Research Article
Correlation of Plasma D-Dimer Levels with Stroke Severity and Short-Term Outcome in Patients with Acute Ischemic Stroke: A Cross-Sectional Study
Kumar V*, Siddiqui A and Kumar S
Department of Medicine All India Institute of Medical Sciences (AIIMS), Patna, Bihar, India
*Corresponding author: Dr. Vijay Kumar, Department of Medicine All India Institute of Medical Sciences (AIIMS), Patna, Bihar, India. E-mail Id: vk1994@gmail.com
Article Information:Submission: 22/04/2026; Accepted: 14/05/2026; Published: 16/05/2026
Copyright: © 2026 Kumar V, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Stroke is a leading cause of death and disability globally, with ischemic stroke accounting for approximately 85% of all cases. While clinical scales like the NIHSS and mRS are widely used for early assessment and prognosis, biochemical markers such as D-dimer are gaining interest for their potential to enhance prognostication. Elevated D-dimer levels, a fibrin degradation product, indicate thrombotic activity and may correlate with stroke severity, etiology, and functional outcomes.
Methods: A total of 140 adult patients (≥18 years) with confirmed acute ischemic stroke, admitted within 48 hours of symptom onset, were includedwas to determine the correlation between admission plasma D-dimer levels and stroke severity using the NIHSS, also association between initial D-dimer and mRSat 4 weeks. Clinical data, risk factors, NIHSS at admission, and plasma D-dimer levelswere collected. Functional outcome was assessed at 4 weeks using the mRS. Spearman’s correlation and chi-square tests were used, with p-values <0.05 considered statistically significant.
Results: 74.3% of patients had elevated D-dimer levels (>0.5 ug/mL). A statistically significant positive correlation was observed between D-dimer levels and NIHSS scores (Spearman’s ρ = 0.581, p < 0.001), indicating higher D-dimer correlates with greater stroke severity. Similarly, a significant positive correlation was found between D-dimer levels and mRS scores at 28 days (Spearman’s ρ = 0.601, p < 0.001), suggesting a link to poorer functional outcomes. Chi-square analyses further confirmed strong associations between elevated D-dimer and both increased stroke severity (χ²(1) = 28.3, p < 0.001) and poor functional outcomes (χ²(1) = 34.3, p < 0.001).
Conclusion: This study highlights a significant association between elevated plasma D-dimer levels and both the severity and short-term functional outcome of acute ischemic stroke. D-dimer can be used to complement clinical scales for early risk stratification, guiding acute management decisions, and predicting recovery trajectories.
• What is already known on this topic -D-dimer is recognized as a marker of thrombotic activity and stroke prognosis and its correlation with severity and outcome has been established in some studies.
• What this study adds -This study demonstrates a significant positive correlation between elevated D-dimer levels at admission and both increased stroke severity (NIHSS) and poorer short-term functional outcomes (mRS) in an Indian cohort confirming previous findings.
• How this study might affect research, practice or policy -D-dimer testing can be integrated into emergency stroke protocols for early risk stratification and guiding management. Future research can build on this by exploring serial D-dimer measurements and developing personalized stroke management models.
Methods: A total of 140 adult patients (≥18 years) with confirmed acute ischemic stroke, admitted within 48 hours of symptom onset, were includedwas to determine the correlation between admission plasma D-dimer levels and stroke severity using the NIHSS, also association between initial D-dimer and mRSat 4 weeks. Clinical data, risk factors, NIHSS at admission, and plasma D-dimer levelswere collected. Functional outcome was assessed at 4 weeks using the mRS. Spearman’s correlation and chi-square tests were used, with p-values <0.05 considered statistically significant.
Results: 74.3% of patients had elevated D-dimer levels (>0.5 ug/mL). A statistically significant positive correlation was observed between D-dimer levels and NIHSS scores (Spearman’s ρ = 0.581, p < 0.001), indicating higher D-dimer correlates with greater stroke severity. Similarly, a significant positive correlation was found between D-dimer levels and mRS scores at 28 days (Spearman’s ρ = 0.601, p < 0.001), suggesting a link to poorer functional outcomes. Chi-square analyses further confirmed strong associations between elevated D-dimer and both increased stroke severity (χ²(1) = 28.3, p < 0.001) and poor functional outcomes (χ²(1) = 34.3, p < 0.001).
