Case Series
A Case Series of Monogenic Strokes in A Tertiary Care Centre
Bilia KA*, Nagendra S, Ojha P, Jagiasi K, Mahto A, Chaudhary G, Goud SK, Bagadia HP and Maniyar A
Department of Neurology, Grant Medical College and JJ Hospital, Mumbai, India
*Corresponding author:Bilia K. Aipu, Department of Neurology, Grant Medical College and JJ Hospital, Mumbai, India. E-mail Id: biliamary92@gmail.com
Article Information:Submission: 12/05/2026; Accepted: 02/06/2026; Published: 05/06/2026
Copyright: © 2026 Bilia KA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Monogenic strokes are a rare but significant cause of stroke in young individuals and often present with distinct clinical and radiographic features. This case series describes three young patients with stroke caused by different monogenic disorders: CADASIL (NOTCH3 mutation), Werner syndrome (WRN gene mutation), and congenital contractural arachnodactyly (FBN2 mutation). Each case highlights unique clinical and imaging characteristics, emphasizing the importance of genetic testing in young stroke patients, particularly in the absence of traditional vascular risk factors. Early recognition and diagnosis of monogenic strokes can guide appropriate management and genetic counseling, underscoring the need for increased awareness and consideration of genetic causes in young stroke patients.
Keywords:Monogenic Stroke; Cerebral Small Vessel Disease; Genetics
Introduction
Stroke is one of the leading causes of death and long-term
disability worldwide. The pathogenesis of stroke is multifactorial.
Cerebral small vessel disease (CSVD) refers to a syndrome of
clinical, neuroimaging, and neuropathological findings arising
from pathological processes affecting cerebral perforating arteries,
arterioles, capillaries, and venules [1]. The underlying etiology varies,
and some causes are genetic in origin.
Monogenic small vessel diseases are responsible for approximately 1-5% of strokes, particularly among young individuals [2]. “Monogenic stroke” refers to stroke caused by a rare single-gene mutation or disorder. These disorders may present with transient ischemic attacks, lacunar infarcts, cognitive decline, psychiatric manifestations, and dementia. The identification of genes implicated in such disorders has enhanced understanding of disease mechanisms and facilitated the development of disease models.
In this case series, we describe the clinical presentations, imaging findings, and genetic basis of three young patients with monogenic stroke.
Monogenic small vessel diseases are responsible for approximately 1-5% of strokes, particularly among young individuals [2]. “Monogenic stroke” refers to stroke caused by a rare single-gene mutation or disorder. These disorders may present with transient ischemic attacks, lacunar infarcts, cognitive decline, psychiatric manifestations, and dementia. The identification of genes implicated in such disorders has enhanced understanding of disease mechanisms and facilitated the development of disease models.
In this case series, we describe the clinical presentations, imaging findings, and genetic basis of three young patients with monogenic stroke.
Case 1:
A 40-year-old male presented with progressive cognitive decline,
behavioral changes and spastic paraparesis for one year. He had a past
history of migraine and a positive family history of similar complaints
in his father.On examination his BP was 140/90 mmHg. Neurological examination revealed bilateral pyramidal signs and executive dysfunction. His routine blood investigations (CBC, RFT, LFT, ESR, CRP) and autoimmune panel (ANA, APLA) were within normal limits. His MRI brain [Figure 1] showed T2 FLAIR hyper intense lesions involving external capsule and periventricular leucomalacia with hypertensive microangiopathy.MR Brain angiogram was normal.
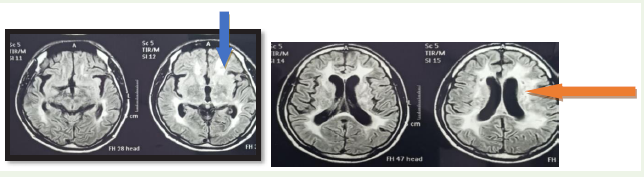
Considering the positive family history, history of migraine and
characteristic MRI findings genetic analysis was performed which
revealed NOTCH 3 mutation consistent with CADASIL.
