Research Article
Clinician Perspectives on the Use of Pregabalin and Combination Therapy in Neuropathic Pain Management: A Nationwide Survey
Manjula S* and Krishna Kumar M
Department of Medical Services, Micro Labs Limited, Bangalore, Karnataka, India
*Corresponding author:Dr Manjula S, Department of Medical Services, Micro Labs Limited, Bangalore, Karnataka, India, E-mail Id: drmanjulas@gmail.com
Article Information:Submission: 08/05/2026; Accepted: 03/06/2026; Published: 05/06/2026
Copyright: © 2026 Manjula S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Neuropathic pain is a complex, chronic condition often associated with comorbidities such as diabetes. Understanding clinical practice patterns and clinicians’ perspectives is essential to optimizing management strategies, including the use of pregabalin and combination therapies. The present survey is intended to assess clinical practice patterns in neuropathic pain management and gather clinicians’ insights on the use of pregabalin and
its combination therapies in routine practice.
Methods: The nationwide cross-sectional survey was conducted among clinicians managing neuropathic pain across India. A 22-item questionnaire was distributed via email and online platforms. Participation was voluntary, informed consent was obtained, and responses were analyzed using descriptive statistics.
Results: Among 343 survey participants, 51% of clinicians reported that 26–50% of their neuropathic pain patients have comorbid diabetes. Nearly 47% of clinicians identified burning sensation as the most common symptom reported by patients. About 54% preferred a benfotiamine–mecobalamin combination for 90 days in neuropathy management. Approximately 64% of respondents indicated that 26–50% of their neuropathy patients are treated with pregabalin. Around 48% of clinicians considered improved nerve function, antioxidant effects, and better bioavailability compared with thiamine as major advantages of benfotiamine. Additionally, 70% of respondents reported patient reluctance to take medications as the most common barrier to effective neuropathic pain treatment. The majority (65%) regularly monitored patients receiving multiple combination supplements, and 63% observed marked clinical improvement with pregabalin based on a 5-point global improvement scale.
Conclusion: This survey highlights neuropathic pain management, showing that diabetes is a common comorbidity and burning sensation is a frequent symptom. Pregabalin and combination therapies demonstrate clinical improvement, although patient reluctance remains a significant barrier.
Methods: The nationwide cross-sectional survey was conducted among clinicians managing neuropathic pain across India. A 22-item questionnaire was distributed via email and online platforms. Participation was voluntary, informed consent was obtained, and responses were analyzed using descriptive statistics.
Results: Among 343 survey participants, 51% of clinicians reported that 26–50% of their neuropathic pain patients have comorbid diabetes. Nearly 47% of clinicians identified burning sensation as the most common symptom reported by patients. About 54% preferred a benfotiamine–mecobalamin combination for 90 days in neuropathy management. Approximately 64% of respondents indicated that 26–50% of their neuropathy patients are treated with pregabalin. Around 48% of clinicians considered improved nerve function, antioxidant effects, and better bioavailability compared with thiamine as major advantages of benfotiamine. Additionally, 70% of respondents reported patient reluctance to take medications as the most common barrier to effective neuropathic pain treatment. The majority (65%) regularly monitored patients receiving multiple combination supplements, and 63% observed marked clinical improvement with pregabalin based on a 5-point global improvement scale.
Conclusion: This survey highlights neuropathic pain management, showing that diabetes is a common comorbidity and burning sensation is a frequent symptom. Pregabalin and combination therapies demonstrate clinical improvement, although patient reluctance remains a significant barrier.
Keywords: Neuropathic Pain; Diabetic Neuropathy; Benfotiamine; Mecobalamin; Pregabalin, Combination Supplementation
Introduction
Neuropathic pain, defined by the International Association
for the Study of Pain (IASP) as pain caused by damage or disease
affecting the somatosensory nervous system, affects approximately
7-8% of adults and is commonly linked to chronic pain conditions.
[1] Its incidence is about 8 cases per 1,000 person-years. Neuropathic
pain occurs in roughly 37% of patients with chronic low back pain,
26% of individuals with diabetes, 35% of people living with HIV, and
20% of cancer patients. It may also arise after surgery or conditions
such as postherpetic neuralgia following shingles.[2] In India, the
overall prevalence of peripheral neuropathy is 75.4%, with mild cases
most common (53.9%), followed by moderate (16.8%) and severe
(4.7%) forms. Prevalence is higher among individuals with diabetes
(90.1%) than non-diabetics (65.3%), slightly higher in males (75.8%),
and shows regional variation from 74.3% to 79.3%, with the Eastern
zone reporting the highest proportion of moderate and severe cases.
[3].