Conclusion: This study highlights a significant association between elevated plasma D-dimer levels and both the severity and short-term functional outcome of acute ischemic stroke. D-dimer can be used to complement clinical scales for early risk stratification, guiding acute management decisions, and predicting recovery trajectories.
• What is already known on this topic -D-dimer is recognized as a marker of thrombotic activity and stroke prognosis and its correlation with severity and outcome has been established in some studies.
• What this study adds -This study demonstrates a significant positive correlation between elevated D-dimer levels at admission and both increased stroke severity (NIHSS) and poorer short-term functional outcomes (mRS) in an Indian cohort confirming previous findings.
• How this study might affect research, practice or policy -D-dimer testing can be integrated into emergency stroke protocols for early risk stratification and guiding management. Future research can build on this by exploring serial D-dimer measurements and developing personalized stroke management models.
Keywords:D-Dimer; Ischemic Stroke; NIHSS; Mrs; Stroke Prognosis; India
Introduction
Acute ischemic stroke (AIS) is a sudden neurological deficit
caused by focal cerebral ischemia due to arterial occlusion, leading
to brain tissue infarction [1]. It constitutes approximately 85% of
all stroke cases globally and is the second leading cause of death
worldwide responsible for approximately 6.5 million deaths and 143
million disability-adjusted life years (DALYs) globally in 2019 [2-4]. A notable shift in stroke burden has occurred toward low- and middle-income countries (LMICs), which now account for over 70%
of all stroke cases and nearly 90% of related deaths and DALYs [5,6].
In India, the incidence rate for stroke ranges between 145 and 154
per 100,000 people annually, with nearly 20% of stroke patients being
under the age of 40, highlighting a growing problem of early-onset
strokes [7,8]
Early assessment of stroke severity is crucial for predicting outcomes, triaging patients, and guiding therapeutic interventions. While clinical scales such as the NIHSS [9,10] and mRS[11-13] provide objective and validated assessments of neurological impairment and functional disability, there is ongoing research into complementary biochemical markers that can enhance prognostication and aid in rapid clinical decision-making.
D-dimer, a by-product of fibrin breakdown, indicates ongoing thrombus formation and fibrinolysis. It is produced when crosslinked fibrin is degraded by plasmin, reflecting active clot formation and breakdown. Elevated D-dimer levels are observed in various thromboembolic disorders, including deep vein thrombosis and pulmonary embolism, and have been utilized as a marker in ischemic stroke patients [13,14]. Its level correlates with stroke lesion severity, magnitude, and short- and long-term prognosis, and can also provide insights into the stroke’s etiology, with higher levels often seen in cardiogenic strokes due to fibrin-rich clots [15].
However, most of these studies have been conducted in Western populations, and data from Indian cohorts remain limited. This study aims to fill this gap by evaluating the correlation between plasma D-dimer levels and stroke severity at presentation (NIHSS) as well as functional outcome at 4 weeks (mRS) in a tertiary care center in Eastern India.
Early assessment of stroke severity is crucial for predicting outcomes, triaging patients, and guiding therapeutic interventions. While clinical scales such as the NIHSS [9,10] and mRS[11-13] provide objective and validated assessments of neurological impairment and functional disability, there is ongoing research into complementary biochemical markers that can enhance prognostication and aid in rapid clinical decision-making.
D-dimer, a by-product of fibrin breakdown, indicates ongoing thrombus formation and fibrinolysis. It is produced when crosslinked fibrin is degraded by plasmin, reflecting active clot formation and breakdown. Elevated D-dimer levels are observed in various thromboembolic disorders, including deep vein thrombosis and pulmonary embolism, and have been utilized as a marker in ischemic stroke patients [13,14]. Its level correlates with stroke lesion severity, magnitude, and short- and long-term prognosis, and can also provide insights into the stroke’s etiology, with higher levels often seen in cardiogenic strokes due to fibrin-rich clots [15].
