Research Article
The Potential Benefits of Functional Electrical Stimulation (FES) Particularly for Spastic Diplegia CP in Children- Recent Advancement and Interventions
Borah AK* and Goswami P
Department of Physiotherapy, Mahatma Gandhi University, Ri-Bhoi Meghalaya, India.
*Corresponding author:Arup Kumar Borah, Department of Physiotherapy, Mahatma Gandhi University, Ri-Bhoi Meghalaya, India. E-mail Id: barup614@gmail.com
Article Information: Submission: 25/10/2025; Accepted: 20/11/2025; Published: 22/11/2025
Copyright: © 2025 Borah AK, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Cerebral palsy is a disorder characterized by abnormal tone, posture and movement clinically classified based on the predominant motor syndrome−spastic diplegia, spastic hemiplegia, spastic quadriplegia and extrapyramidal or dyskinetic. On the other hand, the incidence of CP is 2 to 3 per, 1000 live births. Prematurity and low birth weight are important risk factors for CP, however multiple other factors have been associated with an increased risk for
CP, including maternal infections, and multiple gestation. In most cases in CP the initial injury to the brain occurs during early-fetal–brain development, intracerebral hemorrhage and periventicul at leukomalacia are the main pathologic findings found in preterm infants who develop CP. Moreover, the diagnosis of CP is primarily based on clinical findings. Early diagnosis is possible based on a combination of clinical history, use of standardized neuromotor assessment and findings on magnetic resonance imaging, however, in most clinical setting CP are more reliably recognized by 2 years age. MRI scan is indicated to delineate the extent of brain lesions and to identify congenital brain malformations.
Children and young people with neurological conditions can also benefit from ‘FES treatment’ but there is gap in clinical knowledge, awareness and evidence which needs addressing. Some of the known benefits of FES include safe walking with facilitation and exercise of normal movement, muscle strengthening, joint range and proprioceptive improvements as well as spasticity reduction. FES is considered an affordable, secure, and effective treatment for assisting patients to reach their rehabilitation objectives. Given that their neurological disabilities affect muscle activation and learning of movement, children with CP.
Aim: The aim of the present study was to assess the effectiveness of functional electrical stimulation in upper limb rehabilitation (U L Rehab) in children with cerebral palsy. Moreover, this article aims to share our clinical experience in using FES for children in spastic diplegia with CP to assist in addressing this knowledge gap.
Methods:168 children with spastic cerebral palsy age between 4 years to 18 years old were randomized into 2 groups. On the other hand, 45 children represented the control group, performed conventional physical therapy. In addition to the control group, the experimental group received functional electrical stimulation interventions with postural control on the affected upper-limb.
Objective: To investigate the effectiveness of functional electrical stimulation (FES) to improve upper limb function in children with spastic diplegia of CP in children.
To assess the effect of FES on upper limb (UL) function in children with spastic diplegia of CP at six months post-intervention.
Children and young people with neurological conditions can also benefit from ‘FES treatment’ but there is gap in clinical knowledge, awareness and evidence which needs addressing. Some of the known benefits of FES include safe walking with facilitation and exercise of normal movement, muscle strengthening, joint range and proprioceptive improvements as well as spasticity reduction. FES is considered an affordable, secure, and effective treatment for assisting patients to reach their rehabilitation objectives. Given that their neurological disabilities affect muscle activation and learning of movement, children with CP.
Aim: The aim of the present study was to assess the effectiveness of functional electrical stimulation in upper limb rehabilitation (U L Rehab) in children with cerebral palsy. Moreover, this article aims to share our clinical experience in using FES for children in spastic diplegia with CP to assist in addressing this knowledge gap.
Methods:168 children with spastic cerebral palsy age between 4 years to 18 years old were randomized into 2 groups. On the other hand, 45 children represented the control group, performed conventional physical therapy. In addition to the control group, the experimental group received functional electrical stimulation interventions with postural control on the affected upper-limb.
