Review Article
Transdermal Nanocarriers: New Challenges and Prospectives in the Treatment of Diabetes mellitus
Gangadhara Angajala, R Subashini*
Corresponding author: Chemistry Research Laboratory, Organic Chemistry Division, School of Advanced Sciences, VIT University, Vellore - 632014, Tel: +91 94435 41305, +91 0416 2202352, E-mail: dr.subashini.r@gmail.com
Citation: Angajala G, Subashini R. Transdermal Nanocarriers: New Challenges and Prospectives in the Treatment of Diabetes mellitus. J Chem Applied Biochem. 2014;1(2): 107.
Copyright © 2014 Angajala et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Chemistry & Applied Biochemistry| Volume: 1, Issue: 1
Abstract
In recent years nanotechnology in drug delivery systems has opened new areas for sustained release of therapeutic drugs to the site of action. The new generation of modern drug delivery systems has more advantages than their traditional systems. Infact wide spectrum applications of nanotechnology in pharmaceutical formulations are changing the scientific landscape of diagnosis, treatment and prevention of diseases. Various pharmaceutical nanotechnology based systems which can be termed as nanopharmaceuticals have brought about revolutionary changes in drug delivery as well as in the field of nanomedicine. Today 75% of drugs are taken through oral route and are found not to be as effective as desired. To improve such characters transdermal drug delivery system was emerged. Administration of therapeutic agents topically offers many advantages over conventional, oral and invasive methods of drug delivery. Several important advantages of transdermal drug delivery are limitation of hepatic first pass metabolism, enhancement of therapeutic efficiency and maintenance of steady plasma level of the drug. The present review summarizes the most important applications of nanotechnology in drug delivery systems, the need for transdermal drug delivery systems, their advantages, limitations and the recent developments of such systems in the treatment of diabetes.
Keywords: Nanotechnology; Drug delivery; Diabetes; Transdermal nanocarriers
Introduction
Over the past few years nanotechnology is rapidly expanding, encircling the development of man-made materials in the range of 5-200 nanometer size range. Nanotechnology mainly deals with the design, synthesis and characterization on ultra small particles which is extended to broad area in pharmaceutical, medical, chemical and engineering application due to its unique properties [1,2]. The changes in properties of nanomaterials are mainly due to increase in surface area and dominance of quantum effects which is associated with very small sizes and large surface area to volume ratio. Nanoparticles demonstrate unique properties with potentially wide range of applications and thereby provides useful platform to explore various interdisciplinary fields. In medicine one of the important applications of nanotechnology is the use of nanomaterials in drug delivery systems to target tissue for the treatment of various diseases. Inspite of the limitations associated with the use of traditional medicine systems, there is also lack of target specificities, which further reduce the therapeutic efficacy of drug during its metabolism in the body and also the cellular toxicity of some of the drug molecules [3,4]. At present 95% of the all potential therapeutics have poor pharmacokinetics and biopharmaceutical properties. Therefore there is an effective need to develop suitable drug delivery systems that distribute the active drug molecule only to the site of target organ without affecting the healthy organs and tissues. In recent years, there has been tremendous growth in nanotechnology in the field of medicine especially in targeted drug delivery systems. In nanomedicine, the main goal is to diagnose and preserve health without side effects by using non invasive treatments [5]. The increase in surface area, versatility in target tissues, controlled drug release, solubility, and site-targeted drug delivery are some of the noteworthy characteristics that nanotechnology can contribute in drug-delivery systems. The strategy that the nanomedicine provides to the drugs and other materials in the nanometer scale (1-500 nm) can change the basic properties and improve the bioactivity of materials. With the development in nanotechnology it is now possible to generate drug nanoparticles that can increase drug efficiency and reduce side effects. Surface modifications of nanomaterials have strong effect on the interaction of these nanomaterials with cells in addition to this is also helps to covert toxic nanomaterial to less toxic form [6,7].
Recent advances in nanoparticulate systems for improved drug delivery exhibit a great potential for the successful administration of wide variety of active pharmaceuticals. The quantum effects at nanoscale determine a material’s magnetic, thermal, optical and electrical properties [8]. It is generally expected that products at nanoscale will be cheaper and economically reliable because of less quantity of materials utilized during the process. Nature is considered as the ultimate source in nanotechnology which provides nanostructures that offer various functional proteins and many other biological compounds at cellular level which brings great significance to life on earth. Many biological systems in nature originated through a process of complex dynamic self-assembly comprising partition and separation of many substances into the desired pattern. Some biological systems contain nanosystems that are devoted to specific functions such as locomotion in protozoans, where actin moves along with myosin and kinesin moves along with microtubules. It is considered that one of the functions of proteins and compounds that exist at cellular level is that of nanotechnological separations. Thus a DNA molecule can be seen as a self-assembly machine which replicates itself and also produces complex organisms under the right conditions, subsequently, ribosomes construct protein molecules with accuracy following instructions from DNA. Further molecular motors that construct human muscles are recognized as sophisticated nanomachines that possess ability to convert chemical energy to mechanical energy with high efficiency [9].
Nanoparticles have been used to enhance the selectivity and efficiency of the drug delivery system because they act as mediators of drug release. Due to their extremely small size and large surface area there is possibility to further modify the surface with hydrophobic, hydrophilic, cationic, anionic or any neutral moieties to the surrounding environment which increases their targeting potential applications in biological sciences. The advancement of nanoparticle assisted drug delivery is widely expected to change the landscape of pharmaceutical industries in near future [10]. By virtue of their unique physico chemical properties, nanoparticles have shown promise in delivering a range of molecules to the defined target sites in the body. This special property of nanoparticles makes them a favourable material for biomedical applications. Nanotechnology induced advance approaches in the field of medicine regarding efficient drug delivery have been used especially in the treatment of diabetes. Nanotechnology is quite deliberate in developing modern drug delivery technologies which can expand drug markets. Nanotechnology can be used to reformulate already existing drugs thereby enhancing their overall performance, improve their stability, acceptability by increasing effectiveness, as well as safety and patient adherence, and eventually reduce health care costs [11,12]. Nanotechnology may also increase the performance of drugs that are unable to pass clinical trial phases.