However, most of these studies have been conducted in Western populations, and data from Indian cohorts remain limited. This study aims to fill this gap by evaluating the correlation between plasma D-dimer levels and stroke severity at presentation (NIHSS) as well as functional outcome at 4 weeks (mRS) in a tertiary care center in Eastern India.
Methods
Study Design, Setting, and Duration:This was a cross-sectional
observational study conducted in the inpatient wards and emergency
services of All India Institute of Medical Sciences (AIIMS) Patna. The
study spanned 18 months, from January 2024 to May 2025.
Study Population and Sampling:A total of 140 adult patients (≥18 years) with confirmed acute ischemic stroke, admitted within 48 hours of symptom onset, were included. Patients were recruited using non-probability purposive sampling from AIIMS Patna Emergency or In-Patient Department (IPD). The sample size of 140 was calculated to achieve 80% power with a 95% confidence interval, based on a mean D-dimer level of 457 ± 57 ng/ml in complicated AIS patients from previous research.
Inclusion Criteria:Patients aged ≥18 years with acute ischemic stroke confirmed by CT or MRI, admitted within 48 hours of symptom onset, and providing informed consent.
Study Population and Sampling:A total of 140 adult patients (≥18 years) with confirmed acute ischemic stroke, admitted within 48 hours of symptom onset, were included. Patients were recruited using non-probability purposive sampling from AIIMS Patna Emergency or In-Patient Department (IPD). The sample size of 140 was calculated to achieve 80% power with a 95% confidence interval, based on a mean D-dimer level of 457 ± 57 ng/ml in complicated AIS patients from previous research.
Inclusion Criteria:Patients aged ≥18 years with acute ischemic stroke confirmed by CT or MRI, admitted within 48 hours of symptom onset, and providing informed consent.
Exclusion Criteria:Haemorrhagic stroke on imaging, recent
surgery or trauma (within 4 weeks), known malignancy or active
infection, pre-existing coagulation disorders or ongoing anticoagulant
therapy, and thrombolysis prior to sample collection.
Data Collection:Clinical and demographic data were collected using a structured proforma. This included age, sex, time of symptom onset, and risk factors (hypertension, diabetes mellitus, atrial fibrillation, smoking, dyslipidemia). Stroke severity was assessed using the NIHSS at admission. D-dimer levels were obtained at time of admission. Functional outcome was measured using the mRS at 4 weeks via telephonic interview. Other laboratory parameters included complete blood count, renal function tests, fasting blood glucose, lipid profile, ECG, echocardiography.
D-dimer Assay:D-dimer was measured using a qualitative immunoturbidimetric method at the hospital’s central lab. Results were reported in ug/mL Fibrinogen Equivalent Units (FEU). A threshold of 0.5 ug/mL was used to categorize patients into two groups: ≤0.5 ug/mL and >0.5 ug/mL.
Outcome Measures:The primary outcome was stroke severity (NIHSS) at admission. The secondary outcome was functional outcome (mRS) at 4 weeks post-stroke.
Statistical Analysis:Data were cleaned and coded using Microsoft Excel and analyzed using Jamovi software (version 2.3.28). Qualitative variables were presented as proportions, and quantitative variables as mean ± SD or median with IQR, based on normality assessment (Shapiro-Wilk test). Chi-square test was used for associations between categorical variables (Fisher’s Exact Test for small cell counts). Independent t-test or Mann-Whitney U test compared means between two independent groups. Pearson’s or Spearman’s rank correlation coefficient (rho) assessed correlation between continuous variables. A p-value <0.05 was considered statistically significant.
Data Collection:Clinical and demographic data were collected using a structured proforma. This included age, sex, time of symptom onset, and risk factors (hypertension, diabetes mellitus, atrial fibrillation, smoking, dyslipidemia). Stroke severity was assessed using the NIHSS at admission. D-dimer levels were obtained at time of admission. Functional outcome was measured using the mRS at 4 weeks via telephonic interview. Other laboratory parameters included complete blood count, renal function tests, fasting blood glucose, lipid profile, ECG, echocardiography.
D-dimer Assay:D-dimer was measured using a qualitative immunoturbidimetric method at the hospital’s central lab. Results were reported in ug/mL Fibrinogen Equivalent Units (FEU). A threshold of 0.5 ug/mL was used to categorize patients into two groups: ≤0.5 ug/mL and >0.5 ug/mL.