Objective: To investigate the effectiveness of functional electrical stimulation (FES) to improve upper limb function in children with spastic diplegia of CP in children.
To assess the effect of FES on upper limb (UL) function in children with spastic diplegia of CP at six months post-intervention.
Clinical consideration for applying FES to children: There are important challenges when providing FES for children compared to adults. Moreover, the developmental stages of the neurological system, its neuroplasticity and the lack of learned function are the main difference. More frequent FES reviews are necessary due to constant growth and neuro-developmental changes. Children with CP require education of an activity or function they may not have ever experienced or felt. They lack understanding of normal movement patterns which their peers will have.
Methodology: Design and Study setting: 40 children with spastic cerebral palsy, age between 4 to 18 years old, were randomized into 2 groups. 45 children represented the control group, performed conventional physiotherapy treatment. This study employed a prospective pre/post-test, follow-up design in Spinal Life Physiotherapy Clinic www.spinallife.in . All participants received up to 40 FES therapy session applied to the spastic diplegia CP children in UL. Assessment was made at pretest (i.e before FES), and post-test (within one week after completion of the last therapy session) and follow-up (six months after the intervention period had ended).
The study was registered with ClinicalTrial.gov (OMB No. 0925-0586). Moreover, written informed assent /consent was obtained from all participants/ parents.
Results: Participant recruitment target was not met but adherence was high, and functional electrical stimulation was found to be safe and comfortable. Of the three participants, two of them improved in grasp at post-test, whereas one child’s ability deteriorated. Only one child met success criteria on most outcomes at post-test.
Discussion and Conclusion: The study concluded and emphasis, that functional electrical stimulation intervention was found to be an effective manner to improve motor performance, in terms of coordination, range of motion, three-fingered grasp strength, visibly reducing functional-limitation and improving performance in activities of daily living (ADL). Moreover, the results suggest that FES is effective in increasing impulse during walking but not in decreasing stiffness. The effect on increasing impulse does not result in more typical spatiotemporal gait parameters.
A future case comparison investigation with a larger but more selected sample is suggested.
FES offers promising potential as an adjunct therapy to complement existing treatments for upper limb dysfunction in children with spastic diplegic CP (SCP). Current evidence suggests it can improve a range of motor functions, but more research is necessary to refine treatment protocols and confirm its efficacy across different populations and settings. Evidence Based Treatment Approach: Any approach which is evidence based might be more attractive in the society.
Scientific-novelty: In this study it synthesizes updated evidence regarding lower limb functional electrical stimulation parameters and patient characteristics. Moreover, it also discusses emerging trends in individualized and home based application.
Methodology: Design and Study setting: 40 children with spastic cerebral palsy, age between 4 to 18 years old, were randomized into 2 groups. 45 children represented the control group, performed conventional physiotherapy treatment. This study employed a prospective pre/post-test, follow-up design in Spinal Life Physiotherapy Clinic www.spinallife.in . All participants received up to 40 FES therapy session applied to the spastic diplegia CP children in UL. Assessment was made at pretest (i.e before FES), and post-test (within one week after completion of the last therapy session) and follow-up (six months after the intervention period had ended).
The study was registered with ClinicalTrial.gov (OMB No. 0925-0586). Moreover, written informed assent /consent was obtained from all participants/ parents.
Results: Participant recruitment target was not met but adherence was high, and functional electrical stimulation was found to be safe and comfortable. Of the three participants, two of them improved in grasp at post-test, whereas one child’s ability deteriorated. Only one child met success criteria on most outcomes at post-test.
Discussion and Conclusion: The study concluded and emphasis, that functional electrical stimulation intervention was found to be an effective manner to improve motor performance, in terms of coordination, range of motion, three-fingered grasp strength, visibly reducing functional-limitation and improving performance in activities of daily living (ADL). Moreover, the results suggest that FES is effective in increasing impulse during walking but not in decreasing stiffness. The effect on increasing impulse does not result in more typical spatiotemporal gait parameters.
