Case Report
A Rare Association of Fahr’s Syndrome and Hashimoto’s Encephalopathy
Manoj Prakash Jeyaseelan*, Shobhana N, Sadeesh Kumar V, Selvakumar CJ and Guru S
Department of Neurology, Coimbatore govt medical college and Hospital, Tamil Nadu, India.
*Corresponding author: Manoj Prakash Jeyaseelan, Department of Neurology, Coimbatore govt medical college and Hospital, Tamil Nadu, India. E-mail Id: jmprakas@gmail.com
Article Information:Submission: 29/09/2025; Accepted: 16/10/2025; Published: 18/10/2025
Copyright: © 2025 Manoj Prakash Jeyaseelan, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.
Abstract
Background: Steroid Responsive Encephalopathy Associated with Autoimmune Thyroiditis (SREAT), also known as Hashimoto encephalopathy, is a rare but treatable cause of rapidly progressive dementia. Coexistence with Fahr’s syndrome, an idiopathic bilateral basal ganglia calcification, is
exceptionally uncommon and poses a diagnostic challenge.
Case Presentation: We report a 70-year-old female who presented with a 6-month history of insidious onset behavioral changes, psychosis, cognitive decline, and movement abnormalities including bilateral rest tremors. Laboratory investigations revealed elevated anti-thyroid peroxidase (anti-TPO) antibodies, thyroiditis on ultrasound, elevated parathormone, and vitamin D deficiency. Neuroimaging showed coarse bilateral calcifications in the basal ganglia, dentate nuclei, and occipital gyri consistent with Fahr’s syndrome. Serum autoimmune encephalitis markers were negative. The patient responded dramatically to intravenous pulse steroids and rituximab, with marked clinical improvement and cognitive recovery.
Conclusion: This case highlights the importance of considering SREAT in rapidly progressive dementia even when imaging shows typical Fahr’s syndrome calcifications. Early recognition and immunosuppressive treatment can lead to significant clinical improvement in this potentially reversible disorder, underscoring the need for vigilance in atypical presentations.
Case Presentation: We report a 70-year-old female who presented with a 6-month history of insidious onset behavioral changes, psychosis, cognitive decline, and movement abnormalities including bilateral rest tremors. Laboratory investigations revealed elevated anti-thyroid peroxidase (anti-TPO) antibodies, thyroiditis on ultrasound, elevated parathormone, and vitamin D deficiency. Neuroimaging showed coarse bilateral calcifications in the basal ganglia, dentate nuclei, and occipital gyri consistent with Fahr’s syndrome. Serum autoimmune encephalitis markers were negative. The patient responded dramatically to intravenous pulse steroids and rituximab, with marked clinical improvement and cognitive recovery.
Conclusion: This case highlights the importance of considering SREAT in rapidly progressive dementia even when imaging shows typical Fahr’s syndrome calcifications. Early recognition and immunosuppressive treatment can lead to significant clinical improvement in this potentially reversible disorder, underscoring the need for vigilance in atypical presentations.
Keywords:SREAT; Rapidly progressive dementia; Fahrs syndrome
Introduction
Rapidly progressive dementia refers to cognitive decline with
fast progression which is commonly considered to be less than 1 or 2
years. The etiology includes immune- mediated, infectious, metabolic
encephalopathies which are treatable as well as prion diseases and
atypical rapid presentations of more common neurodegenerative
diseases. Among these, Steroid Responsive Encephalopathy
Associated with Autoimmune Thyroiditis (SREAT), also known
as Hashimoto encephalopathy, is a rare but important treatable
cause characterized by subacute cognitive decline, psychiatric
manifestations, elevated thyroid autoantibodies, and a favorable
response to immunosuppressive therapy.
Fahr’s syndrome, defined by bilateral basal ganglia and other
brain region calcifications, is an uncommon neurodegenerative
disorder classically associated with movement disorders and cognitive
impairment. The coexistence of Fahr’s syndrome and SREAT is
rare and poses a diagnostic dilemma, especially when imaging
abnormalities suggest a neurodegenerative process
This case report describes an elderly female patient presenting with rapidly progressive dementia and neuropsychiatric symptoms, found to have elevated anti-thyroid antibodies and classic basal ganglia calcifications consistent with Fahr’s syndrome.
This case report describes an elderly female patient presenting with rapidly progressive dementia and neuropsychiatric symptoms, found to have elevated anti-thyroid antibodies and classic basal ganglia calcifications consistent with Fahr’s syndrome.
Case report
A 70-year-old female had presented with complaints of insidious
onset slowness of activities for 2 years and behavioural disturbances
which started as episodes of anger outbursts, usage of foul language,
auditory and visual hallucinations, delusion of persecution for 6
months. There was no history of fever, headache and seizures. The
patient also had history of irrelevant talks, throwing up of objects and
later developed way finding difficulty. Later on, the patient became
apathetic requiring assistance for all activities of daily living.
On examination -The patient was awake, irritable, not cooperative,
disoriented with lack of attention. MMSE-6. She was afebrile. without
signs of meningeal irritation. Both pupils were equal, 3mm and
reacting to light. She was moving all 4 limbs with a power of 4/5.
However, they were rigid and bradykinetic. All DTRs were brisk with
bilateral extensor plantar response. There was bilateral rest tremor of
hand (left>right).
On investigation -The patient had normal hemogram with normal
liver and renal function test.