Among the available pharmacological treatments, pregabalin is widely used as a first-line therapy due to its proven efficacy in reducing neuropathic pain and improving sleep quality and functional outcomes.[4] It exerts its therapeutic effects primarily by binding to the α2-δ subunit of presynaptic voltage-gated calcium channels in the central nervous system. This binding reduces calcium influx and modulates the release of excitatory neurotransmitters such as glutamate, substance P, norepinephrine, and calcitonin gene-related peptide, thereby contributing to its antinociceptive and anticonvulsant effects. Pregabalin also inhibits the trafficking of these calcium channel subunits from the dorsal root ganglia to the spinal dorsal horn. Although structurally related to gamma-aminobutyric acid (GABA), it does not bind to GABA or benzodiazepine receptors. [5].
In clinical practice, pregabalin is frequently prescribed either as monotherapy or in combination with other medications to enhance pain relief and improve treatment tolerability.[6] However, treatment strategies may vary among clinicians depending on patient characteristics, symptom severity, and the presence of comorbid conditions. Therefore, evaluating clinical practice patterns is essential to better understand how neuropathic pain is managed outside controlled clinical trial settings. The present survey aims to assess current treatment approaches and gather clinicians’ perspectives regarding the use of pregabalin and its combination therapies in routine clinical practice.
Among the available pharmacological treatments, pregabalin is widely used as a first-line therapy due to its proven efficacy in reducing neuropathic pain and improving sleep quality and functional outcomes.[4] It exerts its therapeutic effects primarily by binding to the α2-δ subunit of presynaptic voltage-gated calcium channels in the central nervous system. This binding reduces calcium influx and modulates the release of excitatory neurotransmitters such as glutamate, substance P, norepinephrine, and calcitonin gene-related peptide, thereby contributing to its antinociceptive and anticonvulsant effects. Pregabalin also inhibits the trafficking of these calcium channel subunits from the dorsal root ganglia to the spinal dorsal horn. Although structurally related to gamma-aminobutyric acid (GABA), it does not bind to GABA or benzodiazepine receptors. [5].
In clinical practice, pregabalin is frequently prescribed either as monotherapy or in combination with other medications to enhance pain relief and improve treatment tolerability.[6] However, treatment strategies may vary among clinicians depending on patient characteristics, symptom severity, and the presence of comorbid conditions. Therefore, evaluating clinical practice patterns is essential to better understand how neuropathic pain is managed outside controlled clinical trial settings. The present survey aims to assess current treatment approaches and gather clinicians’ perspectives regarding the use of pregabalin and its combination therapies in routine clinical practice.
Methodology
Study Settings:
A cross-sectional study was carried out among clinicians involved
in the management of patients with neuropathic pain in the major
Indian cities from June 2025 to December 2025. The study was
performed in accordance with Bangalore Ethics, an Independent
Ethics Committee (ECR/355/Indt/KA/2022), which was recognized
by the Indian Regulatory Authority, the Drug Controller General of
India.Study Participants:
An invitation was sent to leading clinicians in managing
neuropathic pain in the month of March 2025 for participation
in this Indian survey. About 343 clinicians from major cities of all
Indian states, representing the geographical distribution, shared their
willingness to participate and provide necessary data.Study Procedure:
The questionnaire booklet titled PECOM (Pregabalin and
Its Combination in the Management of Neuropathic Pain) study
was sent to the clinicians who were interested in participating in
the survey. The study questionnaire comprised 22 questions that
explored aspects such as common etiologies and symptoms of
neuropathic pain, comorbid conditions, diagnostic approaches,
treatment preferences, use of nutritional supplements, usage patterns
of pregabalin and combination therapies, perceived effectiveness,
adverse effects, and barriers to treatment. Reliability, as determined
by a split-half test (coefficient alpha), was adequate but should be
improved in future versions of the questionnaire. A study of criterion
validity was undertaken to test the questionnaire and to develop
methods of testing the validity of measures of Physicians’ Perspectives.