A future case comparison investigation with a larger but more selected sample is suggested.
FES offers promising potential as an adjunct therapy to complement existing treatments for upper limb dysfunction in children with spastic diplegic CP (SCP). Current evidence suggests it can improve a range of motor functions, but more research is necessary to refine treatment protocols and confirm its efficacy across different populations and settings. Evidence Based Treatment Approach: Any approach which is evidence based might be more attractive in the society.
Scientific-novelty: In this study it synthesizes updated evidence regarding lower limb functional electrical stimulation parameters and patient characteristics. Moreover, it also discusses emerging trends in individualized and home based application.
Keywords:Cerebral Palsy; Functional Electrical Stimulation; Manual Ability Classification System Spastic Diplegia Of CP; GMFCS.
Introduction
The evidence-based approach to upper limb functional electrical
stimulation for children with spastic cerebral palsy involves applying
FES to improve range of motion, muscle strength and voluntary
control, and it is most effective when combined with other goal
oriented and functional therapies. Evidence suggests that FES can
lead benefits like improved grasping function, reduced spasticity
and better movement timing. While more large-scale, long term
studies are needed, the current evidence supports FES as a beneficial
and affordable rehabilitation tool, especially when integrated into a
comprehensive treatment plan.
FES is clinically available since 2017 in Spinal Life Physiotherapy
Clinic, Six Mile Jayanagar Road, Guwahati, India (www.spinallife.
in) as a treatment option for people with Multiple sclerosis, Stroke
(CVA), incomplete spinal cord injury (ISCI), traumatic brain injury
(TBI) and adult cerebral palsy (CP) being the major cohorts. Over
the last 5 years the service has been accepting children with variety
neurological conditions for FES treatment. The service has received
350 pediatric referrals including 210 children with CP. Currently 50
children with CP are receiving treatment using FES device making
this the pediatrics FES service in the clinic.
Cerebral palsy (CP) is a diverse movement conditions that affects kids born at all gestational stages but is more severe in preterm babies often accompanied by sensory disorders, perception, cognition, and musculoskeletal problems [1]. In industrialized countries, this is the most common clinical subtype of a cerebral paralysis, while it is the second most common in developing countries. However, in recent research has found that the percentage of spastic diplegic cases increased from 22% to 34.5% over the last decade [2]. Moreover, with a prevalence estimated range from 1.5 to 4.2 per 1,000 live births, according to recent population-based research from around the world [3].
Cerebral palsy (CP) is a diverse movement conditions that affects kids born at all gestational stages but is more severe in preterm babies often accompanied by sensory disorders, perception, cognition, and musculoskeletal problems [1]. In industrialized countries, this is the most common clinical subtype of a cerebral paralysis, while it is the second most common in developing countries. However, in recent research has found that the percentage of spastic diplegic cases increased from 22% to 34.5% over the last decade [2]. Moreover, with a prevalence estimated range from 1.5 to 4.2 per 1,000 live births, according to recent population-based research from around the world [3].
When the GMFCS (Gross motor function classification system)
was used to evaluate the patient, the diagnostic of spatic diplegia
cerebral palsy was confirmed. Physiotherapy at www.spinallife.in to
be useful in minimizing problems and improving patient outcomes.
The majority of people with CP contracts show that passive mutual
motion is not present [4]. The mechanism that causes contractures
are unknown. On the other hand, physical activities benefit all
children since it has been related to improvements in energy, stamina,
self-esteem, social –participation and overall enjoyment. Specific
spatial and temporal muscle activation may be absent in children
with cerebral paralysis. Cerebral palsy is considered one of the most
disabling conditions in childhood [5].
