Research Article
Prevalence of Depression and Associated Factors Among Patients in the Epilepsy Monitoring Unit at King Abdullah Medical City, Makkah: A Cross-Sectional Study
Sami Saad1*, Andijani O2, Alharthi AS1, Al-Alfard HA3, Fatani B1, Alshehri T3 and Abualela HM4
1Department of Mental Health, King Abdullah Medical City, Makkah, Kingdom of Saudi Arabia.
2Department of Ministry Health and Preventive Medicine, Jeddah, Kingdom of Saudi Arabia
3Department of Ministry Health and Psychiatry, Abha, Kingdom of Saudi Arabi
4Department of Neuroscience Center, Neurology, King Abdullah Medical City, Makkah, Kingdom of Saudi Arabia
2Department of Ministry Health and Preventive Medicine, Jeddah, Kingdom of Saudi Arabia
3Department of Ministry Health and Psychiatry, Abha, Kingdom of Saudi Arabi
4Department of Neuroscience Center, Neurology, King Abdullah Medical City, Makkah, Kingdom of Saudi Arabia
*Corresponding author:Sami Saad, Department of Mental Health, King Abdullah Medical City, Makkah, Kingdom of Saudi Arabia. E-mail Id: sami_yahya@hotmail.com
Article Information:Submission: 02/04/2026; Accepted: 18/04/2026; Published: 20/04/2026
Copyright: ©2026 Saad S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Epilepsy is a chronic neurological disorder frequently associated with psychiatric comorbidities, particularly depression, which significantly impairs quality of life (QOL). Limited data exist regarding its prevalence and associated factors in tertiary care settings, specifically within Epilepsy Monitoring Units (EMUs), in the Kingdom of Saudi Arabia (KSA).
Objective: To determine the prevalence of depression and identify associated factors among patients admitted to the Epilepsy Monitoring Unit (EMU) at King Abdullah Medical City (KAMC) Specialist Hospital, Makkah, KSA.
Methods: A cross-sectional study was conducted from January 2024 to August 2025, enrolling adult patients with a confirmed epilepsy diagnosis admitted to the Epilepsy Monitoring Unit. Data were collected using structured questionnaires including demographic and clinical variables such as the Neurological Disorders Depression Inventory for Epilepsy (NDDI-E), and the Oslo Social Support Scale (OSSS-3). Associations were examined using chisquare and non-parametric tests due to the non-normal distribution of variables, followed by multivariable logistic regression. A p-value <0.05 was considered to determine statistical significance.
Results: Among 68 participants admitted to the EMU, the prevalence of depression was 35.3% (95% CI: 25.0% to 47.2%). Higher seizure frequency (>5 seizures/year) and lower educational level showed trends toward increased depression risk. No other factors reached statistical significance.
Conclusion: Depression affects nearly one-third of patients admitted for monitoring in the EMU at KAMC Makkah, KSA. Routine screening and integrated neuropsychiatric care within the EMU setting are essential to improve overall outcomes and QOL among epilepsy patients.
Objective: To determine the prevalence of depression and identify associated factors among patients admitted to the Epilepsy Monitoring Unit (EMU) at King Abdullah Medical City (KAMC) Specialist Hospital, Makkah, KSA.
Methods: A cross-sectional study was conducted from January 2024 to August 2025, enrolling adult patients with a confirmed epilepsy diagnosis admitted to the Epilepsy Monitoring Unit. Data were collected using structured questionnaires including demographic and clinical variables such as the Neurological Disorders Depression Inventory for Epilepsy (NDDI-E), and the Oslo Social Support Scale (OSSS-3). Associations were examined using chisquare and non-parametric tests due to the non-normal distribution of variables, followed by multivariable logistic regression. A p-value <0.05 was considered to determine statistical significance.
Results: Among 68 participants admitted to the EMU, the prevalence of depression was 35.3% (95% CI: 25.0% to 47.2%). Higher seizure frequency (>5 seizures/year) and lower educational level showed trends toward increased depression risk. No other factors reached statistical significance.
Conclusion: Depression affects nearly one-third of patients admitted for monitoring in the EMU at KAMC Makkah, KSA. Routine screening and integrated neuropsychiatric care within the EMU setting are essential to improve overall outcomes and QOL among epilepsy patients.