However, the extraneous variables in this include the clinician’s
experience, usage of the newer drugs, etc. The two criteria used were
the doctors’ perspectives from the clinical practice and the assessment
of an external assessor and statistician. Clinicians had the option to
skip questions as desired and were instructed to complete the survey
independently, without peer consultation. Before participating in the
survey, all respondents provided written informed consent.Statistical analysis:
Survey responses were analyzed using descriptive statistical
methods. Categorical variables were summarized as frequencies and
percentages. Data visualization, including bar charts and pie charts,
was performed using Microsoft Excel 2013 (version 16.0.13901.20400).Results
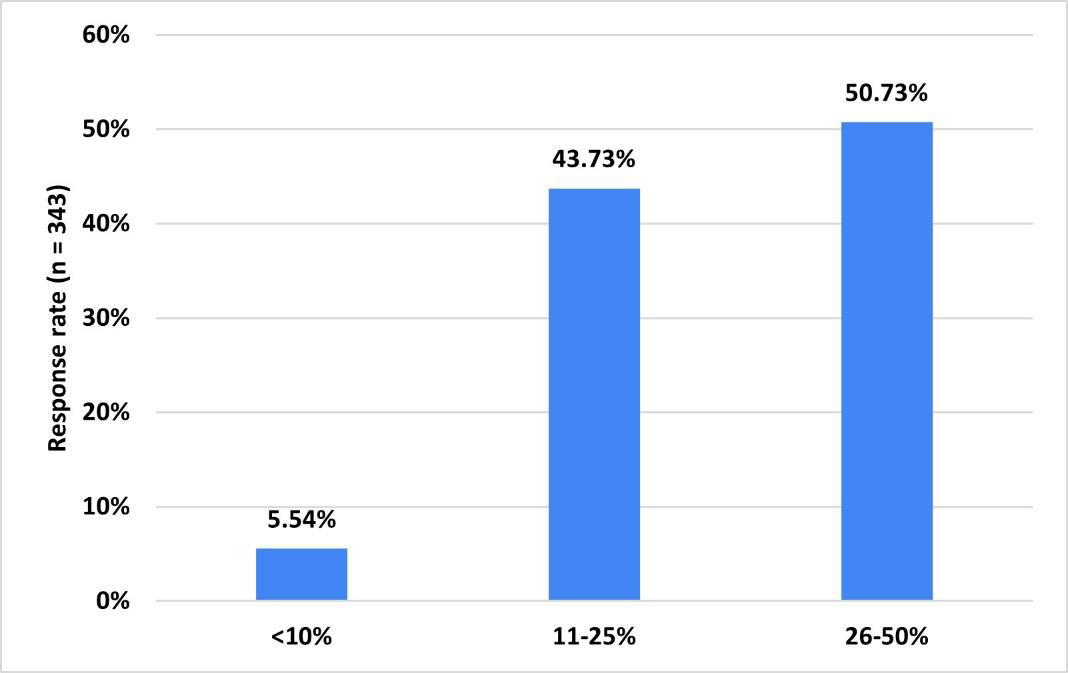
The survey included 343 practitioners; half (50.73%) of the
respondents reported that 26-50% of their patients with neuropathic
pain have comorbid diabetes in clinical practice [Figure 1]. Nearly
half (48.4-) of clinicians reported that 11-25% of their patients present
with postherpetic neuralgia in clinical practice. Approximately 50%
of respondents reported that 10–20% of their patients are affected
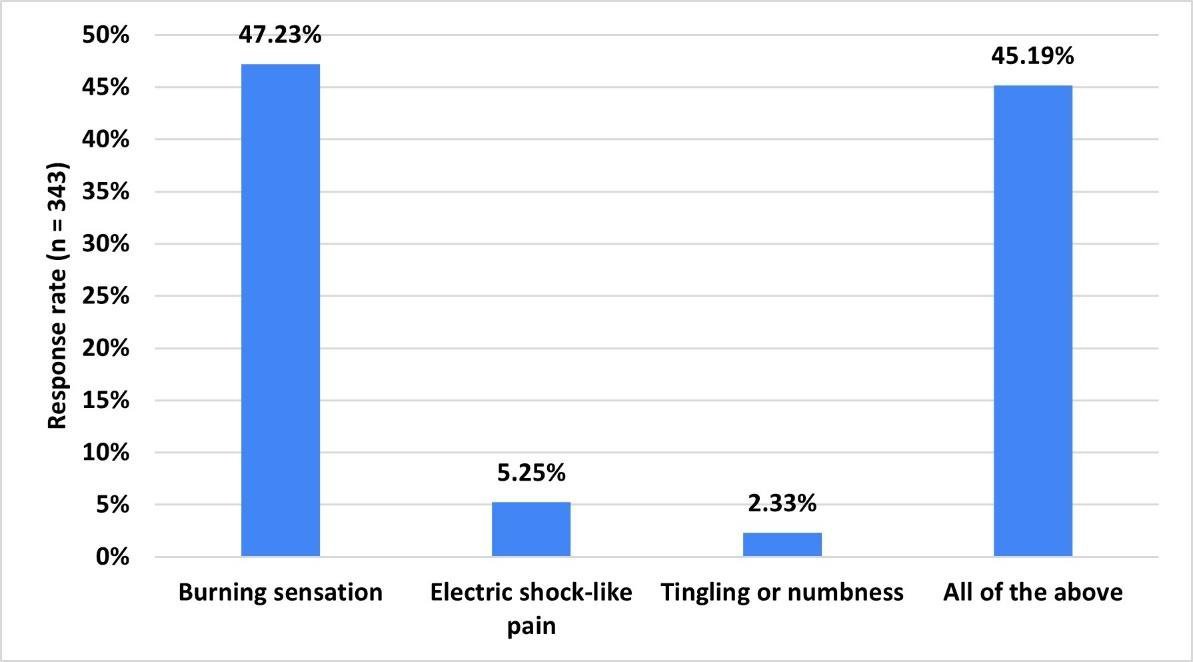
by alcohol-induced neuropathy. About 47% of clinicians identified
burning sensation as the most common symptom of neuropathic
pain in their practice [Figure 2].