Outcome Measures:The primary outcome was stroke severity (NIHSS) at admission. The secondary outcome was functional outcome (mRS) at 4 weeks post-stroke.
Statistical Analysis:Data were cleaned and coded using Microsoft Excel and analyzed using Jamovi software (version 2.3.28). Qualitative variables were presented as proportions, and quantitative variables as mean ± SD or median with IQR, based on normality assessment (Shapiro-Wilk test). Chi-square test was used for associations between categorical variables (Fisher’s Exact Test for small cell counts). Independent t-test or Mann-Whitney U test compared means between two independent groups. Pearson’s or Spearman’s rank correlation coefficient (rho) assessed correlation between continuous variables. A p-value <0.05 was considered statistically significant.
Results
A total of 140 patients with acute ischemic stroke were included.
Baseline Characteristics of the Study Population
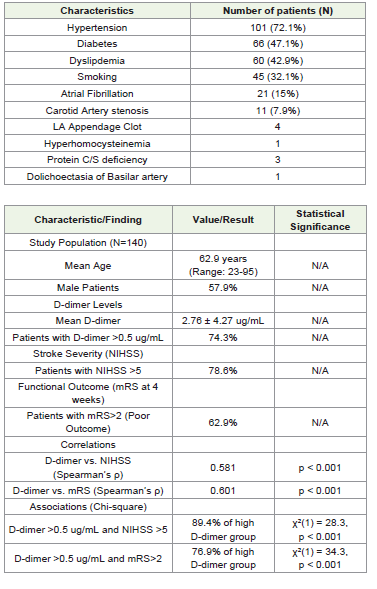
The mean age of the study population was 62.9 years (95% CI: 60.5-65.3), with a median age of 65.0 years. The age ranged from 23 to 95 years, reflecting a wide age range typical of ischemic stroke cohorts. Males constituted 57.9% (n=81) of the cohort, while females were 42.1% (n=59), indicating a male predominance consistent with epidemiological data. Hypertension was highly prevalent, affecting 72.1% (n=101) of patients, reaffirming its role as the most significant modifiable risk factor. Type 2 Diabetes Mellitus (T2DM) was present in 47.1% (n=66) of patients, highlighting its substantial burden. Dyslipidemia was found in 42.9% (n=60) of patients, and 32.1% (n=45) reported a history of smoking. Atrial Fibrillation, used as a proxy for cardioembolic etiology, was present in 15.0% (n=21) of patients. Carotid imaging was not performed in 82.9% of patients; among those imaged, 7.9% had abnormal findings (stenosis, narrowing, or occlusion), with Right Internal Carotid Artery (ICA) involvement being the most common abnormality. Rare etiologies identified included Left Atrial Appendage clot (n=4), significant pause on Holter monitoring (n=1), dolichoectasia of the basilar artery (n=1), hyperhomocysteinemia (n=1), and protein C and/or S deficiency (n=3). [Table 1] highlights all the etiologies.
Baseline Characteristics of the Study Population
The mean age of the study population was 62.9 years (95% CI: 60.5-65.3), with a median age of 65.0 years. The age ranged from 23 to 95 years, reflecting a wide age range typical of ischemic stroke cohorts. Males constituted 57.9% (n=81) of the cohort, while females were 42.1% (n=59), indicating a male predominance consistent with epidemiological data. Hypertension was highly prevalent, affecting 72.1% (n=101) of patients, reaffirming its role as the most significant modifiable risk factor. Type 2 Diabetes Mellitus (T2DM) was present in 47.1% (n=66) of patients, highlighting its substantial burden. Dyslipidemia was found in 42.9% (n=60) of patients, and 32.1% (n=45) reported a history of smoking. Atrial Fibrillation, used as a proxy for cardioembolic etiology, was present in 15.0% (n=21) of patients. Carotid imaging was not performed in 82.9% of patients; among those imaged, 7.9% had abnormal findings (stenosis, narrowing, or occlusion), with Right Internal Carotid Artery (ICA) involvement being the most common abnormality. Rare etiologies identified included Left Atrial Appendage clot (n=4), significant pause on Holter monitoring (n=1), dolichoectasia of the basilar artery (n=1), hyperhomocysteinemia (n=1), and protein C and/or S deficiency (n=3). [Table 1] highlights all the etiologies.