Keywords:Antiepileptic drugs; Depression; Epilepsy; NDDI-E; ESS. OSSS-3; EMU
Introduction
Epilepsy is a chronic neurological disorder characterized by
recurrent seizures affecting individuals of all ages worldwide.
Beyond the physical and cognitive impacts of epilepsy, there is
growing recognition of the significant burden of mental health
disorders experienced by individuals with epilepsy [1,2]. Among
these, depression stands out as a prevalent and contributing factor to
reduced quality of life (QOL) and increased morbidity [3,4].
Depression is a serious mental health disorder associated with persistent feelings of sadness, hopelessness, and a loss of interest or pleasure in activities. It can profoundly affect an individual’s emotional well-being, daily functioning, and overall health. Evidence suggests that patients with epilepsy have a higher risk of developing depression compared to the general population [5]. This association between epilepsy and depression is complex, with a bidirectional relationship between these two conditions [6].
Despite the recognized significance of depression among individuals with epilepsy, there remains a paucity of research investigating the prevalence and associated factors specifically within tertiary care settings such as KAMC [7]. In the literature, it is reported that 39% of participants with epilepsy reported clinically defined depressive symptoms, which is assessed by a reliable self-report index of mood such as Beck Depression Inventory-II (BDI-II) [8].
The Epilepsy Monitoring Unit (EMU) is a specialized inpatient setting where patients with refractory epilepsy undergo continuous video-EEG monitoring for seizure characterization and presurgical evaluation. Admission involves gradual withdrawal of antiseizure medications to provoke seizures, creating a uniquely stressful period marked by seizure anticipation and anxiety. The EMU, therefore offers a critical opportunity to assess the psychological burden of epilepsy, particularly depression, during a time of active seizure evaluation and heightened vulnerability.
A prospective EMU study [4] found that depression was the only independent predictor of quality of life in patients with refractory epilepsy, surpassing seizure burden. Depression affected 54% of patients, and the authors concluded that depression management is often inadequately prioritized compared to seizure reduction in intractable epilepsy. Another study in EMU [9] found that 40% of EMU patients had depression. One of the largest studies examining the prevalence of depression in EMU, among 395 epilepsy patients admitted to the EMU, found that 45.6% had depression [10].
To the best of our knowledge, no study has been done in Saudi Arabia about the prevalence of depression among EMU patients specifically. A large cross-sectional study across the four geographical regions of Saudi Arabia reported that depressive symptoms were prevalent in 84.7% of participants with epilepsy, with a higher prevalence noted among younger individuals [11]. In a 2016 study conducted in Taif, a very high rate of depressive indications (89%) was found among adolescents with epilepsy aged 12 to 18 years [12] Broader studies across different age groups also report substantial prevalence. A national study found that a significant majority (73.7%) of PWE suffered from chronic depression lasting more than a year [13]. More recently, a study at a tertiary care hospital in Riyadh found that nearly half (48.25%) of the 400 participants exhibited depression, which was significantly associated with lower educational level, unemployment, longer epilepsy duration, and poorer quality of life [14]. Collectively, these findings underscore the high variability and critical need for routine screening and integrated care for depression in this patient population across the Kingdom.
Establishing the magnitude and determinants of depression in this population is crucial for informing evidence-based clinical practice. Identifying patients at higher risk enables healthcare professionals to implement early screening strategies and design integrated care models that simultaneously address neurological and mental health needs. A clearer understanding of these associations supports the development of targeted interventions, optimizes comprehensive epilepsy management, and ultimately contributes to improved treatment outcomes along with QOL.
Depression is a serious mental health disorder associated with persistent feelings of sadness, hopelessness, and a loss of interest or pleasure in activities. It can profoundly affect an individual’s emotional well-being, daily functioning, and overall health. Evidence suggests that patients with epilepsy have a higher risk of developing depression compared to the general population [5]. This association between epilepsy and depression is complex, with a bidirectional relationship between these two conditions [6].
Despite the recognized significance of depression among individuals with epilepsy, there remains a paucity of research investigating the prevalence and associated factors specifically within tertiary care settings such as KAMC [7]. In the literature, it is reported that 39% of participants with epilepsy reported clinically defined depressive symptoms, which is assessed by a reliable self-report index of mood such as Beck Depression Inventory-II (BDI-II) [8].
