patients [40]. Based on these results, we conclude that CSGE can successfully be applied in analyzing mutations in GT patients. This method of CSGE can be used not only to screen for mutations, but also helpful in identifying carrier status in family members of the patient. Once the defective exon and the mutation causing GT in the patient are identified, the same defect can be looked for in the family members using CSGE. Thus CSGE is an effective technique to screen for mutation not only in patients but also in family members. Once the defective exon in a patient is identified, the particular exon can be analyzed by CSGE in parents and siblings of the patient, before proceeding to direct sequencing Table 2.
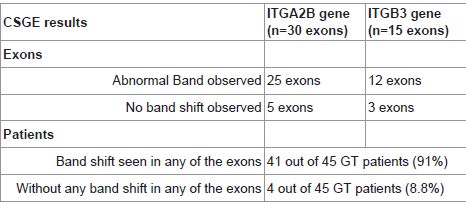
Table 2: Overall CSGE results.
Conclusion
In practice, no single screening technique can detect 100% mutation; however, a simple, rapid and high sensitive mutation screening is reasonable and may help in the mutation analysis. Single Stranded Conformation Polymorphism a is older method and less sensitive, moreover not reliable for fragment sizes greater than 200bp.Denaturing Gradient Gel Electrophoresis is reliable for mutation screening under controlled conditions, but, it requires use of GC clamp on one of the primers used for PCR and the optimization is difficult. Conformation Sensitive Gel Electrophoresis is simple, practical and has high detection efficiency at low cost. The sensitivity of CSGE is higher than conventional SSCP. Though other techniquesuch as Denaturing High-Performance Liquid Chromatography gives very high sensitive for mutation analysis, equipment is very costly and cannot be made available for routine use. In countries like India, Iran, Iraq and Palestine where an increased incidence of consanguinity is common, mutation techniques that involves highcost and low throughput are not preferred. Also, the need is in such that the technique should be high sensitive in detecting mutations and it should be affordable for routine use. Based on the above, and also based on our experience, it is clear that CSGE fulfills the need of high throughput samples, high sensitivity and low cost in mutation detection and thus plays an important role in identifying mutations. Thus it is concluded that mutation screening by CSGE is extremelyuseful in identifying mutations in patients affected with Glanzmann’s Thrombasthenia.
References
- Rosenberg N, Hauschner H, Peretz H, Mor-Cohen R, Landau M, et al. (2005) A 13-bp deletion in alpha(IIb) gene is a founder mutation that predominates in Palestinian-Arab patients with Glanzmann thrombasthenia. J Thromb Haemost 3: 2764-2772.
- Schlegel N, Gayet O, Morel-Kopp MC, Wyler B, Hurtaud-Roux MF, et al. (1995)The molecular genetic basis of Glanzmann's thrombasthenia in a gypsy population in France: identification of a new mutation on the alpha IIb gene. Blood 86: 977-982.
- Khanduri U, Pulimood R, Sudarsanam A, Carman RH, Jadhav M, et al. (1981) Glanzmann's thrombasthenia. A review and report of 42 cases from South India. Thromb Haemost 46: 717-721.
- Nurden AT (2006) Glanzmann thrombasthenia. Orphanet J Rare Dis 1: 10.
- Toogeh G, Sharifian R, Lak M, Safaee R, Artoni A, et al. (2004) Presentation and pattern of symptoms in 382 patients with Glanzmann thrombasthenia in Iran. Am J Hematol 77: 198-199.
- Seligsohn U, Rososhansky S (1984) A Glanzmann's thrombasthenia cluster among Iraqi Jews in Israel. Thromb Haemost 52: 230-231.
- George JN, Caen JP, Nurden AT (1990) Glanzmann's thrombasthenia: the spectrum of clinical disease. Blood 75: 1383-1395.
- Nurden AT, Pillois X, Wilcox DA (2013) Glanzmann thrombasthenia: state of the art and future directions. Semin Thromb Hemost 39: 642-655.
- Kannan M, Saxena R (2009) Glanzmann's Thrombasthenia: An Overview. Clin Appl Thromb Hemost. 15: 152-165.
- French DL (1998) The molecular genetics of Glanzmann’s thrombasthenia. Platelets 9: 5-20.
- Peretz H, Rosenberg N, Landau M, Usher S, Nelson EJ, et al. (2006) Molecular diversity of Glanzmann thrombasthenia in southern India: new insights into mRNA splicing and structure-function correlations of alphaIIbbeta3 integrin (ITGA2B, ITGB3). Hum Mutat 27: 359-369.
- D'Andrea G, Colaizzo D, Vecchione G, Grandone E, Di Minno G, et al. (2002) Glanzmann's thrombasthenia: identification of 19 new mutations in 30 patients. Thromb Haemost 87: 1034-1042.
- Coller BS, French DL (2001) Hereditary Qualitative platelet disorders. In Williams hematology, 6th ed. New York: McGraw Hill :1551-1581.
- Yasunaga K, Nomura S (1993) Statistical analysis of Glanzmann's thrombasthenia in Japan. Acta Haematol 89: 165-166.
- Rosenberg N, Yatuv R, Orion Y, Zivelin A, Dardik R, et al. (1997) Glanzmann thrombasthenia caused by an 11.2-kb deletion in the glycoprotein IIIa (beta3) is a second mutation in Iraqi Jews that stemmed from a distinct founder. Blood 89: 3654-3662.
- Kannan M, Ahmed RPH, Paresh J, Rajive Kumar, Saxena R. Type I Glanzmann Thrombasthenia: Commonest subtypes in North Indians. Am J Hematol. 2003 Oct; 74(2):139-41.