India, the world’s second most populous country, now has more people with type 2 diabetes than any other nation. Diabetes mellitus describes a metabolic disorder of multiple etiologies characterized by chronic hyperglycemia with disturbances of carbohydrate, fat and protein metabolism resulting from defects in insulin secretion, insulin action, or both. With the spread of fast-food outlets and more sedentary lifestyles, the prevalence of diabetes throughout the world is rising alarmingly [13]. Despite many advances in the development of oral hypoglycaemic agents, an ideal drug for treating Type 2 diabetes is still a distant reality [14]. Today, physicians can prefer from among a variety of medications targeting various stages of disease, but each drug class associated with some side effects. The age-old molecules such as biguanides and sulfonylureas are still considered drugs of choice because of their well-studied mechanism of action, better tolerability, safety and ideal pharmacodynamic effects. The prevalence of type 2 diabetes has reached epidemic proportions and is continuously increasing all over the world [15].
As per global estimates predict that the total number of cases of diabetes were about 250 million in the year 2013, which represents a 60% increase in the prevalence compared to the year 2002, and prediction is that there will be about 380 million cases in the year 2030. This scenario clearly makes understanding of the pathogenesis of type 2 diabetes crucial in order to implement rational treatment strategies. Type 2 diabetes results from an insufficient compensatory insulin secretion to insulin resistance. Mostly insulin resistance is an early event due to environmental factors, obesity and β-cell function decline a gradual but generally late event. Major goals of management of diabetes in patients are to lower the incidence of degenerative complications and the risk of fatal or non-fatal health events, to improve quality of life, and to increase life expectancy. Some high incidence of concomitant gastrointestinal symptoms, such as abdominal discomfort, nausea, and diarrhoea, may occur during the treatment [16-18].
Recent advances in nanoparticulate systems for improved drug delivery display a great potential for the administration of wide variety of active pharmaceuticals. Many approaches have been used to enhance the penetration of drugs through skin. The role of these systems in the long-term treatment of diabetes, however, remains debatable. Especially questionable are those methods involving physical or chemical disruption of the skin, which might cause chronic pathological changes. Until we find an ideal drug for the treatment of type 2 diabetes, there is much possibility and interest for leading pharmaceutical companies to modify the pharmacokinetics of old drug molecules in order to better suit for larger sections of patients [19-22]. This review is an attempt to compile and describe various advances in drug delivery systems for the management of diabetes, particularly the extended and sustained release formulations of metformin and glipizide both of which have great potential in treatment of Type 2 diabetes mellitus.
Role of nanocarriers in drug delivery
In the area of drug delivery various efforts have been undertaken by scientists from all over the world for the development of effective targeted delivery system in which the drug is only active in the target area of the body and sustained release formulations in which the drug is released over a period of time in a controlled manner from a formulation. Several therapeutic nanocarriers for different drug delivery systems have been approved and most of them are in clinical use [23]. These drug delivery systems are broadly categorized into four principle routes namely oral, transdermal, inhalation and parenteral. The primary route for the delivery of any drug therapy is through oral administration with once or twice daily dosing. However, there is large number of therapies particularly vaccine-based, proteinbased, gene-based that cannot be delivered by this route. Pulmonary delivery is another non-invasive substitute method that is appropriate for small molecules and proteins. Some of the challenges of most drug delivery systems currently facing include in-vivo stability, solubility, intestinal absorption, poor bioavailability, sustained and targeted delivery to site of action, therapeutic effectiveness, side effects, and plasma fluctuations of drugs which either fall below the minimum effective concentrations or exceed the safe therapeutic concentrations. However, nanodrug delivery is an efficient approach primarily focussed to overcome these challenges due to fabrication and development of nanostructures at submicron scale and nanoscale with multiple advantages [24,25].
Generally, nanostructures have the capability to protect drugs encapsulated within themselves from enzymatic and hydrolytic degradation in the gastrointestinal tract, target the delivery of a wide range of drugs to different parts of the body for sustained release. They deliver drugs that are highly water insoluble and in addition to this it can also bypass the liver, thereby preventing the first pass metabolism of the incorporated drug. These nanocarriers increase oral bioavailability of drugs due to their specific uptake mechanisms such as absorptive endocytosis and are able to stay in the blood circulation for a longer period, releasing the incorporated drug in a sustained and controlled manner leading to less plasma fluctuations thereby minimizing side-effects and toxicity caused by drugs. Due to the small size of nanostructures, they possess the ability to penetrate deep inside the tissues and are effectively taken up by cells, allowing efficient delivery of drugs to site of action. The uptake of nanostructures was found to be 15-200 times faster than that of microparticles in the 1-10μm range. For targeted delivery, nanostructures can be conjugated with various drug molecules so that the linkage between the polymer and the lead substance can be manipulated to control the site and duration of action at which the drug is released. The linkage may be achieved by incorporation of lipids, amino acids, peptides or small chains as spacer molecules [26].
Transdermal nano drug delivery systems
The utilization of transdermal nanocarriers have significantly increased in the last few decades. These systems are designed around the two special features that are required in the modern pharmacy which includes temporal delivery and spatial location. Transdermal delivery has variety of advantages compared to the oral route [27-34]. Perhaps the greatest challenge for transdermal drug delivery is that only a limited number of drugs are amenable to administration by this route. It is very difficult to say which the ideal nanocarrier is, because every day new advantages and disadvantages of each carrier are being discovered (Figure 1). An important point highlighted by Panariti et al. [35] is that the interaction with various biological systems and nanocarrier cell internalization is determined by physicochemical properties of nanocarrier systems.
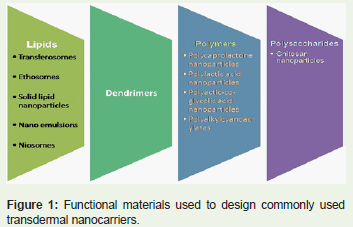
Figure 1: Functional materials used to design commonly used transdermal nanocarriers.
The main physicochemical properties that affect and influence cellular uptake are size, shape, rigidity, and charge in the surface of nanoparticles (Table 1). Nanoparticulated systems can be administered into organisms by almost all routes including transdermal which offers several advantages over other delivery systems (Figure 2) but with its own limitations (Table 2). Transdermal route of drug administration have unique advantages, the drug can easily bypass the first pass metabolism and reaches the systemic circulation. Painless, non invasive and patient-friendly application of patches offers good patient compliance and patches are also easy to remove in the event of hyperinsulinemia [36-39]. An overview of various transdermal nanocarriers has been depicted in Figure 3.