The Epilepsy Monitoring Unit (EMU) is a specialized inpatient setting where patients with refractory epilepsy undergo continuous video-EEG monitoring for seizure characterization and presurgical evaluation. Admission involves gradual withdrawal of antiseizure medications to provoke seizures, creating a uniquely stressful period marked by seizure anticipation and anxiety. The EMU, therefore offers a critical opportunity to assess the psychological burden of epilepsy, particularly depression, during a time of active seizure evaluation and heightened vulnerability.
A prospective EMU study [4] found that depression was the only independent predictor of quality of life in patients with refractory epilepsy, surpassing seizure burden. Depression affected 54% of patients, and the authors concluded that depression management is often inadequately prioritized compared to seizure reduction in intractable epilepsy. Another study in EMU [9] found that 40% of EMU patients had depression. One of the largest studies examining the prevalence of depression in EMU, among 395 epilepsy patients admitted to the EMU, found that 45.6% had depression [10].
To the best of our knowledge, no study has been done in Saudi Arabia about the prevalence of depression among EMU patients specifically. A large cross-sectional study across the four geographical regions of Saudi Arabia reported that depressive symptoms were prevalent in 84.7% of participants with epilepsy, with a higher prevalence noted among younger individuals [11]. In a 2016 study conducted in Taif, a very high rate of depressive indications (89%) was found among adolescents with epilepsy aged 12 to 18 years [12] Broader studies across different age groups also report substantial prevalence. A national study found that a significant majority (73.7%) of PWE suffered from chronic depression lasting more than a year [13]. More recently, a study at a tertiary care hospital in Riyadh found that nearly half (48.25%) of the 400 participants exhibited depression, which was significantly associated with lower educational level, unemployment, longer epilepsy duration, and poorer quality of life [14]. Collectively, these findings underscore the high variability and critical need for routine screening and integrated care for depression in this patient population across the Kingdom.
Establishing the magnitude and determinants of depression in this population is crucial for informing evidence-based clinical practice. Identifying patients at higher risk enables healthcare professionals to implement early screening strategies and design integrated care models that simultaneously address neurological and mental health needs. A clearer understanding of these associations supports the development of targeted interventions, optimizes comprehensive epilepsy management, and ultimately contributes to improved treatment outcomes along with QOL.
Methodology
Study Design, Duration and Setting:
The cross-sectional study was conducted in January 2024 to
August 2025. The study was conducted in King Abdullah Medical
City Specialist Hospital (KAMC), Makkah, KSA, which is a tertiary
and quaternary healthcare facility and a not-for-profit hospital.Study Population:
Adult epilepsy patients admitted to the Epilepsy Monitoring
Units (EMU) at KAMC were enrolled.Sampling Technique and Sample Size:
A simple random sampling technique was used to minimize
selection bias. The required sample size was calculated using Raosoft
sample size calculator, assuming a 5% margin of error, 95% confidence
level, reference population of 108 patients based on hospital records,
and an assumed response distribution of 50%. A total of 85 patients
were enrolled; however, 68 were included in the final analysis after
excluding 19 patients diagnosed with Psychogenic Non-Epileptic
Seizures (PNES) and one patient who did not complete one of the
scales. Although the final sample size was smaller than the initially
calculated sample, it was considered adequate for the planned
descriptive and comparative statistical analyses.Eligibility Criteria:
All adult patients (>18 years) diagnosed with epilepsy through
electroencephalography (EEG) and who provided informed consent
were included. The exclusion criteria were that patients who refused
to participate in the study and were younger than 18 years of age.Data Collection Tools:
Data were collected from patients with a confirmed diagnosis of
epilepsy admitted to the Epilepsy Monitoring Unit (EMU) at King
Abdullah Medical City (KAMC), Saudi Arabia. Eligible participants
who provided verbal informed consent completed a structured
questionnaire consisting of two sections. The first section collected
