Research Article
Effect of Excitatory repetitive Transcranial Magnetic Stimulation over Left Dorsolateral Prefrontal Cortex on Depression and Motorrecovery in Ischemic Stroke Patients
Gupta R1, Kumar N2 and Srivastava AK3*
1,3Department of Neurology, All India Institute of Medical Sciences, New Delhi, India
2Department of Psychiatry, All India Institute of Medical Sciences, New Delhi, India
2Department of Psychiatry, All India Institute of Medical Sciences, New Delhi, India
*Corresponding author:Achal Kumar Srivastava, Department of Neurology, All India Institute of Medical Sciences, New Delhi, India. E-mail Id: achalsrivastava@hotmail.com
Article Information:Submission: 23/09/2025; Accepted: 11/10/2025; Published: 14/10/2025
Copyright: © 2025 Gupta R, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
30 - 50% of stroke survivors develop depression during the first six months known as post-stroke depression (PSD). Repetitive transcranial magnetic stimulation (rTMS) is an FDA-approved therapy for the treatment of major depression in psychiatric cases. However, rTMS is being investigated for the
treatment of post-stroke depression (PSD). Preliminary reports suggest that excitatory 10 Hz rTMS applied over left Dorsolateral Prefrontal cortex (L-DLPFC) area has a beneficial effect in reducing PSD symptoms. However, systematic meta-analyses of those studies suggest that they suffer from several drawbacks.
Reducing PSD is important because it can enhance the post-stroke motor recovery. It can enhance motor recovery either due to motivational benefits or directly by strengthening the cortical connections, but this has not been tested in detail yet. Thus, in this work it is hypothesised that excitatory 10 Hz rTMS of
L-DLPFC will reduce PSD symptoms and reduction of depression will enhance motor recovery either due to motivational or other benefits. To assess that in this work MCA ischemic stroke patients suffering from PSD and hemiplegia were recruited and provided the excitatory rTMS treatment. Our results suggest
that the given rTMS treatment is effective in reducing PSD symptoms significantly but has no immediate impact on motor function in those patients. In future studies, it is planned to study the long-term impact of PSD reduction on motor-recovery.
Keywords:Post-stroke depression; rTMS; Middle Cerebral Artery (MCA) Occlusion; Ischemic stroke; Motor recovery
Introduction
Stroke is a common medical illness. In the United States, there
are approximately 800,000 new cases each year [1]. Currently, an
estimated 4.5 million stroke survivors reside in the United States.
Stroke survivors in whom motor-weakness or paralysis of limbs
develops, makes it difficult for them to perform the basic activities
of daily living, which mostly leads to depression in them. This poststroke
depression (PSD) hampers their motor recovery. PSD has been
identified as a major challenge in stroke recovery. At stroke onset,
patient’s age, sex, marital status, number of children, occupation,
family responsibilities, education, support from caregivers, laterality
of stroke, financial status/load and other illnesses are important
deciding factors in the development of PSD. It has been observed
that around 30 - 50% of stroke patients develop depression within 6
months after stroke. Thus, it is important to evaluate and treat PSD
as its recovery will improve the quality of life of stroke-survivors
[1]. It is believed that there is an association between depression
and hypo-activity of left dorsolateral prefrontal cortex (L-DLPFC).
Currently, drugs are used for PSD treatment which generates a lot of
toxic effects. Repetitive transcranial magnetic stimulation (rTMS) is
a relatively novel therapy which has shown preliminary, promising
results in the treatment of PSD [2]. In rTMS, strong magnetic pulses
are delivered utilizing a powerful magnet at a fixed frequency over
a defined brain area. It has been observed that rTMS applied to any
brain area at ≤ 1 Hz pulse frequency has inhibitory effect on that area
and nearby neurons whereas at > 5 Hz it has excitatory effect.