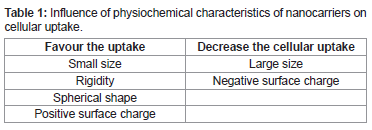
Table 1: Influence of physiochemical characteristics of nanocarriers on cellular uptake.
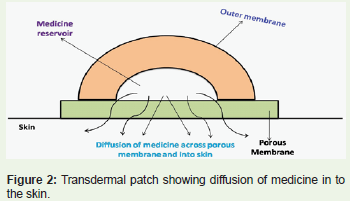
Figure 2: Transdermal patch showing diffusion of medicine in to the skin.
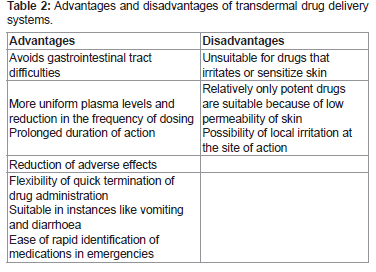
Table 2: Advantages and disadvantages of transdermal drug delivery systems.
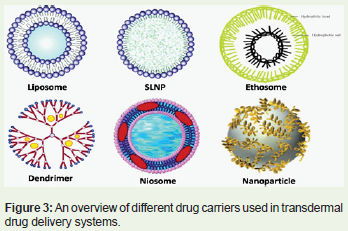
Figure 3: An overview of different drug carriers used in transdermal drug delivery systems.
Different nanocarriers for TDDS
Liposomes
Liposomes are spherical, self-closed structures formed by one or several concentric lipid bilayers with an aqueous phase inside and between the lipid bilayers. Liposomes are biocompatible which can entrap water-soluble pharmaceutical agents in their internal water compartment and water-insoluble pharmaceuticals into the membrane. Liposomes usually provide a unique opportunity to deliver pharmaceuticals into cells or even inside individual cellular compartments. Size, charge and surface properties of liposomes can be easily changed simply by adding new ingredients to the lipid mixture before liposome preparation by variation of preparation methods [40]. Liposomes have become one of the pharmaceutical nanocarriers of choice for many purposes. In recent years, many liposome-based drugs and biomedical products have been approved for use as medicines. The transdermal penetration of liposomes are usually affected by many factors eg, formulation and particle size, as well as the presence of penetration enhancers but there are other important variables like lamellarity, lipid composition, charge on the liposomal surface, mode of application, and total lipid concentrations [41]. Liposomes can be designed to adhere to cellular membranes to deliver a drug payload or simply transfer drugs following endocytosis [42].
Liposomes have been used successfully to transport drugs across the skin. Biologically active materials encapsulated within liposomes are protected to varying extent from immediate degradation or dilution, suggesting drug delivery systems for the transport of drugs and other bioactive capsules to disease infected organs. The unique ability of liposomes to entrap drugs both in an aqueous and a lipid phase make such delivery systems attractive for hydrophilic and hydrophobic drugs. Hashimoto et al, have demonstrated the effect of orally administered insulin liposomes on alloxan diabetic rats. When the liposomes were administered orally to rats in the 3rd phase of acute alloxan diabetes, a reduction of the blood glucose level was observed in seven out of ten animals and the reduction persisted for several hours and was ranging from 30 to 75% [43]. Singh et al have reported antidiabetic efficacy of Glibenclamide loaded liposomes in alloxan induced diabetic rats. Initially multi-lamellar liposomes were prepared by employing thin film hydration technique. A lipid phase was prepared by dissolving weighed quantity of drug accurately. The antihyperglycemic effects of various Glibenclamide loaded liposomes were evaluated on fasting blood glucose levels in diabetic rats at different time levels. The level of blood glucose started to decrease from 2nd hour when Glibenclamide solution (standard) was given and reaches to normal level in 4th and 8th hour but after that it started to rise again. In case of formulated Glibenclamide the level of blood glucose started to decrease from 6th hour and it was maintained up to 16th hour [44]. Dinesh et al have reported formulation characterization and in-vitro evaluation of acarbose loaded ultra-deformable liposome gel for effective transdermal drug delivery. Spherical discrete, free flowing ultra deformable liposomes were prepared. The acorbose loaded ultra-deformable formulations one, two and three showed a percentage drug entrapment of 33.33 ± 2.2 %, 42.6 ± 1.8 %, and 46.66 ± 1.2 % respectively. The percentage cumulative in vitro drug release for these formulations were found to be 70.62 ± 0.24 %,73.35 ± 0.28 %, 84.70 ± 0.92 % respectively [45].
Transfersomes
Transferosome are a form of elastic or deformable vesicle which was first introduced in the early 1990’s. Transferosomes possess good advantages as phospholipid drug vesicles for transdermal drug delivery. The driving force is nothing more than osmotic pressure; these liposomes are called transfersomes. Depending upon the choice of administration or application their self optimized and ultra flexible membrane properties are capable of delivering drugs reproducibly through the skin. The need to reach the narrow tubes that make up the skin (hair follicles and intercellular spaces between lipids) to deliver drugs, led to the invention of transfersomes. The original idea to use liposomes as drug delivery systems was very smart, as they are made of lipids similar to biological membranes, but they have rigid structure. The incorporation of elements in the lipid bilayer to make it flexible has made these carriers successful. Transferosomes deform and pass through narrow constriction (10 times smaller than their own diameter) without measurable loss. This deformation gives better penetration of intact vesicles. Traditional transformable liposomes are made using surfactants in the lipid bilayer. The use of flexible transferosomes is an invaluable strategy to reach the objective of drug delivery via the transdermal route. The use of these kinds of nanocarriers seems to be more effective than liposomes, and their flexibility allows the possibility of using them as transdermal vaccine vectors [46]. Malakar et al have evaluated, formulated and optimized the ability of transferosome gel for transdermal drug delivery. The effect of independent process variables like ratio of lipids (soya lecithin: cholesterol), ratio of lipids and surfactants, and ratio of surfactants (Tween 80: sodium deoxycholate) on the invitro permeation flux (lg/cm2/h) of formulated transferosomal gels containing insulin through porcine ear skin was optimized using 23 factorial design. The optimal permeation flux was achieved as 13.50 ± 0.22 lg/cm2/h with drug entrapment efficiency of 56.55 ±0.37 % and average vesicle diameter range was found to be 625-815 nm [47].