Clinical forms of PC (personal care) are characterized by motor and posture disorders, deficiencies of various types and intensities –which may be associated with involuntary movements and ataxic coordination disorders. Henceforth the most common clinical form of spastic CP (spastic cerebral palsy), which is found in over 86% of cases [6], as shown in [Figure 1].
Clinical forms of PC (personal care) are characterized by motor and posture disorders, deficiencies of various types and intensities –which may be associated with involuntary movements and ataxic coordination disorders. Henceforth the most common clinical form of spastic CP (spastic cerebral palsy), which is found in over 86% of cases [6], as shown in [Figure 1].

Cerebral Palsy affects youngsters and produces a wide range of
symptoms and difficulties. On the other hand, the physiotherapist
(PT) must choose evaluations that appropriately represent the desired
domain – outcome metrics for the individual CP when conducting
occupational therapy and Physiotherapy treatment [7] as shown in
[Figure 2].
In children with cerebral palsy, functional electrical stimulation
has been found to improve range of motion, muscle mass, muscle
strength, walking speed, spasticity, gait, and foot and ankle
positioning. FES stimulates peripheral nerves to activate muscle
contraction [8].
Improving gait in spastic cerebral palsy with FES − Spastic
cerebral palsy (SCP) is the most common form of this condition,
affecting about 80 percent of all children with CP [9]. Recent studies
show that FES can be used to help children with spastic cerebral palsy
walk better and move easily. In one such study, the children received
eight weeks of daily functional electrical stimulation to the muscles
[10]. All the children were evaluated at the beginning of the study,
again at the end of the eight weeks of treatment at www.Spinallife.
in , and six weeks after that. They were assessed for their walking
ability and their own perceptions of how they were walking. Those
who received the treatment showed significant improvements in how
they perceived their ability to work. These children felt that they could
walk better and when less pain.
Moreover, it occurs as a result of damage to the pyramidal system and is characterized by persistent, invariable hypertension, accentuated in the upper limbs on flexors and pronators and in the lower limbs on extensors and adductor muscles, accompanied by decreased muscle strength and motor deficit , stiffness and muscle atrophy secondary to inactivity hyperreflexia, pathological reflexes (Babinski sign) and clonus.
Upper limb tone and posture disorders specific- spastic cerebral palsy have a strong negative impact on hand functionality, decreased muscle strength, abnormal range of motion and coordination deficits leading to deterioration in quality of life in children with CP. The most frequent upper limb contracture patterns encountered in spastic CP are adduction and internal rotation of the shoulder,
Moreover, it occurs as a result of damage to the pyramidal system and is characterized by persistent, invariable hypertension, accentuated in the upper limbs on flexors and pronators and in the lower limbs on extensors and adductor muscles, accompanied by decreased muscle strength and motor deficit , stiffness and muscle atrophy secondary to inactivity hyperreflexia, pathological reflexes (Babinski sign) and clonus.
Upper limb tone and posture disorders specific- spastic cerebral palsy have a strong negative impact on hand functionality, decreased muscle strength, abnormal range of motion and coordination deficits leading to deterioration in quality of life in children with CP. The most frequent upper limb contracture patterns encountered in spastic CP are adduction and internal rotation of the shoulder,
elbow-flexion, forearm-pronation, wrist flexion and clasp hand with
thumb in palm [11,12], it is shown in [Figure 3].
Functional electrical stimulation (FES) can be used in spastic diplegic children with upper limb involvement to improve muscle strength, range of motion, and spasticity. Studies show it can be used in a variety of ways, often combined with traditional therapy, to help with functional activities like grasping, reaching, and manipulating objects. The goal is to improve upper limb function, increase motor capacity, and enhance the benefits of rehabilitation programs.
FES involved transcutaneous administration of electrical impulses to muscles to produce a contraction and obtain functionally useful movement [13]. FES emphasizes active, repetitive, task-specific movement of the paretic arm and hand and has been shown to increase function, range of motion [14], enhance muscle strength [15], and improve muscle tone [16] of the UL in individuals with neurological conditions, such as stroke, [17] and spinal cord injury [18,19]. To date, studies have shown that FES therapy can lead to recovery of UL function, specifically improvements in dexterity, ROM and ADLs have been shown in adults with sub-acute stroke [20-23].