D-dimer Levels, NIHSS, and mRS Distribution:The mean
D-dimer level was 2.76 ± 4.27 ug/mL (median 1.08 ug/mL, range
0.00-20.0 ug/mL). The distribution was non-normal (Shapiro-Wilk
p < 0.001), indicating a right-skew. Elevated D-dimer levels (>0.5 ug/
mL) were observed in 74.3% (n=104) of patients, suggesting a strong
prevalence of thrombotic activity. At admission, 78.6% (n=110) of
patients had moderate to severe stroke (NIHSS >5), while 21.4%
(n=30) had minor strokes (NIHSS ≤5). This distribution highlights
that a significant majority presented with substantial neurological
deficits. At 28 days post-stroke, 62.9% (n=88) of patients had
poor functional outcomes (mRS>2), indicating varying degrees of
dependence, while 37.1% (n=52) achieved good recovery (mRS ≤2).
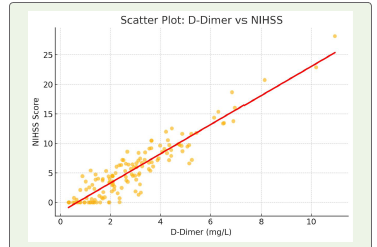
Correlation and Association Findings:A statistically significant
positive correlation was found between D-dimer levels and NIHSS
scores (Spearman’s ρ = 0.581, df = 138, p < 0.001). This indicates that
higher D-dimer levels are associated with increased stroke severity.
The scatter plot between D-dimer levels and NIHSS scores as depicted in [Figure 1] showed an upward trend, indicating that patients with higher D-dimer levels generally had higher NIHSS scores, reflecting more severe neurological deficits.
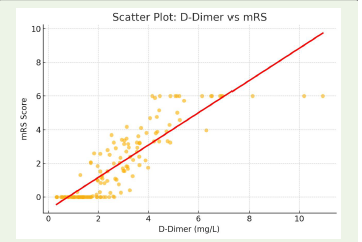
Similarly, a significant positive correlation was observed between D-dimer levels and mRS scores at 28 days (Spearman’s ρ = 0.601, df = 138, p < 0.001), suggesting that elevated D-dimer at admission correlates with greater disability at 4 weeks.
Scatter plot of D-Dimer vs mRS scores, shown in [Figure 2] demonstrating a moderate to strong positive correlation. As D-Dimer levels increase, the mRS score also tends to rise—indicating worse functional outcomes at 28 days.
The scatter plot between D-dimer levels and NIHSS scores as depicted in [Figure 1] showed an upward trend, indicating that patients with higher D-dimer levels generally had higher NIHSS scores, reflecting more severe neurological deficits.
Similarly, a significant positive correlation was observed between D-dimer levels and mRS scores at 28 days (Spearman’s ρ = 0.601, df = 138, p < 0.001), suggesting that elevated D-dimer at admission correlates with greater disability at 4 weeks.
Scatter plot of D-Dimer vs mRS scores, shown in [Figure 2] demonstrating a moderate to strong positive correlation. As D-Dimer levels increase, the mRS score also tends to rise—indicating worse functional outcomes at 28 days.
Discussion
This study investigated the correlation of plasma D-dimer levels
with stroke severity (NIHSS) and short-term functional outcome
(mRS) in 140 acute ischemic stroke patients from Eastern India. Our
findings consistently demonstrate a significant positive association
between elevated D-dimer levels and both greater initial stroke
severity and poorer functional recovery at 4 weeks.
The demographic profile of our cohort, with a mean age of 62.9 years and male predominance (57.9%), aligns with global and Indian epidemiological trends of stroke incidence [16,17]. The high prevalence of hypertension (72.1%) and Type 2 Diabetes Mellitus (47.1%) as risk factors further reinforces their established roles in stroke pathogenesis, consistent with national registries [18,19]. Atrial fibrillation, present in 15% of our patients, highlights the considerable contribution of cardioembolic sources to ischemic stroke in this region [20].
