Case Report
Acinetobacter Secondary Infection on Herpes Stromal Keratitis
Arjun Srirampur1* and Somasheila Murthy2
1Consultant, LV Prasad Eye Institute, KVC campus, Vijayawada, India
2Head of the Department, Cornea Services, LV Prasad Eye Institute, KVC campus, Vijayawada, India
Corresponding author:Arjun Srirampur, Consultant, LV Prasad Eye Institute, KVC campus, Vijayawada, India,Tel: +91-9989229832; E-mail: sarjuneye@gmail.com
Citation: Srirampur A, Murthy S. Acinetobacter Secondary Infection on Herpes Stromal Keratitis. Indian J Ocular Biol. 2017;2(1): 103.
Copyright © Srirampur A, 2017 This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Submission: 14/06/2017; Accepted: 23/06/2017; Published: 04/07/2017
Abstract
Aim: To report 2 cases of HSV stromal keratitis with Acinetobacter secondary bacterial infection.
Methods: Retrospective analysis of microbial keratitis from year 2009-2013.
Results: 2 cases of HSV stromal keratitis with culture proven Acinetobacter species did not resolve with sensitive antibacterial therapy instead responded to antiviral therapy.
Conclusion: Acinetobacter secondary infection is quite common in compromised corneas like herpes stromal keratitis.
Keywords: Acinetobacter; Herpes stromal virus; Keratitis
Introduction
Acinetobacter is a low virulent bacterium that is usually found in nosocomial infection of immune compromised patients in the intensive care units. It rarely causes microbial keratitis. Communityacquired keratitis with corneal perforation resulting from Acinetobacter has been reported [1,2]. Infections associated with corneal exposure, soft contact lens wear penetrating keratoplasty and chronic lymphatic leukemia have been reported in the literature [3-7]. Herpes simplex viral stromal kertatitis can present with stromal edema, epithelial defect and secondary infection with bacteria or fungus. We present two cases of culture proven Acinetobacter infection treated with sensitive antibacterial drugs with no response. Instead when antivirals along with topical steroids were started the lesions responded dramatically.
Material and Methods
Case 1
A 50 year old man presented with pain, redness, dimunition of vision in his left eye since 2 months. He had no history of trauma, foreign body fall into the eye. He was treated elsewhere with antifungal (Natamycin eye drops hourly), antibacterial (Moxifloxacin 0.5% eye drops hourly) and cycloplegic (atropine eye drops 2 times) in a day for 2 month with no response. At presentation he presented with visual acuity of 20/25 in right eye, hand movements in left eye. Anterior & posterior segment were normal in right eye. His left eye showed diffuse conjunctival congestion, central corneal epithelial defect (1.2 x 4.2 mm) with anterior to midstromal infiltrate (1x 2 mm) with surrounding stromal edema, scarring all around (Figure 1). Anterior chamber showed flare, cells and trace hypopyon. Posterior segment was within normal limits. Corneal scraping was done for bacteria and fungus which yielded no organisms. IFA, PCR for HSV 1 was also negative. Confocal microscopy also was inconclusive. Patient was started on fortified cefazolin and ciprofloxacin eye drops hourly with atropine eye drops 3 times day for 4 days. After 4 days there was no response and a repeat corneal scraping was done which showed gram negative coccobacilli, identified as Acinetobacter on culture. It was sensitive to most of the antibiotics except cefuroxime and chloramphenicol. Two weeks on intensive antibiotics did not yield any response. Patient was seen regularly for three months with no response. His visual acuity was the same and also the clinical picture. After three months the diagnosis was revised, as he had chronic presentation, stromal edema, scarring all around with few deep vascularizations, herpes simplex virus stromal keratitis was suspected and he was started on Acyclovir eye ointment 5 times a day and Prednisolone acetate eye drops 8 times a day. He was seen after one week with a dramatic improvement. His visual acuity improved to 20/150 with resolution of infiltrate, stromal edema. Later he was continued on tapering dose of Prednisolone acetate eye drops with Acyclovir eye ointment for 1 week more. After one month he had a best corrected visual acuity of 20/60 with complete resolution of infiltrate, stromal edema with some amount of stromal scarring (Figure 2).
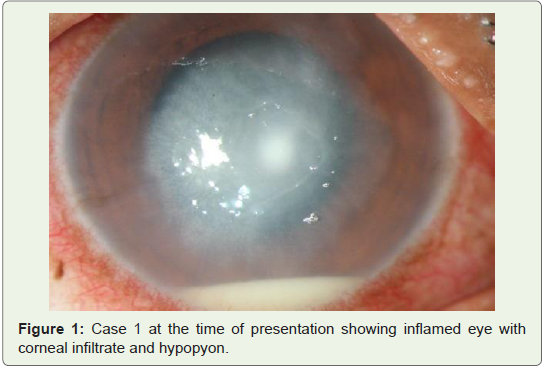
Figure 1: Case 1 at the time of presentation showing inflamed eye with corneal infiltrate and hypopyon.