participants’ demographic information. The second section included
two validated scales (Appendix I). The Neurological Disorders
Depression Inventory for Epilepsy (NDDI-E) [15] is a 6-item
questionnaire used for rapid identification of major depressive
disorder among patients with epilepsy. The Arabic version of the
NDDI-E has been previously translated and validated [16]. The
second scale is the Oslo Social Support Scale (OSSS-3), which is also
used to assess perceived social support [17]. This scale comprises three
items that assess the level of social support the participant receives.Measurements:
Depression was assessed using the Neurological Disorders
Depression Inventory for Epilepsy (NDDI-E). Item responses were
summed to generate a total score ranging from 6 to 24, with higher
scores indicating greater severity of depressive symptoms. A cutoff
score of >13 was used to classify participants as screening positive
for depression. Prior to the main data collection, a pilot study was
conducted on 10 patients to assess the clarity and reliability of the
study instruments. Based on the pilot data, the NDDI-E demonstrated
good internal consistency (Cronbach’s α = 0.780). Perceived social
support was measured using the Oslo Social Support Scale (OSSS-
3). The sum score ranges from 3 to 14, with higher scores indicating
stronger perceived social support. Scores were categorized as poor
support [3-8], moderate support [9-11], and strong support
[12-14]. Based on the pilot study data, the OSSS-3 demonstrated acceptable
internal consistency in this sample (Cronbach’s α = 0.647).Statistical Analysis Plan:
Data were analyzed using R software (version 4.4.1). Descriptive
statistics were used to summarize participants’ sociodemographic
and clinical characteristics. Continuous variables were assessed
for normality using the Shapiro–Wilk test. Normally distributed
variables were reported as mean ± standard deviation (SD), while
non-normally distributed variables were presented as median and
interquartile range (IQR). Categorical variables were summarized
as frequencies and percentages. The prevalence of depression was
estimated with 95% confidence intervals (CIs). Univariate analyses
were conducted to examine associations between depression status
and potential predictors. Categorical variables were compared using
the chi-square test or Fisher’s exact test as appropriate. Continuous
variables were compared using the independent t-test if normally
distributed; otherwise, the Wilcoxon rank-sum test (for two groups)
or the Kruskal–Wallis test (for more than two groups) was applied.
A multivariable logistic regression model was used to identify
factors independently associated with depression. Age and gender
were included in the model a priori as key demographic covariates.
Additional candidate predictors were selected based on univariable
screening (p < 0.20) and entered into the multivariable model. Results
were reported as adjusted odds ratios (aORs) with 95% confidence
intervals and corresponding p-values. A two-sided p-value < 0.05 was
considered statistically significant.Ethical Considerations:
Ethical approval was sought from KAMC IRB 23.1200. No study
activities were initiated until IRB approval was obtained. The purpose
and nature of the study were explained to all patients along with a
brief information sheet describing the study’s purpose and its steps.
It was emphasized that participation was voluntary, and they had the
right to leave the study at any time to ensure autonomy. A serial No.
was given to each participant to de-identify the patient.Results
Participant characteristics and prevalence of depression:
A total of 69 patients were enrolled in the study. Complete
data were available for all participants; however, one patient did
not complete the NDDI-E questionnaire, leaving 68 patients with
evaluable depression status, among whom 24 met the NDDI-E cutoff
for depression, yielding a depression prevalence of 35.3% (95% CI:
25.0%-47.2%).As shown in [Table 1] participants were predominantly female (58.0%) and most were aged 30-40 years (40.6%). Over half were married (53.6%), and 52.2% had a high school/diploma education. Most participants were unemployed (76.8%) and reported an
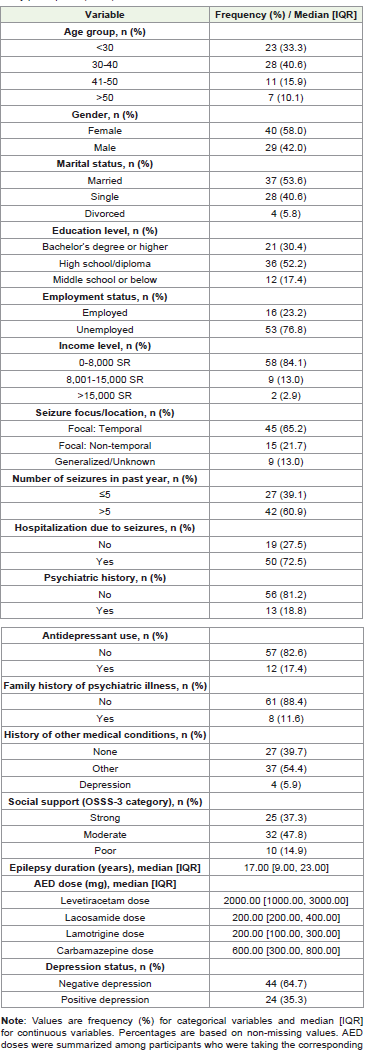
income of less than 8,000 SR (84.1%). Regarding epilepsy-related
characteristics, 65.2% had focal temporal seizures, 60.9% reported
more than 5 seizures in the past year, and 72.5% had a history of
hospitalization due to seizures. The median epilepsy duration was 17.0
years (IQR: 9.0-23.0). Social support was most commonly moderate
(47.8%), followed by strong (37.3%) and poor (14.9%).