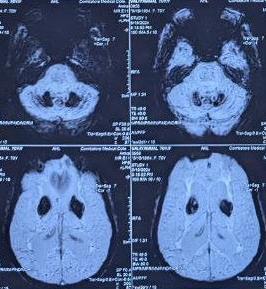
MRI brain was suggestive of coarse calcification in bilateral
basal ganglia, dentate nuclei and occipital gyri. She had low normal
serum calcium level. With elevated parathormone levels and vit-D3
deficiency. Her TSH- 5.4 iu/L. CSF analysis showed acellular smear
with elevated protein level of 97 g/dl.
EEG showed a normal record:
In view of subacute onset of behavioural symptoms. Serum
markers of autoimmune encephalitis were tested which turned
negative. However Anti TPO antibodies were 917 IU/ml with elevated
ESR and C-Reactive protein. Ultrasound scan of neck was suggestive
of thyroiditis.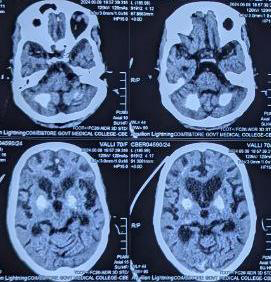
A diagnosis of Hashimoto Encephalitis was considered:
The patient was treated with Intravenous Injection.
Methylprednisolone 1 gm for 5 days along with vitamin D3 and
calcium supplements and also with Inj. Rituximab 1gm 1 week after
pulse steroid course.5 days after the rituximab dose the patient’s cognition started improving. Her MMSE score improved to 27 at the time of discharge. However, there was no improvement with respect to her motor disability. she was discharged on tapering doses of steroid
Discussion
Most SREAT case reports describe a female predominance
with a wide age range, often presenting with subacute or chronic
neuropsychiatric symptoms, cognitive decline, psychiatric
disturbances, and occasionally movement disorders such as
myoclonus or tremor.
High anti-TPO titers are a hallmark in nearly all SREAT cases, even in the presence of normal or slightly abnormal thyroid function tests [1-3]. CSF often shows elevated protein without pleocytosis. [3]
Imaging varies: While many cases report normal MRIs or nonspecific changes, some describe white matter changes or atrophy. Unusually, this case features coarse calcifications in basal ganglia, dentate nuclei, and occipital gyri, meeting radiological criteria for Fahr’s syndrome.[1,4]
It is quite challenging to distinguish Fahr’s calcifications from agerelated changes or other metabolic causes. However, the coexistence of autoimmune thyroiditis and Fahr’s syndrome points to possible metabolic or autoimmune overlap.[4-7]
High anti-TPO titers are a hallmark in nearly all SREAT cases, even in the presence of normal or slightly abnormal thyroid function tests [1-3]. CSF often shows elevated protein without pleocytosis. [3]
Imaging varies: While many cases report normal MRIs or nonspecific changes, some describe white matter changes or atrophy. Unusually, this case features coarse calcifications in basal ganglia, dentate nuclei, and occipital gyri, meeting radiological criteria for Fahr’s syndrome.[1,4]
It is quite challenging to distinguish Fahr’s calcifications from agerelated changes or other metabolic causes. However, the coexistence of autoimmune thyroiditis and Fahr’s syndrome points to possible metabolic or autoimmune overlap.[4-7]
Fahrs syndrome presents with insidious onset movement disorder
like tremor, bradykinesia, rigidity and also cognitive decline and
psychosis particularily late in onset, as in our patient.
The literature highlights diagnostic dilemmas when metabolic or
degenerative findings (e.g., Fahr’s calcifications) coexist, sometimes
confounding initial impressions or delaying immunotherapy.[1,4,5]
The rapid progress in cognitive decline and psychosis prompts to
look for other possible causes to exclude.
SREAT remains a diagnosis of exclusion, based on characteristic
clinical syndrome, high antithyroid antibody titers, and steroid
responsiveness.[1-3] Other treatable RPDs such as voltage-gated
potassium channel antibody encephalitis and NMDA-R encephalitis
present with slightly different syndromes and biomarkers.[8,9]
Most reports cite rapid and dramatic improvement with steroids
as highly suggestive of SREAT. Immunosuppressants or biologics
(such as rituximab) are reserved for refractory cases.[1-3]
The discussed patient responded well to pulse steroid and
rituximab, paralleling outcomes in published series, emphasizing the
treatable nature of SREAT despite atypical imaging.[1]
Fahr’s syndrome, with basal ganglia calcification and elevated
parathormone, has occasionally been reported alongside autoimmune
thyroiditis (chronic lymphocytic thyroiditis). Few case reports
highlight this overlap, hinting at shared autoimmune or metabolic
pathways.[1,5-7]
Conclusion
This case underscores that steroid-responsive encephalopathy
associated with autoimmune thyroiditis (SREAT) should be
considered in rapidly progressive dementia, even in the presence
of basal ganglia calcifications suggestive of Fahr’s syndrome. The
unique radiological overlap highlights possible coexistence of
neurodegenerative and autoimmune-metabolic processes in elderly
patients. High anti-thyroid antibody titers and dramatic steroid
responsiveness are key diagnostic clues for SREAT, despite atypical
imaging findings. Timely institution of immunomodulatory therapy,
including steroids and biologics, can lead to significant neurological
recovery in such atypical presentations.
References
Citation
Jeyaseelan MP, Shobhana N, Sadeesh Kumar V, Selvakumar CJ, Guru S. A Rare Association of Fahr’s Syndrome and Hashimoto’s Encephalopathy. Indian J Neurol. 2025;6(1): 161.