Ethosomes
Ethosomes are lipid vesicles containing phospholipids, alcohol (in relatively high concentrations) and water. Ethosomes, contain alcohol in the lipid bilayer to make them more flexible and be able to be deformed when more pressure is applied. These carriers allow drugs to reach deeper skin layers and thereby reach systemic circulation. Ethosomes are easy to prepare, and they are recognized as safe and efficient. For these reasons, they could have wide variety of future applications. Their main characteristics are malleability and softness because of this they are considered as good drug-delivery systems. Ethosomes are able to contain and deliver a lot of molecules because they can transport highly lipophilic drugs. Ethosomes can entrap drug molecule with various physicochemical properties and in the future these systems offer a huge opportunity to make better therapies, besides which they can transport molecules through the skin and biological membranes [48-50].
Niosomes
Niosomes are generally made up of lipids and non-ionic surfactants, which are biodegradable and minimally toxic. Niosomes (non-ionic surfactant vesicles) obtained on hydration are microscopic lamellar structures which forms a closed bilayer vesicle in aqueous media depending upon its amphiphilic nature utilizing some energy for physical agitation and instant heat to create this structure. Niosomes were created with the same goal as transferosomes and ethosomes in order to make liposomes less rigid and let these bilayer systems go where liposomes cannot go. In addition, the incorporation of non-ionic surfactants gives better stability to the liposomes. In the bilayer structure, hydrophobic parts are usually oriented away from the aqueous solvent, whereas the hydrophilic heads remain in close contact with the aqueous solvent.
The properties of the vesicles can be changed by varying the composition of the vesicles, size, lamellarity, tapped volume, surface charge and concentration. Various forces act inside the vesicle such as repulsive forces emerging from the electrostatic interactions among charged groups of surfactant molecules, vanderwaal forces among surfactant molecules, entropic repulsive forces of the head groups of surfactants, short-acting repulsive forces, etc. These forces play a key role in maintaining the vesicular structure of niosomes.
The niosomes were originally used in the cosmetics industry, and the versatility of these systems has allowed their use to spread to other areas. For example, in pharmaceutical products, they are formulated for drug delivery. They are used for many routes of administration: oral, parenteral, ocular, and vaginal, including transdermal. The application of niosomes in transdermal drug delivery has been very important, because they can carry anti-aging agents and antifungal molecules, among other drugs. Due to presence of hydrophilic, amphiphilic and lipophilic moieties in the structure, these can accommodate drug molecules with a wide range of solubility [51,52]. Pardakhty et al. have studied pharmacokinetic properties of niosomeloaded insulin in diabetic rats. They entrapped recombinant human insulin in multilamellar niosomes composed of polyoxyethylene alkyl ether surfactants (Brij 52 and Brij 92) or sorbitan monostearate (Span 60) and cholesterol. The amount of insulin released in simulated intestinal fluid (SIF) and simulated gastric fluid (SGF) were measured at 37 °C. The results obtained showed that animals treated with oral niosome-encapsulated insulin (100 IU/kg) showed decreased levels of blood glucose and elevated serum insulin, which in the case of Brij 92 niosomes, hypoglycemic effect was significant (P<0.05) [53].
Raja et al have reported formulation and evaluation of maltodextrin based proniosomal drug delivery system possessing antidiabetic glipizide drug. Glipizide loaded maltodextrin based proniosome were prepared (Figure 4) by slurry method with different surfactant to cholesterol ratio. The corresponding proniosome formulations were evaluated for entrapment efficiency. The results showed higher entrapment efficiency of 84.25 ± 1.25 and in-vitro release of 99.23% at the end of 24h [54].
Figure 4: Maltodextrin based proniosome loaded with antidiabetic drug Glipizide.
Azza et al have reported formulation and evaluation of metformin hydrochloride (MH)-loaded niosomes as controlled release drug delivery system. Reverse phase evapouration technique with slight modification was adopted for the preparation of MH-loaded niosomes by using span 40 and cholesterol (Figure 5). To obtain negative and positive charged vesicles diacetyl phosphate (DCP) and 1, 2-dioleoyl- 3-trimethylammonium propane chloride salt (DOTAP) was used. The mean particle size ranged from 223.5 to 384.6 nm and the MHloaded niosomes effectively sustain the release of drugs particularly with the positively charged niosomes. By measuring the serum values of glucose and metformin the bioavailability of MH- loaded niosomes were determined. Results showed that the MH-loaded niosomal preparation significantly prolonged the intensity of hypoglycemic effect more than that of free MH solution [55].
Figure 5: TEM image showing Metformin Hydrochloride loaded niosomes.
Dendrimers
Dendrimers are polymer-based macromolecules designed from monomeric or oligomeric units, such that each layer of branching units doubles or triples the number of peripheral groups. The void area within a dendrimer, the degree of its branching, its simplicity of modification and preparation, and size control offer great potential for drug delivery. The term “dendrimer†is Greek: “dendra†means tree and “meros†means part. This name was coined in the late 1970s by a research group formed by Vogtle, Denkewalter, Tomalia, and Newkome. Dendrimers are nonpeptidic fractal 3-D structures made of numerous small molecules. Modification of the degree of branching may allow for encapsulation of a molecule within this structure. For example, a dendrimer may become water-soluble when end-groups of dendrimers are functionalized with hydrophilic groups, such as carboxylic acids. Thus, water-soluble dendrimers may be designed with internal hydrophobicity, suitable for the encapsulation of a hydrophobic drug. The use of dendrimers to encapsulate hydrophobic and labile molecules has been a successful road. The permeability of dendrimers through the skin depends on physicochemical characteristics like generation size, molecular weight, surface charge, composition, and concentration [56-59] [Figure 6 and Figure 7] .
Figure 6: Rosiglitazone loaded gelatin nanoparticles.
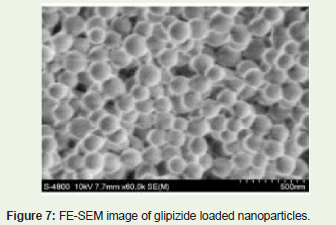
Figure 7: FE-SEM image of glipizide loaded nanoparticles.