In one study, ten sessions of rTMS (10 Hz, 110% of the resting
motor threshold, 20 trains of 5 seconds duration) applied over the
L-DLPFC has been shown to have a significant reduction in PSD
symptoms [3]. In another study on PSD patients (n=20) with either left
or right hemispheric lesion at stroke onset, application of ten sessions
of low frequency rTMS over left DLPFC (1 Hz, at 100% of resting
motor threshold) showed 41.3% reduction of Hamilton Depression
Rating Score (HAMD score) and this effect was maintained for one
month [4]. Further, a sham-controlled study showed that five sessions
of high frequency (10 Hz) rTMS for five consecutive days over the
region spanning from the dorsal anterior cingulate cortex to medial
prefrontal cortex led to a decline in the severity of apathy and degree
of depression in chronic stroke patients [5]. A meta-analysis of 22
RCTs (n=1764 patients) reported beneficial effects of rTMS on poststroke
depression using HAM-D as primary outcome [6]. In addition
to that, a sham-controlled, double-blind prospective study showed
that ten sessions of 10 Hz rTMS (110% resting motor threshold, 5
s/train, 20 trains with 1 minute interval, total 1000 pulses) over
left DLPFC in chronic post-stroke depression patients improved
depression (measured by HAMD-17 and Beck Depression Inventory
(BDI) scores) but no significant motor-recovery was reported [7].
Accelerated rTMS (20 Hz frequency, 110% of resting motor threshold,
applied over DLPFC area (five sessions per day for four consecutive
days for total 20 sessions) was given to ischemic stroke patients (n=6)
(within 2 weeks to six months post-stroke) suffering from post-stroke
depression identified using HAMD. Accelerated rTMS significantly
decreased HAMD score but no significant difference was found
in modified Rankin scale, functional independence measures and
National Institute of Health Stroke Scales [8].
Although the above-mentioned preliminary studies suggests that
excitatory 10 Hz rTMS applied over left DLPFC area has a beneficial
effect on post-stroke depression but meta-analyses of different
studies shows that they are highly heterogenous in terms of small
or inadequate sample size and highly variable therapy assessment
criteria in different studies etc. [9-12]. Dorsolateral prefrontal cortex
is anatomically connected with the primary motor cortex (M1) and
other associated motor areas, both being part of the frontal lobe, thus
it is reasonable to hypothesize that rTMS stimulation of L-DLPFC can
enhance post stroke motor-recovery. In addition to that, L-DLPFC
stimulation can have motivational benefits to the patient which
should enhance motor recovery. Keeping all this in view, in this
work it was hypothesised that excitatory rTMS treatment provided
in L-DLPFC area will reduce PSD symptoms and will enhance motor
recovery.
Methodology
a. Subjects:
Forty post-stroke depressed patients (> 6 months old) of Middle
cerebral artery (MCA) Occlusion with left or right sided paralysis
(hemiplegia) of similar degree were recruited from Neurology
OPD, AIIMS, New Delhi using the below-mentioned inclusion and
exclusion criteria. Patients were randomly recruited in the rTMS
(n=20) or the Sham/control group (n=20). A patient with a BDI-II
score > 17 was taken as clinically depressed [13].Inclusion Criteria:
Stroke patients with similar level of depression and motor-deficits
as assessed by BDI and Barthel Index (BI score) were recruited in
both the rTMS and Sham group [14].Exclusion Criteria:
Stroke patients with any type of seizure activity, any major
head injury in the past or having daily headaches. Patients with
MRI contraindications such as stents, aneurysm clips, and cardiac
pacemaker or defibrillator. Patients with severe systemic disease,
encephalitis, auto-immune disorders or tumors/cancers. Patients with
neurodegenerative or psychiatric disorders like chronic headaches,
Parkinson’s, multiple sclerosis, Alzheimer’s, cerebral palsy, CJD or
bipolar disorders. Patients with rapidly progressing dementia and
language comprehension deficits. Patients with movement disorders.