Univariable comparisons by depression status:
[Table 2] summarized univariable comparisons by depression
status. No statistically significant associations were observed between
depression status and age group, marital status, employment status,
income, seizure frequency in the past year, seizure focus/location,
hospitalization due to seizures, psychiatric history, history of other
medical conditions, social support category, epilepsy duration,
or antiepileptic drug doses (all p>0.05). Education level showed a
non-significant association with depression status (p=0.187), with
a higher proportion of depression among participants with middle
school or below education (29.2% vs. 11.4% in the non-depression
group). Family history of psychiatric illness also demonstrated a nonsignificant
trend (p=0.120), with a larger proportion of depressed
participants having family history (20.8% vs. 6.8%). Gender showed a
non-significant trend (p=0.126), with a higher proportion of females
in the depression group (70.8% vs. 50.0%).Multivariable logistic regression:
[Table 3] presents the results of the multivariable logistic
regression model. Age group and gender were included a priori, and
additional covariates were included based on univariable screening
(p<0.20). After adjustment, none of the covariates were statistically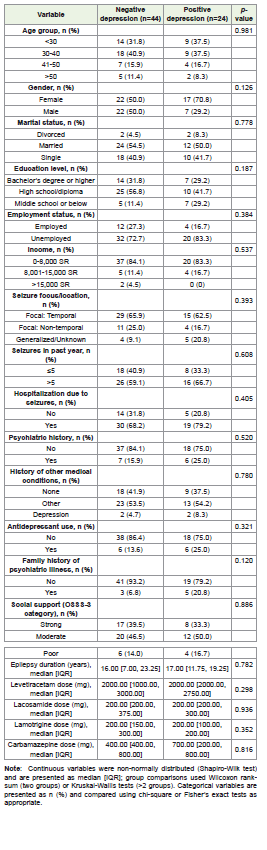
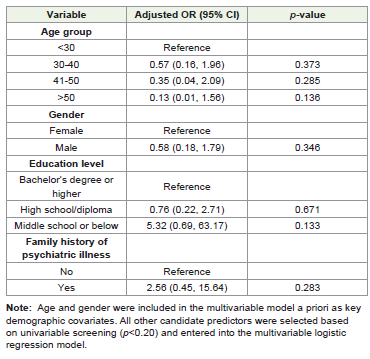
significantly associated with depression (all p>0.05). Several factors
showed suggestive trends toward higher or lower odds of depression.
Participants aged over 50 years old had relatively lower odds of
depression compared with those younger than 30 years old (a
OR=0.13, 95% CI 0.01 to 1.56; p=0.136). Compared to participants
with a bachelor’s degree or higher, those with middle school or below
education had higher odds of depression (a OR=5.32, 95% CI 0.69 to
63.17; p=0.133), although the confidence interval was wide.
Discussion
According to the NDDI-E scale, EMU patients with epilepsy
had a depression prevalence of 35.3% (95% CI: 25.0% to 47.2%) in
this cross-sectional study at KAMC, KSA. This study demonstrates
that patients with epilepsy experience depression as a significant
psychiatric comorbidity.