Nanoparticles
The main property of drug delivery systems is to reach the organ of interest and often to go through it. The use of different carriers like those mentioned previously in this text, in addition to this nanoparticle also contributes significant role to accomplishing the core objective of drug delivery [60]. From the past few years, scientists have designed lots of nanocarriers for helping to improve transport of therapeutic drugs into the skin and through biological membranes. Skin is considered as an important route for various drug delivery systems, and moreover because of its larger contact area it can be very valuable to administer drugs both locally and systemically.[61-65] Nanotechnology in the pharmaceutical industry opens a new avenue of therapies for the treatment of many diseases and represents hope that people may be benefited to lead a better life. Nowadays, it is quite easier to encapsulate a wide variety of pharmacologically active molecules into nanoparticles like drugs, proteins, peptides, DNA, etc. To enable percutaneous delivery gold nanoparticles, has been used to encapsulate protein drugs to trigger, the interaction between the skin barrier and gold nanoparticles so that the increase in skin nanoparticles with 32 full factorial design emulsification solventevaporation technique was used. Initially the drug and the polymer were dissolved in dichloromethane/methanol mixed solvents. Inorder to reduce the particle size in nano scale high pressure homogenizer was used. Dissolution study of the selected formulation showed 209.6 nm size and 95.66 ± 1.70 percent encapsulation efficiency. From the in-vitro studies it was found that glipizide loaded nanoparticles showed a sustained release up to seven days (64.79 ± 2.68) and follows first order kinetics. The blood glucose level was decreased to 132.66 ± 9.83 mg/dL over seven days time interval. Finally it was concluded that sustained release of glipizide loaded nanoparticles could be able to manage type II diabetes with reduced dose frequency, minimal side effects and enhanced patient compliance [66].
Chander et al. have reported development and characterization of nanoparticles of Glibenclamide (GB) by solvent displacement method (Figure 8). GB enriched nanoparticles Drug: Polymer ratio was found to be an important factor in determining the size of the nanoparticles besides other factors but smallest particle size was observed at drug : polymer (1:1) which is mainly attributed to the amount of surfactant enough to maintain the stability of nanoparticles at an equimolar ratio of drug and polymer and moreover coalescence of droplets did not occur at this ratio. Further with the increase in drug concentration with respect to polymer the encapsulation efficiency as well as drug loading capacity was found to be increased. The formulated nanoparticles showed a significant change in saturation solubility in comparison to pure drug and decreased tmin with improved bioavailability. Over all the developed GB nanoparticles showed superior activity when compared to plain GB in alloxan induced diabetic model with reduced dose frequency, decreased side effects and improved patient compliance [67].
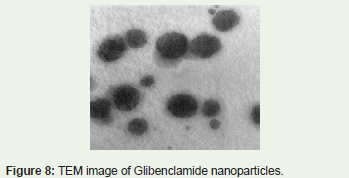
Figure 8: TEM image of Glibenclamide nanoparticles.
Nanoemulsions
Emulsions with droplet size in the nanometric scale (typically in the range 20-200 nm) are often referred in the literature as miniemulsions, nano-emulsions, ultrafine emulsions, submicron emulsions. Nanoemulsions are isotropic dispersed systems of two nonmiscible liquids, generally consisting of an oily system dispersed in an aqueous system, or an aqueous system dispersed in an oily system but forming droplets or other oily phases of nanometric sizes. Nanoemulsions are thermodynamically considered as unstable systems, in contrast to microemulsions, because nanoemulsions require high energy to generate them. Due to their small droplet size nano-emulsions possess extra stability against sedimentation or creaming with Ostwald ripening forming the main mechanism of nano-emulsion breakdown. The main application of nanoemulsions is the preparation of nanoparticles using a polymerizable monomer as the disperse phase where nano-emulsion droplets act as nanoreactors. Despite this, they can be stable for long periods due to their extremely small size and the use of adequate surfactants. Hydrophobic and hydrophilic drugs can be formulated in nanoemulsions because it is possible to make water/oil or oil/water nanoemulsions. They are nontoxic and non-irritant systems, and they can be used for skin or mucous membranes and parenteral and nonparenteral administration in general, and they have been utilized in the cosmetic field [68,69].
Nanoemulsions can be prepared by three methods mainly: highpressure homogenization, microfluidization and phase-inversion temperature. Transdermal delivery using nanoemulsions has decreased due to the stability problems inherent to this dosage form. Li et al have reported the efficacy of nano emulsions coated with alginate /chitosin act as effective oral insulin delivery systems. The relative pharmacological bioavailability of the coated nanoemulsion with 25 and 50 IU/kg insulin were found to be 8.42% and 5.72% in normal rats and 8.19% and 7.84% in diabetic rats respectively. Moreover, there were significant prolonged hypoglycaemic effects were observed after oral administration of the coated nanoemulsions compared with subcutaneous insulin. They finally concluded that, the nanoemulsion coated with alginate/chitosan was a potential delivery system for oral delivery of polypeptides and proteins [70]. Mohammed et al have reported investigation of nanoemulsion system for transdermal drug delivery of Glibenclamide (Figure 9). The nanoemulsion formulation mainly consists of labrafac and triacetin (1:1) as an internal oil phase in external aqueous phase. Tween 80 was used as surfactant and diethylglycol as a cosurfactant. The nanoemulsion formulation had small droplet size of nearly 117 nm, with uniform size distribution (PI < 0.247) and low viscosity (< 73.0 mP). From the results it concluded that size and region of nanoemulsion existence was strongly influenced by the presence of surfactant and cosurfactant. The nanoemulsion formulation in the form of dermal gel can be prepared effectively for both in vivo and ex vivo studies and a novel transdermal system for Glibenclamide could be introduced successfully.
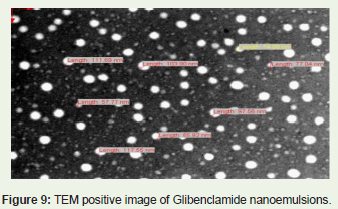
Figure 9: TEM positive image of Glibenclamide nanoemulsions.
Enkhzaya et al. have reported the formulation parameters influencing the physicochemical characteristics of rosiglitazoneloaded cationic lipid emulsion. By using cationic lipid DOTAP, DOPE, castor oil, tween 20, and tween 80 rosiglitazone loaded cationic lipid emulsions were prepared. They optimized various parameters in terms of droplet size on the effect of cationic lipid emulsion composition ratio on drug encapsulation efficiency, in-vitro drug release and cellular uptake of rosiglitazone loaded emulsion. The results showed that the rosiglitazone loaded cationic emulsion improves in-vitro drug release in comparison to rosiglitazone alone. The cellular uptake of rosiglitazone in insulin resistant HepG2 cells was more than the normal HepG2 cells. In conclusion these cationic lipid emulsions can be used as excellent drug delivery systems for rosiglitazone and could enhance its cellular uptake efficiency in target cells [71].