Case 2:
A 37 year old male with hypertension for three years presented
with recurrent stroke episodes. The first episode consisted of sudden
onset left sided weakness that resolved within a few hours, followed
four months later by dysarthria.He also had a history of cataract
requiring surgery. His father had a history of young onset left
hemiparesis.On clinical examination his blood pressure was elevated (180/100mmHg). Neurological examination showed left UMN facial nerve palsy, bilateral pyramidal signs and extensor plantar responses. Routine laboratory investigations including autoimmune workup (ANA, ANA blot, APLA) were within normal limits. Two dimensional ECHO showed evidence of hypertensive heart disease. USG abdomen with renal Doppler study was normal.
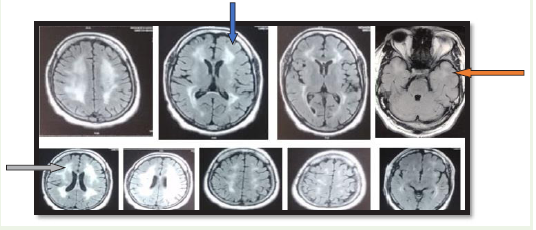
MRI brain [Figure 2] revealed T2/ FLAIR hyper intense white matter lesions involving the periventricular, external capsule and anterior temporal pole. His MR brain angiogram was normal.
In view of young age, positive family history and characteristic MRI findings clinical exome sequencing was performed and revealed WRN gene mutation suggestive of Werner syndrome.
Case 3:
A 19 year old boy presented with six episodes of transient left sided
weakness over one month, with each episode lasting approximately
30 minutes and complete recovery afterward. There was no significant
past or family history.On examination his vitals were stable. General examination revealed marfanoid features including joint hyper mobility, high arched palate and arm span to height ratio greater than one. Neurological examination showed left pronator drift, brisk reflexes and an extensor plantar response on the left side.
His routine lab investigations (CBC, RFT, LFT, ESR, CRP) including autoimmune profile (ANA, APLA), serum homocysteine were normal.
MRI brain [Figure 3] demonstrated an acute ischemic infarct in the right frontal lobe with diffusion restriction. MR angiogram was normal.
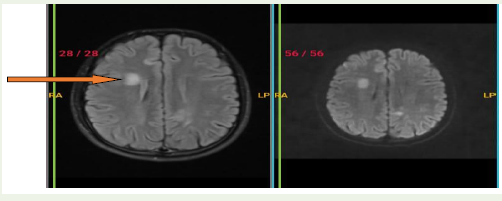
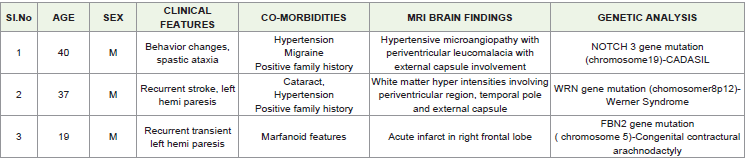
In view of the marfanoid habitus and recurrent transient ischemic
episodes genetic testing was performed which revealed an FBN2
missense mutation suggestive of contractural arachnodactyly.
Discussion
Stroke remains a major cause of mortality and long-term
disability worldwide. It is a heterogeneous condition resulting from a
complex interplay of environmental and genetic factors. The TOAST
classification categorizes ischemic stroke into five etiological subtypes:
large artery atherosclerosis, small vessel disease, cardio embolism,
stroke of other determined etiology, and stroke of undetermined
etiology [3].
Genetic causes should be considered in young stroke patients, especially when conventional vascular risk factors, systemic disorders, and cardiac etiologies are absent. The most common monogenic disorders associated with stroke include cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), Fabry disease, mitochondrial encephalopathy with lactic acidosis and stroke-like episodes (MELAS), COL4A1-related disorders, cerebral autosomal recessive arteriopathy with subcortical infarcts and leukoencephalopathy (CARASIL), and hereditary endotheliopathy with retinopathy, nephropathy, and stroke (HERNS).