Approximately 51% of respondents identified nerve compression
or injury as a causative factor for neuropathic pain in 11–20%
of patients. A large majority (88.63%) of clinicians reported that
patients with neuropathy commonly present with disturbed sleep.
Approximately 51% of respondents estimated that 11-25% of their
neuropathy patients have vitamin B12 deficiency. About 44% of
clinicians indicated burning feet as a complication of vitamin B12
deficiency affecting 21-30% of the relevant patient population.
The majority (62.68%) of respondents reported that 21-30% of
neuropathy patients are treated with benfotiamine in combination
with vitamin B12. Similarly, about 58% of respondents indicated that
26-50% of neuropathy patients are treated with pregabalin 75 mg plus
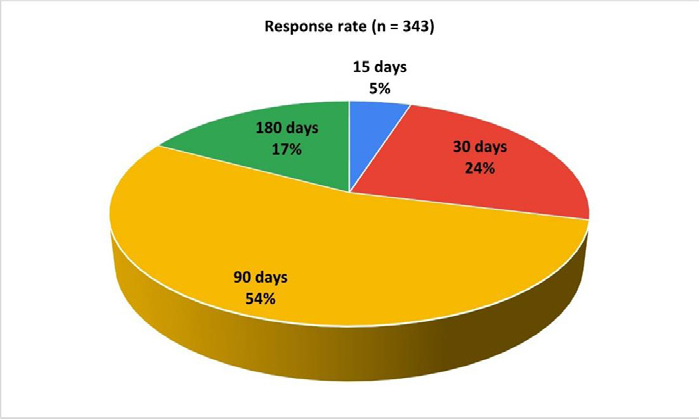
methylcobalamin 750 mcg capsules. Approximately 54% of clinicians
reported recommending a benfotiamine–mecobalamin combination
for 90 days in patients with neuropathy in clinical practice [Figure 3].
About 45% of respondents reported evaluating 11–20% of patients
with neuropathic pain using a biothesiometer in clinical practice.
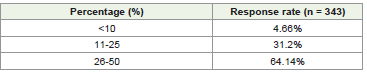
Nearly two-thirds (64.14%) of clinicians reported that 26-50% of their
neuropathy patients are treated with pregabalin in clinical practice,
either as an initial pharmacological option or as part of combination
therapy [Table 1]. About 34% of participants considered alphalipoic
acid to be very effective in slowing the progression of diabetic
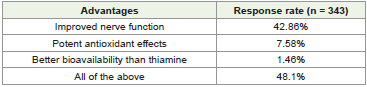
neuropathy. According to 48% of respondents, improved nerve
function, potent antioxidant effects, and better bioavailability than
thiamine are key advantages of benfotiamine [Table 2].
Approximately 46% of clinicians reported that the reduction
of pain and paresthesia, neutralization of free radicals due to its
strong antioxidant properties, and enhancement of microcirculation
around nerves are the mechanisms through which alpha-lipoic acid
improves outcomes in neuropathic pain. More than half (55.39%) of
respondents reported that 21-30% of their neuropathic pain patients
are treated with a combination of pregabalin and nortriptyline.
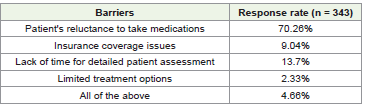
Approximately 70% of respondents stated that patient reluctance to
take medications is the most frequently cited barrier to the treatment
of neuropathic pain [Table 3].