A substantial proportion of our patients (74.3%) presented with elevated D-dimer levels (>0.5 ug/mL), and 78.6% exhibited moderate to severe neurological impairment (NIHSS >5). These figures are comparable to other studies in similar settings, suggesting that activation of coagulation and fibrinolysis is a common pathophysiological response in AIS, often reflecting a higher thrombotic burden [21,22]. Nam et al. [5] and Strbian et al. [14] also reported that acute increases in D-dimer correlated significantly with infarct volume and early neurological deterioration, reinforcing its dynamic nature and potential for clinical triage.
Our study’s core finding is the strong positive correlation between D-dimer levels and NIHSS scores (ρ = 0.581, p < 0.001). This relationship suggests that higher D-dimer levels reflect a larger thrombus burden or embolic source, leading to more severe strokes. This is consistent with previous research showing that elevated D-dimer correlates with larger infarct volumes and greater NIHSS scores [15,19,22-24]. The significant association observed in chisquare analysis (89.4% of high D-dimer patients had NIHSS >5) further strengthens this link, supporting D-dimer as a surrogate marker of infarct severity. Montaner et al. [25] also found plasma biomarkers of vascular injury, including D-dimer, to be associated with stroke prognosis.
Furthermore, the significant positive correlation between D-dimer levels and 28-day mRS scores (ρ = 0.601, p < 0.001) indicates that elevated D-dimer at admission is predictive of poorer functional outcomes. This aligns with studies demonstrating that higher D-dimer levels are associated with increased functional dependence or mortality [26,27]. The chi-square analysis reinforced this, showing that 76.9% of patients with high D-dimer had poor outcomes (mRS>2), validating D-dimer’s prognostic utility for shortterm recovery. Sato et al. [24] highlighted that even minor stroke patients with large vessel occlusion and elevated D-dimer were at risk of deterioration and poor outcome, underscoring the importance of biochemical markers in complementing clinical scales like mRS. Our subgroup analysis revealed significantly higher D-dimer levels in patients with atrial fibrillation, consistent with findings from other studies [28,29]. This supports D-dimer’s diagnostic utility in identifying cardioembolic stroke subtypes, which often present with more severe deficits and necessitate specific management strategies.
The demographic profile of our cohort, with a mean age of 62.9 years and male predominance (57.9%), aligns with global and Indian epidemiological trends of stroke incidence [16,17]. The high prevalence of hypertension (72.1%) and Type 2 Diabetes Mellitus (47.1%) as risk factors further reinforces their established roles in stroke pathogenesis, consistent with national registries [18,19]. Atrial fibrillation, present in 15% of our patients, highlights the considerable contribution of cardioembolic sources to ischemic stroke in this region [20].
A substantial proportion of our patients (74.3%) presented with elevated D-dimer levels (>0.5 ug/mL), and 78.6% exhibited moderate to severe neurological impairment (NIHSS >5). These figures are comparable to other studies in similar settings, suggesting that activation of coagulation and fibrinolysis is a common pathophysiological response in AIS, often reflecting a higher thrombotic burden [21,22]. Nam et al. [5] and Strbian et al. [14] also reported that acute increases in D-dimer correlated significantly with infarct volume and early neurological deterioration, reinforcing its dynamic nature and potential for clinical triage.
Our study’s core finding is the strong positive correlation between D-dimer levels and NIHSS scores (ρ = 0.581, p < 0.001). This relationship suggests that higher D-dimer levels reflect a larger thrombus burden or embolic source, leading to more severe strokes. This is consistent with previous research showing that elevated D-dimer correlates with larger infarct volumes and greater NIHSS scores [15,19,22-24]. The significant association observed in chisquare analysis (89.4% of high D-dimer patients had NIHSS >5) further strengthens this link, supporting D-dimer as a surrogate marker of infarct severity. Montaner et al. [25] also found plasma biomarkers of vascular injury, including D-dimer, to be associated with stroke prognosis.