Benefits of increased limb awareness [24], and improved sensory function [25] have been reported as well. Moreover, previous approaches applying FES for the upper limb usually targeted one or two muscles only [26]. There are only a few published studies employing therapeutic functional electrical stimulation in CP, and those are mainly focused on gait and lower-limb rehabilitation [27].
Functional electrical stimulation (FES) can be used in spastic diplegic children with upper limb involvement to improve muscle strength, range of motion, and spasticity. Studies show it can be used in a variety of ways, often combined with traditional therapy, to help with functional activities like grasping, reaching, and manipulating objects. The goal is to improve upper limb function, increase motor capacity, and enhance the benefits of rehabilitation programs.
FES involved transcutaneous administration of electrical impulses to muscles to produce a contraction and obtain functionally useful movement [13]. FES emphasizes active, repetitive, task-specific movement of the paretic arm and hand and has been shown to increase function, range of motion [14], enhance muscle strength [15], and improve muscle tone [16] of the UL in individuals with neurological conditions, such as stroke, [17] and spinal cord injury [18,19]. To date, studies have shown that FES therapy can lead to recovery of UL function, specifically improvements in dexterity, ROM and ADLs have been shown in adults with sub-acute stroke [20-23].
Benefits of increased limb awareness [24], and improved sensory function [25] have been reported as well. Moreover, previous approaches applying FES for the upper limb usually targeted one or two muscles only [26]. There are only a few published studies employing therapeutic functional electrical stimulation in CP, and those are mainly focused on gait and lower-limb rehabilitation [27].


Henceforth, it is surprising because children with congenital spastic
diplegia often share a similar underlying mechanism of injury [28], it
is shown in [Figure 4].
Outcome measures:
The assessment also involved gathering demographic variables
including gender, age, and side of involvement. Brain injury patterns
were collected from the patients – available neuroimaging (MRI or
CAT scan) data, and the child’s ability to manipulate objects in daily
activities was classified applying the Manual ability classification
system ages between (five level system and 4-8 years old children of
CP) [29], as well as the ability to carry out self-initiated movements
related to sitting and walking with the Gross Motor Function
Classification system (GMFCS) [30].Intervention:
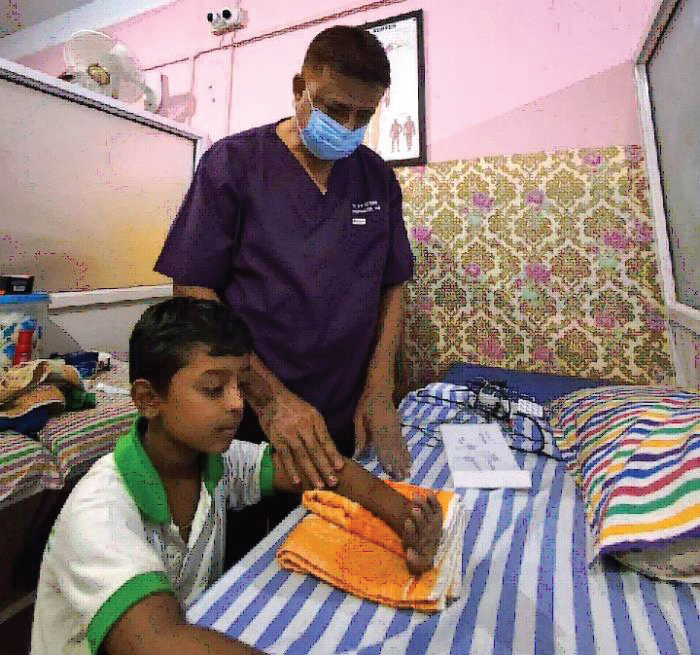
The FES was delivered during 45−60 minutes therapy sessions
three days a week, over approximately 15 −20 weeks, for up to
maximum of 48 sessions by trained physiotherapist. The experimental
set up is presented in [Figure 1]. The participant was seated with the
arm unsupported and the therapist triggered the stimulation using a
foot switch.Contraindications:
Functional electrical stimulation is not suitable for everyone