Solid-lipid-nanoparticles
Solid lipid nanoparticles (SLPs) are lipid-based submicron colloidal carriers. In the early 1990s SLNPs treated as a pharmaceuticalalternative to liposomes and emulsions. Presence of relatively rigid core comprising of hydrophobic lipids that are solid at room and body temperatures, surrounded by a monolayer of phospholipids makes them more stable than liposomes in biological systems. These aggregates are further stabilized by the inclusion of high levels of surfactants further stabilizes the aggregates of SLNPs. Because of theirease of biodegradation, they are less toxic when compared to polymer or ceramic nanoparticles. They have controllable pharmacokinetic parameters and can be engineered with three types of hydrophobic core designs: a homogenous matrix, a drug-enriched shell, or a drugenriched core. Two primary production methods exist for SLNPs which includes a high-pressure homogenization technique devised by Muller and Lucks and a microemulsion technique pioneered by Gasco. It has been confirmed that the compound payload exits the hydrophobic core at warmer temperatures conversely, the compound payload enters the hydrophobic core at cooler temperatures. These properties are used to load and unload SLNP’s for the delivery of therapeutic drugs, taking advantage of recent techniques to selectively produce hypo and hyperthermia.
Additionally, the quantity of surfactant used during the process of synthesis contributes to the release profile of the drug payload. SLNPs can be used to deliver drugs orally, topically, or via inhalation. Rakesh et al have reported the ability of SLNPs as a carrier for antidiabetic drug metformin for transdermal drug delivery. Metformin-SLNPs were prepared by solvent diffusion technique using propylene glycol (solvent), polymethacrylic acid (polymer) and soya lecithin (lipid base). After doing the evaluation of the above mentioned pharmaceutical parameters, Metformin-SLNP’S were loaded in Methocel K100M transdermal patches. Ex-vivo permeation studies indicate that the high cumulative amount of drug was permeated from Metformin-SLNPs [72-74] (Figure 10)(Figure 11).
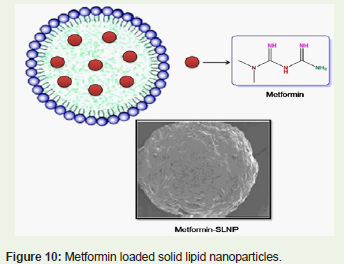
FIgure 10: Metformin loaded solid lipid nanoparticles.
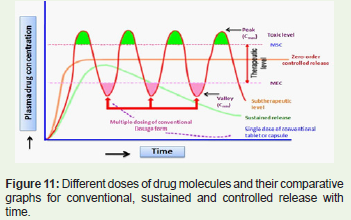
FIgure 11: Different doses of drug molecules and their comparative graphs for conventional, sustained and controlled release with time.
Cell penetration of nanodrug
There are several natural biological barriers to inhibit the body suffering from damage, such as blood brain barrier, blood-eye barrier, biomembrane barrier and so on, but the existence of given programmed time through the process of leaching, infiltration and proliferation or dissolution and act on the specific target organ, tissue and cell.
In addition to this, the nanocarriers prevent drug from degradation by various biological enzymes and extends the effective time period of drugs. At the same time at this controlled-release nanodrug can decrease the peak phenomenon of blood concentration, reduce toxic effects and improve overall efficacy.
Conclusion
The interdisciplinary multifunctional nature of nanotechnology and nanodrugs enabled diversification and advancements to improve the quality of life. Because nanodrug is a new type of drug, the development of nano-drug will cause the revolution of the diagnosis and treatment however at present, the basic theory of nanotechnology applied in medicine and the preparation of nanodrugs are not fully explored. Therefore extensive research has to be carried out in the field of nanotechnology applied in medicine has a great deal of work needs to be done, but the superior capability that nanodrugs owns indicates a very wide range of applications in the clinical treatment of various diseases. Transdermal drug delivery offers an attractive alternative to the conventional drug delivery methods of oral administration and injection. However at present the clinical use of transdermal drug delivery is limited by the fact that very few drugs can be delivered transdermally at a viable rate. This difficulty is mainly because the stratum corneum of the skin acts as efficient barrier that limits the penetration of drugs through the skin. Inorder to increase the rate of drugs available for transdermal drug delivery the use of nanocarriers became an excellent alternative source for delivering both lipophilic and hydrophilic drugs throughout the stratum corneum with the possibility having local or systemic effect for treating various diseases.
Acknowledgements
The authors sincerely thank the management of VIT University for providing all the necessary facilities for writing this review in paper form.
References
- Sahoo SK, Labhasetwar V (2003) Nanotech approaches to drug delivery and imaging. Drug discov Today 8: 1112-1120.
- Bhumkar DR, Joshi HM, Sastry M, Pokharkar VB (2007) Chitosan reduced gold nanoparticles as novel carriers for transmucosal delivery of insulin. Pharm Res 24:1415-1426.
- Kayser O, Lemke A, Hernandez-Trejo N (2005) The impact of nanobiotechnology on the development of new drug delivery systems. Curr Pharm Biotechnol 6: 3-5.
- Yih T, Al †Fandi M (2006) Engineered nanoparticles as precise drug delivery systems. J Cell Biochem 97: 1184-1190.
- Tao SL, Desai TA (2003) Microfabricated drug delivery systems: from particles to pores. Adv Drug Deliv Rev 55: 315-328.
- Parveen S, Misra S, Sahoo SK (2012) Nanoparticles: a boon to drug delivery, therapeutics, diagnostics and imaging. Nanomedicine 8: 147-166.
- Nel AE, Madler L, Velegol D, Xia T, Hoek EMV, et al. (1999) Understanding the biophysicochemical interactions at the nano bio-interface. Nature Materials 8: 543-557.
- Shephard MJ, Todd D, Adair BM, Po ALW, Mackie DP, et al. (2003) Immunogenicity of bovineparainfluenza type 3 virus proteins encapsulated in nanoparticle vaccines, following intranasal administration to mice. Res Vet Sci 74: 187-190.