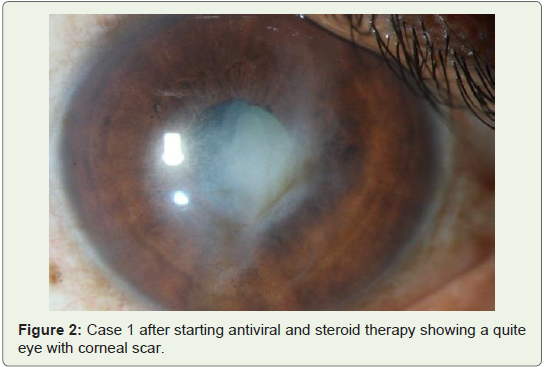
Figure 2: Case 1 after starting antiviral and steroid therapy showing a quite eye with corneal scar.
Case 2
The second case also presented with similar clinical history andfindings which responded with antiviral and steroid therapy insteadof antibacterial therapy (Figures 3 and 4).

Figure 3: Case 2 showing inflamed eye with central corneal ulcer.
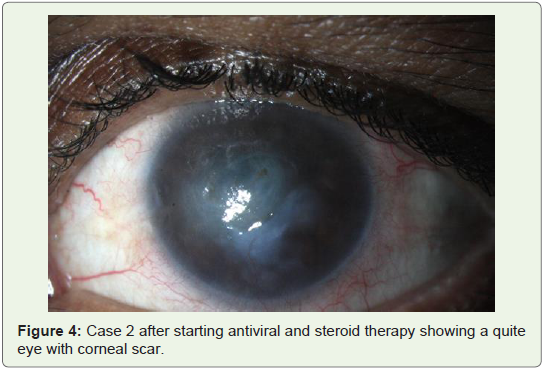
Figure 4: Case 2 after starting antiviral and steroid therapy showing a quite eye with corneal scar.
Discussion
Acinetobacter is ubiquitous, aerobic, gram-negative coccobacilli. It is known by various names such as Bacterium, Herellea, Mima, Achromobacter, Alcaligenes, Neisseria, Micrococcus, Diplococcus, B5W and Cytophaga [8,9]. It is a human commensal of relatively low virulence present on skin, mucus membranes, and the eyelid margin and in the urinary tract [10]. Patients with impaired host defenses or those in the intensive care unit setting are most frequently colonized. Among the Acinetobacter organisms, A. baumannii is the main species associated with nosocomial outbreaks. Pneumonia is the most common infection, whereas septicemia, endocarditic, urinary tract infections, meningitis and skin and soft tissue wound infections have also been reported.
Here we describe two cases which had colonization of Acinetobacter species on active herpes stromal keratitis. Mere microbiological positivity for Acinetobacter should not misguide the treating ophthalmologist to treat the bacteria rather should be aware that these bacteria colonizes the eye and does not cause fulminant infection.
Conclusion
Acinetobacter is a normal human commensal of relatively low virulence which colonizes rather than infects. The two patients presented in this study focus the attention of the ophthalmologist on yet another cause of opportunistic eye infection. Herpes stromal keratitis can be an important factor for subsequent contamination with Acinetobacter species.
References
- Wand M, Olive GM, Mangiaracine AB (1975) Corneal perforation and irisprolapse due to Mima polymorpha. Arch Ophthalmol 93: 239-241.
- Prashanth K, Ranga MP, Rao VA, Kanungo R (2000) Corneal perforation due to Acinetobacter junii: A case report. Diagn Microbiol Infect Dis 37: 215-217.
- Marcovich A, Levartovsky S (1994) Acinetobacter exposure keratitis. Br J Ophthalmol 78: 489-490.
- Herbst RW (1972) Herellea corneal ulcer associated with the use of soft contact lenses. Br J Ophthalmol 56: 848-850.
- Kent HD, Cohen EJ, Laibson PR, Arentsen JJ (1990) Microbial keratitis and corneal ulceration associated with therapeutic soft contact lenses. CLAO J 16: 49-52..
- Zabel RW, Winegarden T, Holland EJ, Doughman DJ (1989) Acinetobacter corneal ulcer after penetrating keratoplasty. Am J Ophthalmol 107: 677-678.
- Presley GD, Hale LM (1968) Corneal ulcer due to Bacterium anitratum. Am J Ophthalmol 65: 571-572.
- Glew RH, Moellering RC, Kunz LJ (1977) Infections with Acinetobacter calcoaceticus (Herellea vaginicola): Clinical and laboratory studies. Medicine 56: 79-97.
- Juni E (1984) Genus III. Acinetobacterer. Williams & Wilkins, Baltimore, Volume 1: pp. 303-307.
- Rosenthal SL (1974) Sources of Pseudomonas and Acinetobacter species found in human culture materials. Am J Clin Pathol 62: 807-811.