Approximately 38% of clinicians reported recommending the
combination of benfotiamine 150 mg, methylcobalamin 1.5 mg,
alpha-lipoic acid 100 mg, chromium 200 mcg, selenium 55 mcg,
folic acid 1.5 mg, and inositol 100 mg soft gelatin capsules to 41-
60% of their neuropathy patients, either as a first-line therapy or
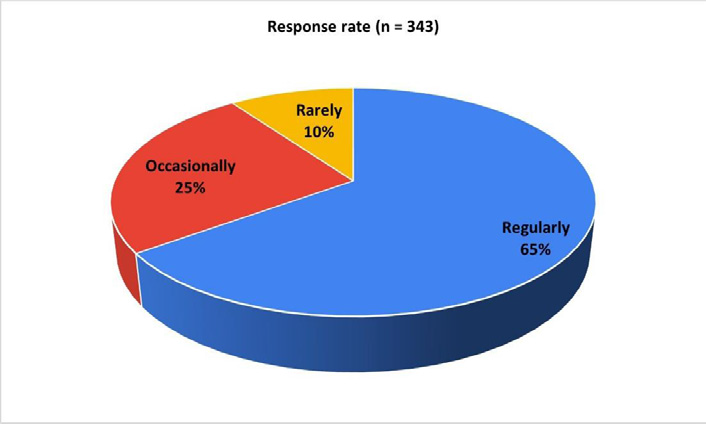
as an add-on treatment. Approximately 65% of clinicians reported
regularly monitoring patients receiving multiple combination
supplementation for neuropathic pain to detect potential adverse
effects or complications [Figure 4]. Nearly half (48.98%) of
respondents observed adverse drug reactions to pregabalin in their
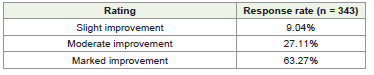
neuropathic pain patients. Approximately 63% indicated marked
improvement in their patients for outcomes with pregabalin, which
are assessed using a 5-point global improvement scale [Table 4].
Discussion
The survey findings highlight the multifactorial nature of
neuropathic pain, including its associated comorbidities, diagnostic
approaches, pharmacological strategies, and barriers that influence
treatment outcomes in routine clinical settings. A substantial
proportion of clinicians in the present survey reported that 26–50% of
their neuropathic pain patients have comorbid diabetes, highlighting
the strong association between neuropathy and diabetes. Diabetes
mellitus remains one of the most common causes of peripheral
neuropathy, primarily due to chronic hyperglycemia, oxidative
stress, metabolic disturbances, and microvascular damage affecting
peripheral nerves. These pathophysiological mechanisms contribute
to progressive nerve dysfunction and the development of diabetic
neuropathy.[3]
Supporting this observation, Nicholson and Verma reported that neuropathic pain frequently occurs in association with several comorbid conditions, among which diabetes mellitus is one of the most common underlying causes.[7] Similarly, Mayur Mayabhate reported that diabetes represents one of the most prevalent comorbidities associated with neuropathic pain, with observational studies indicating that approximately 26–50% of patients with neuropathic pain in clinical practice have diabetes mellitus.[8] These findings further emphasize the substantial burden of diabetic neuropathy in routine clinical practice and highlight the importance of early screening, optimal glycemic control, and integrated management strategies for neuropathic pain in diabetic populations. The survey also revealed that burning sensation is the most commonly reported symptom of neuropathic pain in clinical practice. This symptom is characteristic of neuropathic pain syndromes and is typically associated with abnormal sensory nerve signaling and peripheral nerve damage. According to the study by Mayabhate, the most common symptom of neuropathic pain in India is a burning sensation, which was reported by 68.5% of participants in a retrospective, multi center, cross-sectional observational study. [8] In a survey assessing neuropathic pain symptoms in primary care, Pollack et al. reported that burning pain was one of the most commonly described symptoms, affecting 47.6% of patients.[9] Similarly, Attal et al. reported that approximately 65% of patients with neuropathic pain experience ongoing burning pain in clinical practice.[10]
The present survey found that the majority of clinicians reported prescribing a benfotiamine and mecobalamin combination for approximately 90 days in patients with neuropathy. This prescribing pattern suggests that clinicians prefer a relatively extended duration of therapy to achieve optimal neurological recovery and symptomatic relief. Similarly, a previous survey conducted by the current authors reported that 43% of clinicians recommended a 12-week duration for benfotiamine and methylcobalamin combination therapy in patients with neuropathy.[11] Evidence from clinical studies also supports the therapeutic role of benfotiamine in neuropathic conditions. Stracke et al. conducted a randomized, placebo-controlled clinical trial demonstrating that benfotiamine (300–600 mg/day) significantly improved neuropathy symptom scores, particularly pain, in patients with diabetic polyneuropathy.[12] Likewise, in another placebo controlled trial, Haupt et al. reported that benfotiamine therapy significantly reduced neuropathy symptom scores and alleviated pain, highlighting its potential benefits in the management of diabetic polyneuropathy.[13]