- Cui ZR, Mumper RJ (2002) Intranasal administration of plasmid DNA-coated nanoparticles results in enhanced immune responses. J Pharm Pharmacol 54: 1195-1203.
- Vijayanathan V, Thomas T, Thomas TJ (2002) DNA nanoparticles and development of DNA delivery vehicles for gene therapy. Biochemistry 41: 14085-14094.
- Cleland JL (1998) Solvent evaporation processes for the production of controlled release biodegradable microsphere formulations for therapeutics and vaccines. Biotechnol Prog 14: 102-107.
- Aukunuru JV, Ayalasomayajula SP, Kompella UB (2003) Nanoparticle formulation enhances the delivery and activity of a vascular endothelial growth factor antisense oligonucleotide in human retinal pigment epithelial cells. J Pharm Pharmacol 55: 1199-1206.
- Wild S, Roglic G, Green A, Sicree R, King H (2004) Globalprevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 27: 1047-1053.
- DeFronzo RA (1988) Lilly Lecture 1987: The triumvirate: beta cell, muscle, liver. A collusion responsible for NIDDM. Diabetes 37: 667-687.
- Pratley RE, Weyer C (2001) The role of impaired early insulin secretion in the pathogenesis of Type II diabetes mellitus. Diabetologia 44: 929-945.
- Zimmet P, Alberti KG, Shaw J (2001) Global and societal implications of the diabetes epidemic. Nature 414: 782-787.
- Wild S, Roglic G, Green A, Sicree R, King H (2004) Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 27: 1047-1053.
- Butler AE, Janson J, Bonner-Weir S, Ritzel R, Rizza RA, et al. (2003) Beta-cell deï¬cit and increased beta-cell apoptosis in humans with type 2 diabetes. Diabetes 52: 102-110.
- Stumvoll M, Goldstein BJ, van Haeften TW (2005) Type 2 diabetes principles of pathogenesis and therapy. Lancet 365: 1333-1346.
- King H, Aubert RE, Herman WH (1998) Global burden of diabetes, 1995/2025: prevalence, numerical estimates, and projections. Diabetes Care 21: 1414-1431.
- Watanabe M, Yamaoka K, Yokotsuka M, Tango T (2003) Randomized controlled trial of a new dietary education program to prevent type 2 diabetes in a high-risk group of Japanese male workers. Diabetes Care 26: 3209-3214.
- Zafar A, Davies M, Azhar A, Khunti K (2010) Clinical inertia in management of T2DM. Prim Care Diabetes 4: 203-207.
- Martin CR (2006) Welcome to nanomedicine. Nanomedicine 1: 5-5.
- Park K (2007) Nanotechnology: what it can do for drug delivery. J Control Release 120: 1-3.
- Florence AT (2007) Pharmaceutical nanotechnology: more than size. Ten topics for research. Int J Pharm 339: 1-2.
- Forrest ML, Kwon GS (2008) Clinical developments in drug delivery nanotechnology. Adv Drug Deliv Rev 60: 861-862.
- Papakostas D, Rancan F, Sterry W, Blume-Peytavi U, Vogt A (2011) Nanoparticles in dermatology. Arch Dermatol Res 303: 533-550.
- Kristl J, Teskac K, Grabnar PA (2010) Current view on nanosized solid lipid carriers for drug delivery to the skin. J Biomed Nanotechnol 6: 529-542.
- Schroeter A, Engelbrecht T, Neubert RH, Goebel AS (2010) New nanosized technologies for dermal and transdermal drug delivery: a review. J Biomed Nanotechnol 6: 511-528.
- Neubert RH (2011) Potentials of new nanocarriers for dermal and transdermal drug delivery. Eur J Pharm Biopharm 77: 1-2.
- Desai P, Patlolla RR, Singh M (2010) Interaction of nanoparticles and cell-penetrating peptides with skin for transdermal drug delivery. Mol Membr Biol 27: 247-259.
- Chourasia R, Jain SK (2009) Drug targeting through pilosebaceous route. Curr Drug Targets 10: 950-967.
- Cho K, Wang X, Nie S, Shin DM (2008) Therapeutic nanoparticles for drug delivery in cancer. Clin Cancer Res 14: 1310-1316.
- Blynskaya E, Alekseev K, Alyautdin R (2012) Perspectives of the development of pharmaceutical nanotechnology. Russ J Gen Chem 82: 519-526.
- Panariti A, Miserocchi G, Rivolta I (2012) The effect of nanoparticle uptake on cellular behavior: disrupting or enabling functions?. Nanotechnol Sci Appl 2012: 87-100.
- Pailler-Mattei C, Bec S, Zahouani H (2008) In vivo measurements of the elastic mechanical properties of human skin by indentation tests. Med Eng Phys 30: 599-606.
- Pailler-Mattei C, Bec S, Zahouani H (2008) In vivo measurements of the elastic mechanical properties of human skin by indentation tests. Med Eng Phys 30: 599-606.
- Diaz-Torres R. Transdermal nanocarriers (2010) In: Escobar-Chávez JJ, Merino V, editors. Current Technologies to Increase the Transdermal Delivery of Drugs. Bussum: Bentham Science 120-140.
- Grice JE, Ciotti S, Weiner N, Lockwood P, Cross SE, et al. (2010) Relative uptake of minoxidil into appendages and stratum corneum and permeation through human skin in vitro. J Pharm Sci 99: 712-718.
- Bakowsky H, Richter T, Kneuer C, Hoekstra D, Rothe U, et al. (2008) Adhesion characteristics and stability assessment of lectin-modified liposomes for site-specific drug delivery. Biochim Biophys Acta 1778: 242-249.
- Zaborova OV, Sybachin A, Ballauff M, Yaroslavov A (2011) Structure and properties of complexes of polycationic brushes with anionic liposomes. Polym Sci Ser A Chem Phys 53: 1019-1025.
- Touitou E, Junginger H, Weiner N, Nagai T, Mezei M (1994) Liposomes as carriers for topical and transdermal delivery. J Pharm Sci 83: 1189-1203.
- Hashmoto, Kawada J (1979) Effects of Oral Administration of Positively Charged Insulin Liposomes on Alloxan Diabetic Rats: Preliminary Study. Endocrinol Jpn 26: 337-344.
