Case Report
The Eyes see only what the Mind Knows: A Rare Case Report of Scedosporium Apiospermum Brain Abscesses Following Near-Drowning in a Biogas Tank
Gavade G, Gosawi S, Vaswani R and Antony S*
Department of Pediatrics, Seth G.S and K.E.M Hospital, Mumbai, India
*Corresponding author:Sonu Antony, Department of Pediatrics, Seth G.S and K.E.M Hospital, Mumbai, India. E-mail Id: sonuantony94@gmail.com
Article Information:Submission: 06/06/2026; Accepted: 27/06/2026; Published: 30/06/2026
Copyright: ©2026 Gavade G, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Scedosporium apiospermum is an emerging opportunistic mold that causes invasive infections, particularly central nervous system (CNS) involvement with multiple brain abscesses in near-drowning victims exposed to contaminated water. We describe a 20-month-old immunocompetent boy from rural Maharashtra, India, who developed multiple brain abscesses following accidental near-drowning in a household biogas tank. He presented with aspiration pneumonitis, acute respiratory distress syndrome, refractory seizures, and left hemiparesis. Initial broad-spectrum antibiotics (ceftriaxone, metronidazole, vancomycin, meropenem) failed to resolve lesions on serial neuroimaging. High clinical suspicion, informed by literature on scedosporiosis in polluted-water near-drowning and biogas-related accidents, prompted empirical addition of oral voriconazole. Pus from surgical drainage of a parieto-occipital abscess revealed septate hyphae on calcofluor staining, with culture confirming S. apiospermum. Antifungal susceptibility testing showed low MICs to voriconazole (0.125 μg/mL), posaconazole, and itraconazole. Combination therapy with voriconazole and terbinafine, alongside surgical drainage, led to defervescence, seizure freedom, and gradual neurological recovery over four weeks. This case highlights the critical role of literature-guided suspicion for Scedosporium in atypical CNS infections refractory to antibacterials, especially in settings with household biogas exposure. Early voriconazole initiation and surgical intervention are essential for improved outcomes in this high-mortality infection.
Keywords:Scedosporiosis; Invasive Fungal Diseases; Tropical Infections; CNS Infections
Introduction
Scedosporium apiospermum and its teleomorph (sexual form)
Pseudallescheria boydii are soil saprophytes that thrive in polluted
waters and sewage [1]. These fungal pathogens, although generally
harmless, are known to cause highly invasive infections and have
emerged as the most common fungal infection in immunocompetent
near-drowning victims [2]. Scedosporiosis often manifests as
disseminated mycotic infections with frequent spread to the central
nervous system (CNS), resulting in multiple brain abscesses and
high mortality in near-drowning victims [3]. Biogas, as a renewable
energy source, has been traditionally used in Asia for over a century.
Harnessing biogas at the household level through anaerobic digestion
to convert organic animal waste, especially cow dung, into clean
cooking fuel is a widespread practice, particularly in rural India
[4]. Although underreported, accidents involving biogas plants
are common in Asia [5]. Pulmonary scedosporiosis following
biogas inhalation after falling into manure pits has previously been
reported in the literature [6]. We report a case of a 20-month-old
boy who developed multiple brain abscesses after near-drowning in a
household biogas tank.