Nearly two-thirds of respondents in the current survey reported that 26–50% of their neuropathy patients are treated with pregabalin, indicating its widespread use in routine clinical practice for the management of neuropathic pain. This observation is consistent with previous prescribing pattern studies. Madkholkar et al. reported that pregabalin-based regimens were among the most commonly prescribed treatments for neuropathic pain, with 48.5% of patients receiving pregabalin in combination with methylcobalamin.[14] Substantial clinical evidence supports the effectiveness of pregabalin in neuropathic pain management. Multiple studies have demonstrated that pregabalin significantly reduces pain intensity and improves sleep quality as well as overall quality-of-life indicators in patients with diabetic peripheral neuropathy. [15,16] These therapeutic benefits are primarily attributed to its ability to modulate calcium channel activity and reduce excitatory neurotransmitter release within the central nervous system. Further supporting its clinical utility, a three-week prospective study by Sule et al. reported that pregabalin significantly reduced pain scores in patients with peripheral neuropathic pain and was generally well tolerated, reinforcing its role as an effective pharmacological option for neuropathic pain management.[17] According to the current survey findings, clinicians perceived improved nerve function, antioxidant activity, and superior bioavailability compared with thiamine as the key advantages of benfotiamine in neuropathy management. These perceptions are supported by Xie et al., who demonstrated in a pharmacokinetic study that oral benfotiamine produced markedly higher plasma thiamine and erythrocyte thiamine diphosphate levels compared with thiamine hydrochloride, indicating substantially greater systemic bioavailability.[18] Similarly, Bozic and Lavrnja reported that benfotiamine provides several therapeutic advantages, including improved nerve function, antioxidant activity, and enhanced bioavailability relative to conventional thiamine formulations.[19]
Furthermore, Volvert et al. highlighted the antioxidant and antiinflammatory properties of benfotiamine, suggesting its potential neuroprotective role in conditions associated with oxidative stress and metabolic dysfunction.[20]
Patient reluctance to take medications was the most frequently cited barrier to the treatment of neuropathic pain in the present survey. Such reluctance may arise from concerns about adverse effects, limited awareness of treatment benefits, or hesitation to add additional medications to existing treatment regimens. Supporting these findings, Rees et al. reported that many patients expressed concerns about taking medications for neuropathic pain, including fears of side effects, inadequate knowledge about the prescribed drugs, and reluctance to increase their medication burden.
Approximately 51% of patients reported concerns regarding the use of medications, highlighting patient reluctance as a significant barrier to effective treatment.[21] Similarly, Shrestha et al., in a prospective study assessing medication adherence patterns among patients with neuropathic pain, reported that more than 50% of patients were nonadherent to their prescribed medications, indicating the presence of substantial patient-related barriers that may negatively affect treatment outcomes.[22] These findings emphasize the importance of patient education, counseling, and shared decision-making to improve adherence and optimize the management of neuropathic pain in routine clinical practice.
The present survey also underscored the importance of regularly monitoring patients with neuropathic pain who are receiving multiple combination supplements. Consistent with these findings, Balanaser et al., in their systematic review on combination pharmacotherapy for neuropathic pain, reported that when multiple agents are used, clinicians should conduct closely monitored individualized dosing trials to ensure safety and detect adverse effects.[23] Similarly, Deng et al. in their study reported that regular monitoring and follow-up are essential components of neuropathic pain management due to the complexity of pharmacological treatment and risk of adverse effects. [24]
The current survey noted marked improvement in patients treated with pregabalin, with outcomes assessed using a 5-point global improvement scale. This finding suggests that pregabalin remains an effective therapeutic option for managing neuropathic pain in routine clinical practice. Consistent with this observation, a multicentre open-label clinical study evaluating pregabalin in patients with peripheral neuropathic pain reported significant reductions in pain scores along with improvements in both patient- and clinician rated global impression scores. The study further demonstrated that pregabalin was safe, well-tolerated, and effective in the management of peripheral neuropathic pain among Indian patients.[17] Similarly, Srivastava et al. conducted a comparative study evaluating sustained release pregabalin and immediate-release pregabalin for the treatment of diabetic peripheral neuropathy. Treatment outcomes were assessed using the Clinical Global Impression–Improvement (CGI-I) and Clinical Global Impression–Severity (CGI-S) scales. The study reported significant improvements in neuropathic pain scores and overall clinical outcomes after 12 weeks of treatment, further supporting the effectiveness of pregabalin in neuropathic pain management [25]
The key strength of this survey is the nationwide participation of clinicians across diverse clinical settings, which offers a broader understanding of treatment approaches for neuropathic pain.