CADASIL is the most common monogenic cerebral small vessel disease and is caused by cysteine-altering pathogenic variants in the NOTCH3 gene located on chromosome 19. More than 280 pathogenic NOTCH3 mutations have been described, including deletions, duplications, and splice-site mutations. Approximately 95% are pathogenic missense variants. Clinical manifestations include migraine, ischemic episodes, cognitive impairment, psychiatric disturbances, and acute reversible encephalopathy [4], many of which were observed in our patient. MRI brain typically demonstrates subcortical infarcts and white matter hyperintensities involving the anterior temporal lobe and external capsule, which are characteristic imaging findings. Diagnosis is confirmed by genetic testing, and treatment remains largely supportive.
Genetic causes should be considered in young stroke patients, especially when conventional vascular risk factors, systemic disorders, and cardiac etiologies are absent. The most common monogenic disorders associated with stroke include cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), Fabry disease, mitochondrial encephalopathy with lactic acidosis and stroke-like episodes (MELAS), COL4A1-related disorders, cerebral autosomal recessive arteriopathy with subcortical infarcts and leukoencephalopathy (CARASIL), and hereditary endotheliopathy with retinopathy, nephropathy, and stroke (HERNS).
CADASIL is the most common monogenic cerebral small vessel disease and is caused by cysteine-altering pathogenic variants in the NOTCH3 gene located on chromosome 19. More than 280 pathogenic NOTCH3 mutations have been described, including deletions, duplications, and splice-site mutations. Approximately 95% are pathogenic missense variants. Clinical manifestations include migraine, ischemic episodes, cognitive impairment, psychiatric disturbances, and acute reversible encephalopathy [4], many of which were observed in our patient. MRI brain typically demonstrates subcortical infarcts and white matter hyperintensities involving the anterior temporal lobe and external capsule, which are characteristic imaging findings. Diagnosis is confirmed by genetic testing, and treatment remains largely supportive.
Werner syndrome is a rare autosomal recessive disorder caused
by loss-of-function mutations in the WRN gene on chromosome
8p12. It is characterized by features of premature aging, including
early cataracts, premature atherosclerosis, osteoporosis, and type
2 diabetes mellitus [5]. Diagnosis is established through genetic
evaluation, while treatment is primarily supportive and focused on
management of vascular risk factors.
Congenital contractural arachnodactyly (CCA) exhibits a broad phenotypic spectrum. Classical CCA is characterized by arachnodactyly, flexion contractures involving multiple joints, kyphoscoliosis, marfanoid habitus, highly arched palate, muscular hypoplasia, and characteristic crumpled ears [6]. The clinical phenotype can vary considerably within affected families. Although cerebrovascular involvement is uncommon, connective tissue abnormalities may predispose affected individuals to vascular complications.
Congenital contractural arachnodactyly (CCA) exhibits a broad phenotypic spectrum. Classical CCA is characterized by arachnodactyly, flexion contractures involving multiple joints, kyphoscoliosis, marfanoid habitus, highly arched palate, muscular hypoplasia, and characteristic crumpled ears [6]. The clinical phenotype can vary considerably within affected families. Although cerebrovascular involvement is uncommon, connective tissue abnormalities may predispose affected individuals to vascular complications.
Conclusion
Monogenic diseases are rare but important causes of stroke
in young individuals and are frequently under diagnosed. Due
to overlapping phenotypes and marked intrafamilial variability,
diagnosis can be challenging. However characteristic clinical features
and neuroimaging findings may provide important clues to the
underlying genetic etiology.
Although genetic testing is expensive, it should be considered as part of diagnostic workup in young patients with cerebrovascular events, particularly when conventional vascular risk factors are absent or when there is a positive family history. Early diagnosis facilitates appropriate management, genetic counseling and prognostication.
Although genetic testing is expensive, it should be considered as part of diagnostic workup in young patients with cerebrovascular events, particularly when conventional vascular risk factors are absent or when there is a positive family history. Early diagnosis facilitates appropriate management, genetic counseling and prognostication.
Acknowledgement
We would like to acknowledge the patient and their families for
their cooperation and consent for publication of this case series. We
also appreciate the efforts of the entire medical team involved in
patient care.
References
Citation
Bilia KA, Nagendra S, Ojha P, Jagiasi K, Mahto A, et al. A Case Series of Monogenic Strokes in A Tertiary Care Centre. Indian J Neurol. 2026;7(1): 170.