Case Details
Our patient was a 20-month-old boy born of a third-degree
consanguineous union. He was hitherto developmentally normal,
with an uneventful perinatal history, and hailed from Baramati
district in Maharashtra, India. One month prior to presentation
at our center, he had an alleged history of accidental fall into a
household biogas plant. He was immediately rescued, found to be
unresponsive with no respiratory efforts, and received mouth-tomouth
breathing by his parents before being taken to a local hospital,
where he was resuscitated. He was diagnosed with aspiration
pneumonitis post-near-drowning, secondary to inhalation of toxic
chemicals and biogas, complicated by acute respiratory distress
syndrome (ARDS) with subcutaneous emphysema. He required
mechanical ventilation initially but was weaned and extubated by
day four of admission. He received intravenous (IV) ceftriaxone
and metronidazole. On day ten of admission, he developed multiple
episodes of paroxysmal events consisting of left-sided neck version
accompanied by tonic-clonic movements of the left upper and
lower limbs with secondary generalization. Seizures were controlled
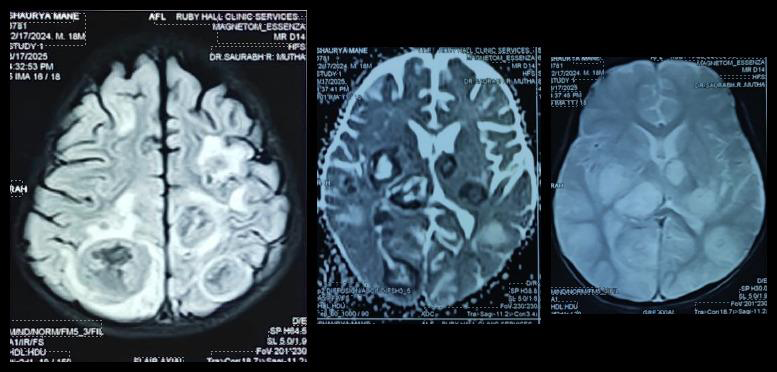
with levetiracetam and phenytoin. Magnetic resonance imaging
(MRI) of the brain showed multiple scattered round lesions (largest
measuring 3 × 2.6 cm) in the bilateral frontal, parietal, temporal, and
occipital white matter, bilateral thalami, ganglio-capsular region,
and cerebellum, with areas of diffusion restriction and tiny areas of
blooming on gradient echo (GRE) sequences, suggestive of multiple
brain abscesses [Figure 1]. This was on Day 11 after the aspiration.
Cerebrospinal fluid (CSF) analysis revealed 300 white blood cells with
lymphocytic predominance (76% lymphocytes), normal CSF sugar
(68 mg/dL; random blood sugar 79 mg/dL), and protein (24 mg/dL).
Aerobic, anaerobic, and fungal cultures of blood and CSF showed
no growth. Xpert MTB/RIF assay (Cepheid, Sunnyvale, California,
USA) for tuberculosis was negative. Antibiotics were upgraded to IV
vancomycin (60 mg/kg/day) and meropenem (40 mg/kg/day). After
21 days of IV therapy with these antibiotics, repeat neuroimaging
showed persistence of the lesions with interval increase in the size of
the largest lesion to 3 × 3 cm. He was therefore referred to our tertiary
care center for further management.
At presentation to our center, his vital parameters were normal.
Anthropometric assessment showed weight 8.6 kg (−2SD to −3SD),
length 79 cm (−2SD to −3SD), and head circumference 45.5 cm
(−2SD to −3SD) according to World Health Organization (WHO)
growth charts. On neurological examination, the child was awake but
irritable, with no cranial nerve deficits. He had left-sided hemiparesis,
with spasticity, exaggerated deep tendon reflexes, and non-sustained
clonus in the left upper and lower limbs. No features suggestive of
raised intracranial pressure were noted. Developmental assessment
revealed regression of motor and speech milestones. Fundus
examination was normal with no papilledema. Examination of other
systems was unremarkable. Preliminary investigations showed a
normal complete blood count (hemoglobin 9.8 g/dL, white blood
cell count 9.8 × 10³/mm³, platelet count 5.41 × 10⁵/mm³). C-reactive
protein (CRP) was 78 mg/L and erythrocyte sedimentation rate (ESR)
was 48 mm/hour. His 2D ECHO was normal and showed no evidence
of any vegetations. Repeat neuroimaging showed persistence of the
lesions with leptomeningeal enhancement in the bilateral parieto-
occipital lobes. After a thorough literature search for similar case
reports, scedosporiosis was considered in the differential diagnosis.
On clinical suspicion, voriconazole (9 mg/kg orally twice daily) was
added.
The patient underwent aspiration and drainage of the right
parieto-occipital abscess. Fluorescent microscopy and calcofluor
staining of the pus revealed septate fungal filaments. Fungal culture
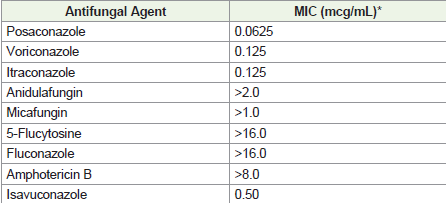
confirmed growth of Scedosporium apiospermum. Antifungal
susceptibility testing (broth microdilution per CLSI M38-A2
guidelines for filamentous fungi [7] showed low minimum
inhibitory concentrations (MICs) to posaconazole (0.0625 μg/
mL), voriconazole (0.125 μg/mL), and itraconazole (0.125 μg/mL),
with higher MICs to isavuconazole (0.5 μg/mL), amphotericin B
(>8.0 μg/mL), echinocandins, and other agents (Table 1). Guided
by the susceptibility profile, oral voriconazole was continued with
monitoring for therapeutic levels and hepatotoxicity. Antibiotics
were discontinued, and oral terbinafine was added in view of the
severe disease. After surgical drainage and four weeks of combination
therapy, the patient remained afebrile, seizure-free, and showed
significant clinical improvement, including increased interaction and
gradual recovery of lost milestones. At discharge, he was advised to
continue prolonged oral therapy with voriconazole and terbinafine,
with vigilant clinical and radiological follow-up, and was referred for
neuro-rehabilitation to address persisting neurological deficits and
sequelae.