Additionally, the relatively large sample size of practitioners enhances the representativeness of the findings and provides useful information on current clinical practices. However, several limitations should be acknowledged. As the survey relied on self-reported responses from clinicians, the findings may be influenced by individual clinical experience and subjective judgment, which could introduce potential reporting bias. Furthermore, the cross-sectional design captures clinical practices and perceptions at a single point in time and may not fully reflect evolving trends in neuropathic pain management. In addition, the survey did not include patient-level clinical data or objective outcome measures, which limits the ability to directly correlate reported treatment approaches with actual outcomes. The questionnaire also did not specifically evaluate whether pregabalin was consistently preferred as first-line therapy, patterns of switching from pregabalin or its combination therapies to alternative medications, or the timing and reasons for such treatment modifications in clinical practice. These factors should be considered when interpreting the findings, and future prospective studies incorporating patient-level clinical data are warranted to further validate and expand upon these observations.
Supporting this observation, Nicholson and Verma reported that neuropathic pain frequently occurs in association with several comorbid conditions, among which diabetes mellitus is one of the most common underlying causes.[7] Similarly, Mayur Mayabhate reported that diabetes represents one of the most prevalent comorbidities associated with neuropathic pain, with observational studies indicating that approximately 26–50% of patients with neuropathic pain in clinical practice have diabetes mellitus.[8] These findings further emphasize the substantial burden of diabetic neuropathy in routine clinical practice and highlight the importance of early screening, optimal glycemic control, and integrated management strategies for neuropathic pain in diabetic populations. The survey also revealed that burning sensation is the most commonly reported symptom of neuropathic pain in clinical practice. This symptom is characteristic of neuropathic pain syndromes and is typically associated with abnormal sensory nerve signaling and peripheral nerve damage. According to the study by Mayabhate, the most common symptom of neuropathic pain in India is a burning sensation, which was reported by 68.5% of participants in a retrospective, multi center, cross-sectional observational study. [8] In a survey assessing neuropathic pain symptoms in primary care, Pollack et al. reported that burning pain was one of the most commonly described symptoms, affecting 47.6% of patients.[9] Similarly, Attal et al. reported that approximately 65% of patients with neuropathic pain experience ongoing burning pain in clinical practice.[10]
The present survey found that the majority of clinicians reported prescribing a benfotiamine and mecobalamin combination for approximately 90 days in patients with neuropathy. This prescribing pattern suggests that clinicians prefer a relatively extended duration of therapy to achieve optimal neurological recovery and symptomatic relief. Similarly, a previous survey conducted by the current authors reported that 43% of clinicians recommended a 12-week duration for benfotiamine and methylcobalamin combination therapy in patients with neuropathy.[11] Evidence from clinical studies also supports the therapeutic role of benfotiamine in neuropathic conditions. Stracke et al. conducted a randomized, placebo-controlled clinical trial demonstrating that benfotiamine (300–600 mg/day) significantly improved neuropathy symptom scores, particularly pain, in patients with diabetic polyneuropathy.[12] Likewise, in another placebo controlled trial, Haupt et al. reported that benfotiamine therapy significantly reduced neuropathy symptom scores and alleviated pain, highlighting its potential benefits in the management of diabetic polyneuropathy.[13]
Nearly two-thirds of respondents in the current survey reported that 26–50% of their neuropathy patients are treated with pregabalin, indicating its widespread use in routine clinical practice for the management of neuropathic pain. This observation is consistent with previous prescribing pattern studies. Madkholkar et al. reported that pregabalin-based regimens were among the most commonly prescribed treatments for neuropathic pain, with 48.5% of patients receiving pregabalin in combination with methylcobalamin.[14] Substantial clinical evidence supports the effectiveness of pregabalin in neuropathic pain management. Multiple studies have demonstrated that pregabalin significantly reduces pain intensity and improves sleep quality as well as overall quality-of-life indicators in patients with diabetic peripheral neuropathy. [15,16] These therapeutic benefits are primarily attributed to its ability to modulate calcium channel activity and reduce excitatory neurotransmitter release within the central nervous system. Further supporting its clinical utility, a three-week prospective study by Sule et al. reported that pregabalin significantly reduced pain scores in patients with peripheral neuropathic pain and was generally well tolerated, reinforcing its role as an effective pharmacological option for neuropathic pain management.[17] According to the current survey findings, clinicians perceived improved nerve function, antioxidant activity, and superior bioavailability compared with thiamine as the key advantages of benfotiamine in neuropathy management. These perceptions are supported by Xie et al., who demonstrated in a pharmacokinetic study that oral benfotiamine produced markedly higher plasma thiamine and erythrocyte thiamine diphosphate levels compared with thiamine hydrochloride, indicating substantially greater systemic bioavailability.[18] Similarly, Bozic and Lavrnja reported that benfotiamine provides several therapeutic advantages, including improved nerve function, antioxidant activity, and enhanced bioavailability relative to conventional thiamine formulations.[19]
Furthermore, Volvert et al. highlighted the antioxidant and antiinflammatory properties of benfotiamine, suggesting its potential neuroprotective role in conditions associated with oxidative stress and metabolic dysfunction.[20]
Patient reluctance to take medications was the most frequently cited barrier to the treatment of neuropathic pain in the present survey. Such reluctance may arise from concerns about adverse effects, limited awareness of treatment benefits, or hesitation to add additional medications to existing treatment regimens. Supporting these findings, Rees et al. reported that many patients expressed concerns about taking medications for neuropathic pain, including fears of side effects, inadequate knowledge about the prescribed drugs, and reluctance to increase their medication burden.