Furthermore, the significant positive correlation between D-dimer levels and 28-day mRS scores (ρ = 0.601, p < 0.001) indicates that elevated D-dimer at admission is predictive of poorer functional outcomes. This aligns with studies demonstrating that higher D-dimer levels are associated with increased functional dependence or mortality [26,27]. The chi-square analysis reinforced this, showing that 76.9% of patients with high D-dimer had poor outcomes (mRS>2), validating D-dimer’s prognostic utility for shortterm recovery. Sato et al. [24] highlighted that even minor stroke patients with large vessel occlusion and elevated D-dimer were at risk of deterioration and poor outcome, underscoring the importance of biochemical markers in complementing clinical scales like mRS. Our subgroup analysis revealed significantly higher D-dimer levels in patients with atrial fibrillation, consistent with findings from other studies [28,29]. This supports D-dimer’s diagnostic utility in identifying cardioembolic stroke subtypes, which often present with more severe deficits and necessitate specific management strategies.
Ramos-Pachón et al. [28] specifically demonstrated that elevated
D-dimer could reliably predict large vessel occlusion, particularly in
cardioembolic strokes.
Clinical Implications:
The findings suggest that D-dimer testing can serve as a
valuable, accessible, and cost-effective early biomarker for assessing
stroke severity and predicting short-term functional outcomes. Its
rapid turnaround makes it suitable for integration into emergency
stroke protocols alongside established clinical scales like NIHSS. In
resource-constrained settings, where immediate access to advanced
neuroimaging (like MRI or CT angiography) or neuro-specialist
input may be delayed, D-dimer could be particularly useful for early
risk stratification, helping to prioritize patients for urgent evaluation
and more aggressive treatment. Identifying patients at higher risk of
poor outcome at admission may prompt closer monitoring, and early
rehabilitation planning. Furthermore, D-dimer levels might aid in
differential diagnosis; for instance, a normal D-dimer level in a patient
with stroke-like symptoms might suggest alternative diagnoses such as
functional neurological disorders or migraine, while a highly elevated
level could alert clinicians to consider stroke mimics with thrombotic
components, like cerebral venous thrombosis or hypercoagulable
states. Ultimately, future research combining D-dimer with other
emerging biomarkers and advanced imaging parameters could lead
to the development of more integrated and personalized risk models
for comprehensive stroke management.Strengths and Limitations:
Strengths: This is one of the few cross-sectional studies in Eastern
India focusing on D-dimer in acute ischemic stroke, incorporating
both NIHSS and mRS for a comprehensive assessment of severity
and outcome. The study demonstrates a strong correlation between
D-dimer levels and stroke severity, highlighting its potential for early
identification and outcome prediction.Limitations: Being a cross-sectional study, it cannot infer causality. D-dimer elevation can occur due to non-stroke-related causes, despite efforts to exclude common confounders. The modest sample size (n=140) necessitates larger, multi-center studies for validation. Follow-up was limited to 4 weeks, leaving long-term prognostic utility unexplored. Serial D-dimer measurements, which could provide dynamic prognostic value, were not performed. Despite these limitations, the study offers important insights into D-dimer’s clinical relevance in acute ischemic stroke within the Indian context.
Conclusion
This study establishes a significant association between elevated
plasma D-dimer levels and both the severity (NIHSS) and short-term
functional outcome (mRS) of acute ischemic stroke. The strong positive
correlation observed suggests that higher D-dimer concentrations at
admission are linked to more severe neurological deficits and poorer
recovery trajectories. D-dimer, a readily available and cost-effective
biomarker, can complement clinical scales to enhance early risk
stratification, guide acute management decisions, and predict short
term outcomes, especially in resource-limited environments. Its
utility in identifying cardioembolic stroke subtypes further adds to
its diagnostic value. Future research should validate these findings in
larger cohorts, explore serial D-dimer measurements, and integrate
biomarker data into predictive models for personalized stroke care.
References
3. The top 10 causes of death [Internet] (2024) World Health Organization; 2024 [cited 2025 Jun 22].
Citation
Kumar V, Siddiqui A, Kumar S. Correlation of Plasma D-Dimer Levels with Stroke Severity and Short-Term Outcome in Patients with Acute Ischemic Stroke: A Cross-Sectional Study. Indian J Neurol. 2026;7(1): 168.