- Scoggan KA, Bulman DE (2002) Single-Strand Conformational Polymorphism Analysis (SSCP) and Sequencing for Ion Channel Gene Mutations. Methods in Molecular Biology 217: 143-151.
- Hongyo T, Buzard GS, Calvert RJ, Weghorst CM (1993) 'Cold SSCP': a simple, rapid and non-radioactive method for optimized single-strand conformation polymorphism analyses. Nucleic Acids Res 21: 3637-3642.
- Orita M, Iwahana H, Kanazawa H, Hayashi K, Sekiya T (1989) Detection of polymorphisms of human DNA by gel electrophoresis as single-strand conformation polymorphisms. Proc Natl Acad Sci U S A 86: 2766-2770.
- Ruan J, Peyruchaud O, Nurden P, Cazes E, Combrié R, et al. (1998) Family screening for a Glanzmann's thrombasthenia mutation using PCR-SSCP. Platelets 9: 129-136.
- Jin Y, Dietz HC, Montgomery RA, Bell WR, McIntosh I, et al. (1996) Glanzmann Thrombasthenia: Cooperation between Sequence Variants in Cis during Splice Site Selection. J Clin Invest 98 1745-1754..
- Garcia LC, Breillat C, Lima M, Combrié R, Morais S, et al. (2004) Mutations in the beta3 gene giving rise to type I Glanzmann thrombasthenia in two families in Portugal. Platelets 15: 15-22.
- Milet-Marsal S, Breillat C, Peyruchaud O, Nurden P, Combrié R, et al. (2002) Two different beta3 cysteine substitutions alter alphaIIb beta3 maturation and result in Glanzmann thrombasthenia. Thromb Haemost 88: 104-110.
- Nair S, Ghosh K, Shetty S, Mohanty D (2005) Mutations in GPIIIa molecule as a cause for Glanzmann thrombasthenia in Indian patients. J Thromb Haemost 3: 482-488.
- Ravnik-Glavac M, Glavac D, Dean M (1994) Sensitivity of single-strand conformation polymorphism and heteroduplex method for mutation detection in the cystic fibrosis gene. Hum Mol Genet 3: 801-807.
- Sheffield VC, Beck JS, Kwitek AE, Sandstrom DW, Stone EM (1993) The sensitivity of single-strand conformation polymorphism analysis for the detection of single base substitutions. Genomics 16: 325-332.
- Steers F, Wallace, M, Johnson P, Carritt B, Daniels G (1996) Denaturing gradient gel electrophoresis: a novel method for determining Rh phenotype from genomic DNA. Br J Haematol 94: 417-421. .
- Fischer SG, Lerman LS (1983) DNA fragments differing by single base-pair substitutions are separated in denaturing gradient gels: correspondence with melting theory. Proc Natl Acad Sci U S A 80: 1579-1583.
- Liu T (2010) Mutational screening of hMLH1 and hMSH2 that confer inherited colorectal cancer susceptibility using denature gradient gel electrophoresis (DGGE). Methods Mol Biol 653: 193-205.
- Goeldel AL, Cornillet-Lefebvre P, Durlach A, Birembaut P, Bernard P, et al. (2010) T-cell receptor gamma gene rearrangement in cutaneous T-cell lymphoma: comparative study of polymerase chain reaction with denaturing gradient gel electrophoresis and GeneScan analysis. Br J Dermatol 162: 822-829.
- Costabile M, Quach A, Ferrante A (2006) Molecular approaches in the diagnosis of primary immunodeficiency diseases. Hum Mutat 27: 1163-1173.
- Siqueira JF Jr, Rôças IN, Rosado AS (200) Application of denaturing gradient gel electrophoresis (DGGE) to the analysis of endodontic infections. J Endod 31: 775-782.
- 33.Vinciguerra C, Bordet JC, Beaune G, Grenier C, Dechavanne M, et al. (2001) Description of 10 new mutations in platelet glycoprotein IIb (alphaIIb) and glycoprotein IIIa (beta3) genes. Platelets 12: 486-495.
- Ganguly A (2002) An update on conformation sensitive gel electrophoresis. Hum Mutat 19: 334-342.
- Korkko J, Annunen S, Pihlajamaa T, Prockop DJ, Ala-Kokko L (1998) Conformation sensitive gel electrophoresis for simple and accurate detection of mutations: comparison with denaturing gradient gel electrophoresis and nucleotide sequencing. Proc Natl Acad Sci U S A 95: 1681-1685.
- Taylor CF, Taylor GR (2004) Current and emerging techniques for diagnostic mutation detection: an overview of methods for mutation detection. Methods Mol Med 92: 9-44.
- Kannan M, Ahmad F, Yadav B, Kumar R, Choudhry V, et al. (2009) Molecular defects in ITGA2B and ITGB3 genes in patients with Glanzmann’s thrombasthenia. J Thromb Haemost 7: 1878-1885.
- Kannan M, Ahmad F, Yadav BK, Kumar R, Saxena R (2007) Mutation screening of GPIIb and GPIIIa exons by Conformation sensitive gel electrophoresis. Blood 110: 3218.
- Kannan M, Ahmad F, Kumar R, Choudhry VP, Saxena R (2006) Use of CSGE, TspRI- RFLP and Western Blot in Carrier Detection in an Indian Family with Type I Glanzmann Thrombasthenia. Blood 108: 3975.
- Kannan M, Ahmad F, Yadav BK, Kumar P, Jain P, et al. (200) Carrier detection in Glanzmann’s Thrombasthenia: Comparison of flow cytometry and western blot with respect to DNA mutation. Am J Clin Pathol 130: 93-98.