These findings align with current global data. Depending on screening methods and demographics, a 2020 meta-analysis by Yang Y et al. found that pooled depression prevalence rates among epileptic patients ranged from 27% to 34% [7]. Similarly, Vacca M et al. (2022) reported clinically significant depressive symptoms in 39% of patients attending a tertiary epilepsy facility [8]. Siddiqui et al. (2009), using the Hospital Anxiety and Depression Scale (HADS) in an EMU setting, found that 40% of patients had depression. Notably, they reported no significant associations between depression and clinical variables such as epilepsy type, age, sex, duration of epilepsy, seizure localization, MRI findings, or antiepileptic drugs [9]. Rocamora et al. (2021) conducted a large study on 395 patients with epilepsy admitted to an EMU. They assessed depressive symptoms using both the Beck Depression Inventory-II (BDI-II) and the (HADS-D) subscale. The study found that 45.57% of patients exhibited depression according to the BDI-II, and 30.9% according to the HADS-D. Aligning with our study, females had significantly higher BDI-II scores compared to males [18]. The study also highlighted that psychiatric symptoms were more severe when psychogenic non-epileptic seizures (PNES) coexisted with epilepsy. Differences in sample size, cultural background, healthcare access, and screening thresholds may account for our marginally lower prevalence. Overall, the prevalence in our observational cohort aligns with global and regional data, supporting the external validity of our findings.
These findings align with current global data. Depending on screening methods and demographics, a 2020 meta-analysis by Yang Y et al. found that pooled depression prevalence rates among epileptic patients ranged from 27% to 34% [7]. Similarly, Vacca M et al. (2022) reported clinically significant depressive symptoms in 39% of patients attending a tertiary epilepsy facility [8]. Siddiqui et al. (2009), using the Hospital Anxiety and Depression Scale (HADS) in an EMU setting, found that 40% of patients had depression. Notably, they reported no significant associations between depression and clinical variables such as epilepsy type, age, sex, duration of epilepsy, seizure localization, MRI findings, or antiepileptic drugs [9]. Rocamora et al. (2021) conducted a large study on 395 patients with epilepsy admitted to an EMU. They assessed depressive symptoms using both the Beck Depression Inventory-II (BDI-II) and the (HADS-D) subscale. The study found that 45.57% of patients exhibited depression according to the BDI-II, and 30.9% according to the HADS-D. Aligning with our study, females had significantly higher BDI-II scores compared to males [18]. The study also highlighted that psychiatric symptoms were more severe when psychogenic non-epileptic seizures (PNES) coexisted with epilepsy. Differences in sample size, cultural background, healthcare access, and screening thresholds may account for our marginally lower prevalence. Overall, the prevalence in our observational cohort aligns with global and regional data, supporting the external validity of our findings.
Consistent with previous research, there was a trend toward
higher seizure frequency being associated with depression, although
this did not reach statistical significance in our sample. Higher seizure
frequency dramatically raises the incidence of depressive symptoms
according to a meta-analysis with odds ratios ranging from 2.0 to
3.5 [7]. Despite having large confidence intervals, patients with less
than a middle school education had higher risks of depression. This
is consistent with research found that depression was substantially
correlated with lower educational status [19]. Reduced education may
increase psychological vulnerability by limiting health literacy, coping
strategies and socioeconomic prospects [19]. Another potential
consideration is the presence of other medical comorbidities, which
may act as confounding factors in the relationship between epilepsy
and depressive symptoms. Although history of other medical
conditions was not significantly associated with depression in our
sample, the coexistence of chronic illnesses may still contribute to
psychological burden through reduced functional status, medication
load, and perceived health limitations. The lack of statistical
significance in our study may be related to the limited sample size
and heterogeneity of the reported medical conditions.
Although depressive patients were more likely to have poor social
support this difference was not statistically significant. Nonetheless
social support is regularly found to be protective in the literature.
Strong associations between depressive symptoms and low support
are shown by OSSS-3 standardization tests [17] social isolation in
KSA may be somewhat mitigated by cultural and familial systems
which could weaken statistical correlations.
There were no discernible links found between depression and AED dosages. Nonetheless, earlier studies have indicated that some drugs (such clonazepam) could cause mood swings in vulnerable [20] or Levetiracetam may cause significant psychiatric symptoms [21]. These findings highlight the need for more extensive pharmacovigilance focused research as they neither support nor contradict these correlations.
There were no discernible links found between depression and AED dosages. Nonetheless, earlier studies have indicated that some drugs (such clonazepam) could cause mood swings in vulnerable [20] or Levetiracetam may cause significant psychiatric symptoms [21]. These findings highlight the need for more extensive pharmacovigilance focused research as they neither support nor contradict these correlations.