Approximately 51% of patients reported concerns regarding the use of medications, highlighting patient reluctance as a significant barrier to effective treatment.[21] Similarly, Shrestha et al., in a prospective study assessing medication adherence patterns among patients with neuropathic pain, reported that more than 50% of patients were nonadherent to their prescribed medications, indicating the presence of substantial patient-related barriers that may negatively affect treatment outcomes.[22] These findings emphasize the importance of patient education, counseling, and shared decision-making to improve adherence and optimize the management of neuropathic pain in routine clinical practice.
The present survey also underscored the importance of regularly monitoring patients with neuropathic pain who are receiving multiple combination supplements. Consistent with these findings, Balanaser et al., in their systematic review on combination pharmacotherapy for neuropathic pain, reported that when multiple agents are used, clinicians should conduct closely monitored individualized dosing trials to ensure safety and detect adverse effects.[23] Similarly, Deng et al. in their study reported that regular monitoring and follow-up are essential components of neuropathic pain management due to the complexity of pharmacological treatment and risk of adverse effects. [24]
The current survey noted marked improvement in patients treated with pregabalin, with outcomes assessed using a 5-point global improvement scale. This finding suggests that pregabalin remains an effective therapeutic option for managing neuropathic pain in routine clinical practice. Consistent with this observation, a multicentre open-label clinical study evaluating pregabalin in patients with peripheral neuropathic pain reported significant reductions in pain scores along with improvements in both patient- and clinician rated global impression scores. The study further demonstrated that pregabalin was safe, well-tolerated, and effective in the management of peripheral neuropathic pain among Indian patients.[17] Similarly, Srivastava et al. conducted a comparative study evaluating sustained release pregabalin and immediate-release pregabalin for the treatment of diabetic peripheral neuropathy. Treatment outcomes were assessed using the Clinical Global Impression–Improvement (CGI-I) and Clinical Global Impression–Severity (CGI-S) scales. The study reported significant improvements in neuropathic pain scores and overall clinical outcomes after 12 weeks of treatment, further supporting the effectiveness of pregabalin in neuropathic pain management [25]
The key strength of this survey is the nationwide participation of clinicians across diverse clinical settings, which offers a broader understanding of treatment approaches for neuropathic pain.
Additionally, the relatively large sample size of practitioners enhances the representativeness of the findings and provides useful information on current clinical practices. However, several limitations should be acknowledged. As the survey relied on self-reported responses from clinicians, the findings may be influenced by individual clinical experience and subjective judgment, which could introduce potential reporting bias. Furthermore, the cross-sectional design captures clinical practices and perceptions at a single point in time and may not fully reflect evolving trends in neuropathic pain management. In addition, the survey did not include patient-level clinical data or objective outcome measures, which limits the ability to directly correlate reported treatment approaches with actual outcomes. The questionnaire also did not specifically evaluate whether pregabalin was consistently preferred as first-line therapy, patterns of switching from pregabalin or its combination therapies to alternative medications, or the timing and reasons for such treatment modifications in clinical practice. These factors should be considered when interpreting the findings, and future prospective studies incorporating patient-level clinical data are warranted to further validate and expand upon these observations.
Conclusion
The present survey highlights diabetes as a common comorbidity
and burning sensation as a frequent symptom. Pregabalin and
combination therapies, including benfotiamine and mecobalamin,
are widely used and are perceived by clinicians to improve clinical
outcomes. However, patient reluctance to take medications remains
a significant barrier to effective treatment. These findings emphasize
the need for optimized therapeutic strategies and improved patient
education to enhance treatment adherence and outcomes in
neuropathic pain management.
Acknowledgement
We would like to thank all the clinicians who participated in this study.
References
Citation
Manjula S, Krishna Kumar M. Clinician Perspectives on the Use of Pregabalin and Combination Therapy in Neuropathic Pain Management: A Nationwide Survey. Indian J Neurol. 2026;7(1): 169.