- Singh M, Balamurugan M, Gupta A, Yadav S, Sharma A, et al. (2007) Antidiabetic activity of Glibenclamide loaded liposomes in Alloxan induced diabetic rats. Ars Pharm 48: 31-36.
- Dinesh kumar V, Surya prakash TNK, Easwari TS (2010) Formulation characterization and in vitro evaluation of acarbose loaded ultra-deformable liposome gel for effective transdermal drug delivery. Adv Pharmacol Toxicol 11: 43-46.
- Patel R, Singh SK, Singh S, Sheth N, Gendle R (2009) Development and characterization of curcumin loaded transfersome for transdermal delivery. J Pharm Sci Res 1: 71-80.
- Malakar J, Suma OS, Amit KN, Kalyan KS (2012) Formulation, optimization and evaluation of transferosomal gel for transdermal insulin delivery. Saudi Pharmaceutical Journal 20: 355-363.
- Madsen JT, Vogel S, Karlberg AT, Simonsson C, Johansen JD, et al. (2010) Ethosome formulations of known contact allergens can increase their sensitizing capacity. Acta Derm Venereol 90: 374-378.
- Pannala S, Sri Samala U (2012) Ethosomes, a novel transdermal drug delivery systems: a review. J Pharm Res 4: 4628-4630.
- Lu WB, Chang GH, Luo YL, Liao F, Sun XP (2011) Method for effective immobilization of Ag nanoparticles/graphene oxide composites on single-stranded DNA modified gold electrode for enzymeless H2O2 detection. J Mater Sci 46: 5260-5266.
- Keservani RK, Sharma AK, Ramteke S (2010) Novel vesicular approach for topical delivery of baclofen via niosomes. Lat Am J Pharm 29: 1364-1370.
- Kumar GP, Rao PR (2012) Ultra deformable niosomes for improved transdermal drug delivery: the future scenario. Asian J Pharm Sci7: 96-109.
- Pardakhty A, Moazeni E, Varshosaz J, Hajhashemi V, Rouholamini NA (2011) Pharmacokinetic study of niosome-loaded insulin in diabetic rats. Daru 19: 404-411.
- Raja K, Jestin PU, Athul PV, Tamizharasi S, Sivakumar T (2011) Formulation and evaluation of maltodextrin based proniosomal drug delivery system containing anti-diabetic (Glipizide) drug. International Journal of PharmTech Research 3: 471-477.
- Hasan AA, Madkor H, Wageh S (2013) Formulation and evaluation of metformin hydrochloride-loaded niosomes as controlled release drug delivery system. Drug Deliv 20: 120-126.
- Astruc D, Boisselier E, Ornelas C (2010) Dendrimers designed for functions: from physical, photophysical, and supramolecular properties to applications in sensing, catalysis, molecular electronics, photonics, and nanomedicine. Chem Rev 110: 1857-1959.
- Esfand R, Tomalia DA (2001) Poly (amidoamine) (PAMAM) dendrimers: from biomimicry to drug delivery and biomedical applications. Drug Discovery Today 6: 427-436.
- Uchegbu I, Dufes CM, Kan PL, Schatzlein A (2008) Polymers and dendrimers for gene delivery in gene therapy. In: Templeton NS, editor. Gene and Cell Therapy: Therapeutic Mechanisms and Strategies, 3rd ed. Boca Raton: CRC Press.
- Svenson S (2009) Dendrimers as versatile platform in drug delivery applications. Eur J Pharm Biopharm 71: 445-462.
- Diaz-Torres R (2010) Transdermal nanocarriers. In: Escobar-Chavez JJ, Merino V, editors. Current Technologies to Increase the Transdermal Delivery of Drugs. Bussum: Bentham Science 120-140.
- Huang Y, Yu F, Park YS, Wang J, Shin MC, et al (2010) Co-administration of protein drugs with gold nanoparticles to enable percutaneous delivery. Biomaterials 31: 9086-9091.
- Mihranyan A, Ferraz N, Strømme M (2012) Current status and future prospects of nanotechnology in cosmetics. Prog Mater Sci 57: 875-910.
- Prow TW, Grice JE, Lin LL, Faye R, Butler M, et al (2011) Nanoparticles and microparticles for skin drug delivery. Adv Drug Deliv Rev 63: 470-491.
- Mohanraj V, Chen Y (2007) Nanoparticles - a review. Trop J Pharm Res 5: 561-573.
- Vandana S, Amrendra K (2010) Development and characterization of rosiglitazone loaded gelatin nanoparticles using two step desolvation method. International journal of pharmaceutical sciences review and research 5: 100-103.
- Amolkumar L, Satyendra M, Ravindra K, Jitendra N (2013) Formulation and evaluation of glipizide. International journal of pharmacy and pharmaceutical sciences 5: 147-151.
- Dora CP, Singh SK, Kumar S, Datusalia AK, Deep A (2010) Development and characterization of nanoparticles of Glibenclamide by solvent displacement method. Acta Pol Pharm 67: 283-290.
- Shakeel F, Ramadan W (2010) Transdermal delivery of anticancer drug caffeine from water-in-oil nanoemulsions. Colloids Surf B Biointerfaces 75: 356-362.
- Sonneville-Aubrun O, Simonnet JT, L’Alloret F (2004) Nanoemulsions: a new vehicle for skincare products. Adv Colloid Interface Sci 108-109:145-149.
- Li X, Qi J, Xie Y, Zhang X, Hu S, et al. (2013) Nanoemulsions coated with alginate/chitosan as oral insulin delivery systems: preparation, characterization and hypoglycaemic effect in rats. Int J Nanomedicine 8: 23-32.
- Enkhzaya D, Jeong-Sook P (2012) Formulation parameters influencing the physicochemical characteristics of rosiglitazone-loaded cationic lipid emulsion. Arch Pharm Res 35: 1205-1213.
- Rakesh KS, Navneet S, Sudha R, Shivkumar HG (2013) Solid lipid nanoparticles as a carrier of metformin for transdermal delivery. International Journal of Drug Delivery 5: 137-145.
- Ding JC, Hu FQ, Yuan H (2004) Uptake of mono-stearin solid lipid nanoparticles by A549 cells. Acta Phamaceutica Sinica 39: 876-880.
- Becker ML, Fagan JA, Gallant ND, Bauer BJ, et al. (2007) Length-dependent up take of DNA-wrapped single-walled carbon nanotubes. Adv Mater 19: 939-945.