Implication of Findings:
There are various ramifications to the assessment that depression
affects almost one in three epileptic patients in Makkah, KSA. Early
detection may be enhanced in neurology clinics by implementing
proven instruments like the NDDI-E. Patients who have more
frequent seizures and have less education should need a more
thorough psychiatric evaluation. Important epidemiological evidence
supporting structured mental health care in tertiary epilepsy centers
is provided by this study.Strengths of findings:
This study has a number of noteworthy advantages. To
improve the reliability and comparability of the results it first used
internationally recognized and established assessment instruments
such as the Oslo Social Support Scale (OSSS-3) and the Neurological
Disorders Depression Inventory for Epilepsy (NDDI-E). Second, a
more thorough representation of people with epilepsy across various
clinical severity within the EMU setting. Lastly, by concentrating on
King Abdullah Medical City Specialist Hospital, a tertiary care facility
in Makkah, the study fills a significant research gap in the region and
offers useful epidemiological data from Saudi Arabia where there is
little published data on depression in epileptic patients.Limitations:
There are various limitations of this study. Initially, the statistical
power was limited by the smaller analytical sample size, which made
it harder to identify meaningful correlations between depression and
other risk variables. The temporal relationships cannot be established
due to the cross-sectional design as it is impossible to identify whether
depression arose as a result of or before epilepsy. The accuracy of
diagnosing depression may be limited by the fact that the Neurological
Disorders Depression Inventory for Epilepsy (NDDI-E) is a validated
and commonly used screening tool but it is still only a screening
tool and cannot replace structured psychiatric diagnostic interviews
based on standardized criteria. In addition, other coexisting medical
conditions were recorded as broad categories rather than specific
diagnoses, which may have limited the ability to fully assess their
potential confounding effect on depressive symptoms. An additional
limitation is that the depression scales were administered without
accounting for the timing of the participants’ most recent seizure,
which may have influenced the scores.Future Recommendations:
Multicenter longitudinal studies throughout KSA should be the
main focus of future research in order to improve generalizability
and determine the temporal correlations between depression and
epilepsy. Beyond screening methods, the use of structured mental
diagnostic interviews based on DSM-5 criteria would increase
diagnostic accuracy and enable more accurate estimation of the
prevalence of depression. Clarifying underlying pathophysiological
processes may be aided by additional research into putative biological
indicators such as neuroinflammatory, neurochemical and genetic
factors that connect epilepsy and depression. Such comprehensive
approaches would improve the body of evidence and direct the
creation of focused culturally relevant therapies.Conclusion
The cross-sectional study conducted at KAMC Makkah KSA
demonstrates that depression is a highly prevalent psychiatric
comorbidity among patients with epilepsy underscoring structured
psychiatric diagnostic interviews within tertiary care settings.
Although multivariable analysis did not identify statistically
significant independent predictors, clinically meaningful trends were
observed. Lower educational attainment and higher seizure frequency
appeared to be associated with increased depressive symptoms.
The results emphasize the importance of implementing integrated neuropsychiatric care models within epilepsy clinics including routine depression screening using validated assessment tools. Addressing depression as a core component of comprehensive epilepsy management is essential to enhance treatment adherence, optimize seizure control and improve overall quality of life. Future multicenter and longitudinal studies across Saudi Arabia are recommended to clarify potential causal pathways and to inform the development of culturally appropriate targeted mental health interventions for patients living with epilepsy. Such studies should also examine specific medical comorbidities as potential confounding factors influencing depressive symptoms in patients with epilepsy.
The results emphasize the importance of implementing integrated neuropsychiatric care models within epilepsy clinics including routine depression screening using validated assessment tools. Addressing depression as a core component of comprehensive epilepsy management is essential to enhance treatment adherence, optimize seizure control and improve overall quality of life. Future multicenter and longitudinal studies across Saudi Arabia are recommended to clarify potential causal pathways and to inform the development of culturally appropriate targeted mental health interventions for patients living with epilepsy. Such studies should also examine specific medical comorbidities as potential confounding factors influencing depressive symptoms in patients with epilepsy.
References
Citation
Saad S, Andijani O, Alharthi AS, Al-Alfard HA, Fatani B, et al. Prevalence of Depression and Associated Factors Among Patients in the Epilepsy Monitoring Unit at King Abdullah Medical City, Makkah: A Cross-Sectional Study. Indian J Neurol. 2026;7(1): 165.