Discussion
Scedosporium species are ubiquitous saprophytes and remain
a rare cause of invasive fungal disease (IFD) in immunocompetent
hosts. However, due to limited therapeutic options and high
mortality, it has been categorized as a medium-priority pathogen in
the recent World Health Organization Fungal Priority Pathogen List
(WHO FPPL) [8]. It is important to note that frequent taxonomy and
nomenclature changes over the last decade can make the literature
on this pathogen confusing for practicing clinicians. In the past
decade, numerous case reports of scedosporiosis have been described
in near-drowning victims in polluted waters and, interestingly, in
post-tsunami survivors. It is interesting to note, that such cases have
been reported in immunocompetent individuals as well. [2,3,8].
On microscopy, these organisms may resemble Aspergillus, so
definitive diagnosis relies on culture from infected tissue or sterile
body fluids. Species-level identification is increasingly performed
using matrix-assisted laser desorption/ionization time-of-flight mass
spectrometry (MALDI-TOF MS) and polymerase chain reaction
(PCR)-based sequencing of the internal transcribed spacer (ITS)
region and β-tubulin gene [8]. Species-level differentiation is critical,
as treatment response varies between the Scedosporium apiospermum
complex and closely related species such as Lomentospora prolificans
[8]. According to the latest European Confederation of Medical
Mycology (ECMM) guidelines [9], voriconazole remains the firstline
drug of choice for all forms of scedosporiosis. Monotherapy with
amphotericin B is discouraged due to high rates of in vitro resistance
and poor clinical efficacy. There is only marginal evidence for the
efficacy of posaconazole, itraconazole, and isavuconazole, which
have been used in select cases when voriconazole is unavailable or
contraindicated [8]. Voriconazole-based combination therapy with
terbinafine has been employed in refractory cases, although robust
evidence is lacking [8,9]. The optimal duration of treatment remains
controversial and should be individualized based on site, severity,
response, and immune status. Reported durations of voriconazole
therapy in the literature range from several months to even years
[10]. Novel antifungal agents such as olorofim and fosmanogepix
are in late-stage clinical trials and may expand treatment options for
scedosporiosis in the near future [11].
This case highlights several important clinical lessons. A
thorough literature search is an indispensable tool for clinicians. It
enabled us to recognize that scedosporiosis is a common pathogen
causing brain abscesses in survivors of near-drowning in polluted
waters, especially in Asian countries. This was crucial, as it prompted
empirical addition of voriconazole based on high clinical suspicion
even before microbiological confirmation. It also underscores the
need for pediatricians and intensivists to maintain a high index of
suspicion for atypical organisms when brain abscesses are refractory
to conventional antibiotic therapy. In complicated and atypical
CNS infections, early surgical drainage is often helpful for precise
microbiological diagnosis, optimization of antimicrobial strategy,
and reduction in therapy duration. Conventional wisdom often
favors liposomal amphotericin B or echinocandins for invasive fungal
diseases (IFDs); however, rare mold infections such as scedosporiosis
respond poorly to both agents. Therefore, clinicians and intensivists
must stay updated on existing treatment guidelines or seek expert
opinion from infectious disease (ID) specialists when feasible.
Conclusion
Delayed recognition of Scedosporium Apiospermum in postnear-
drowning CNS infections can lead to mortality and prolonged
morbidity. This case illustrates how literature-guided suspicion can
avert such delays. Early voriconazole initiation and surgical drainage
is critical. Heightened awareness of household biogas-related
accidents and polluted-water exposure is essential to improve timely
diagnosis and outcomes in pediatric scedosporiosis.
Declaration of patient consent:
Appropriate patient consent was obtained.References
Citation
Gavade G, Gosawi S, Vaswani R, Antony S. The Eyes see only what the Mind Knows: A Rare Case Report of Scedosporium Apiospermum Brain Abscesses Following Near-Drowning in a Biogas Tank. Indian J Neurol. 2026;7(1): 171.