and should not use by people with pacemakers, active deep-vein
thrombosis (DVT) or those who are pregnant.Procedure and participants:
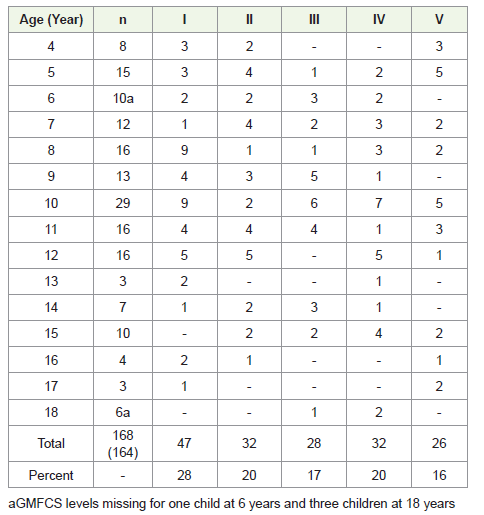
As originally planned, we started by classifying children aged
between 4 years to 18 years. During the process of developing
MACS we frequently received comments from the parents as well as
therapists the classification could be valid for children at other ages
as well. We decided to include children between 4 and 18 years in
the reliability testing. In total 168 children between 4 and 18 years
(98 males, 70 females) were classified by as shown in [Table 2] .
Moreover, the severity of disability according GMFCS varies, and do
the subtype of CP [Table 2,3] .MACS (Appendix-I) is reliable, both between therapists and between parents and therapists. On the other hand, several parents mentioned the importance of highlighting the children’s ability to use

their hands. Henceforth, we also believe that MACS will enhance the
communication among professional and families in the same way as
the GMFCS, ie. To determine the child’s need, make management
decisions, and compare and generalize results of intervention [31].
Conclusion
Functional electrical stimulation (FES) presents valuable
strategy for improving motor performance in cerebral palsy,
especially for lower limb function. Future research should prioritize
protocol standardization, large-scale trials, and long-term effects to
support clinical integration of functional electrical stimulation into
personalized rehabilitation plans.
Funding:
All authors certify that they have no affiliations with or
involvement in any organization or entity with any financial interest
or non-financial interest in the subject matter or materials discussed
in this manuscript.Compliance With Ethics Requirements:
The authors declare no conflict of interest regarding this article.
Informed consent was obtained from all the concerned patients
included in the studyConsent for publication: Not applicable
Competing interest: The authors declare that they have no competing interest.
Competing interest: The authors declare that they have no competing interest.
Acknowledgement
We acknowledge the parents and therapist without whose
contribution this study would not have been accomplished. We also
thank those parents who participated in the validating process.
This study is a part of the research carried out within the P G final
year Physiotherapy Thesis in Neurology.
The author would like to thank the Head of the Department, Dr. Priyanka Goswami, Mahatma Gandhi University, Ri-Bhoi District, Meghalaya, Pin-793101, for her support of the study, her involvement and her enthusiasm.
The author would like to thank the Head of the Department, Dr. Priyanka Goswami, Mahatma Gandhi University, Ri-Bhoi District, Meghalaya, Pin-793101, for her support of the study, her involvement and her enthusiasm.
References
Citation
Borah AK, Goswami P. The Potential Benefits of Functional Electrical Stimulation (FES) Particularly for Spastic Diplegia CP in Children- Recent Advancement and Interventions. Indian J Neurol. 2025;6(1): 162.