Depressed patients who are actively suicidal. Currently breast feeding
or pregnant females. Patients not willing to give consent.Informed consent was taken from all the patients as and when it was decided that they can participate in the study.
b. Pre-rTMS BI and BDI-II scores:
Before providing the rTMS treatment, BDI and BI scores were
noted from all the patients by a neurologist not involved in this study.c. rTMS procedure:
rTMS was applied using Magstim rapid 2 stimulators. All the
patients recruited in the rTMS group were given the same rTMS
treatment using the below-mentioned procedure. Patients in the
sham group were also provided the same rTMS treatment but the coil
was kept at 90 degrees to the patient’s scalp creating a placebo effect.Procedure: A figure 8-shaped magnetic coil was placed over left DLPFC (F3 position) and repetitive magnetic pulses were delivered at a frequency of 10 Hz, at an intensity of 110% of the resting motor threshold, duration of 5 seconds and total of 20 trains (total 1000 pulses) separated by 40 s inter-train interval [7]. The procedure was repeated for 4 weeks, five times a week (Monday-Friday) at the same day time.
d. Post-rTMS BI and BDI-II scores:
BI and BDI-II scores were again recorded on the last day of 4th
week of rTMS treatment. All the scores were noted by a neurologist
not involved in this study. Mean ± standard deviation of the values
in the two groups were calculated. Paired Student’s t-test was used
for the statistical comparision between the pre-post values in the two
groups.Results
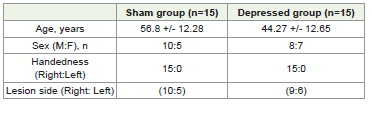
Out of forty recruited patients, thirty patients only completed
the entire procedure. [Table 1] shows mean ± standard deviation of
patients’ demographic data in the two groups, sham (control group)
and experimental rTMS group. The two groups were choosen in such
a way that there was no statistically significant difference between
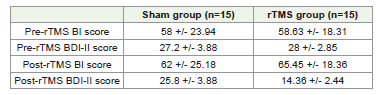
the two groups in terms of demographic features. [Table 2] shows
the pre- and post-rTMS BI and BDI-II scores of the sham and the
rTMS group. Our results suggest that excitatory rTMS over L-DLPFC
significantly reduce PSD symptoms as suggested by the decrease in
the BDI score.The decrease in the BDI score in the rTMS treatment
group was found to be statistically significant at p < 0.05, however,
in group with sham exposure, pre-post BDI scores were statistically
non-significant. This suggests that the observed difference in BDI
score or reduction of PSD symptoms in the rTMS group is because
of the given rTMS treatment. Furthermore, the reduction in PSD
symptoms in the rTMS group was same irrespective of the laterality
of the stroke. No statistically signifant difference was observed for
the BI score between the Sham and the rTMS treatment group which
suggests our rTMS treatment did not provide any motor recovery to
the stroke patients.
Discussion
The aim of this study was to assess the impact of excitatory rTMS
applied over the left dorsolateral prefrontal cortical area (DLPFC)
on depression and motor recovery in post-stroke depression (PSD)
patients. Several investigations have been carried out to study the
effect of rTMS on PSD and has shown positive outcome. Also, several
mechanisms have been proposed explaining the beneficial effects
of excitatory rTMS such as increase in the BDNF levels [15]. PSD
results in reduction of BDNF levels. Low levels of BDNF results in
mood dysregulation and loss of hippocampal function. In rats, high
frequency rTMS (20 Hz) has been shown to trigger BDNF expression.
Apart from increasing BDNF expression, it can activate the BDNF/
ERK signalling, which is important for hippocampal cell proliferation
[15]. Glucose metabolism is known to decrease in the ischemic
hemisphere, especially in patients with PSD. Using FDG-PET imaging
it has been shown that rTMS increases glucose uptake in rat cortex
and striatum [15]. It also inhibited apoptosis in the ischemic brain.
Similarly, rTMS has been shown to induce neurogenesis. Stroke can
lead to abnormal changes in the concentration of neurotransmitters
and cytokines and excessive generation of free radical species.
Experimental evidence in rodents suggests that rTMS corrects for all
these factors [15]. Studies conducted in the recent past, has analysed
the effect of dual target rTMS (L-DLPFC and ipsilesional primary
motor cortex) on serological markers such as Brain derived growth
factor (BDNF) and Vascular Endothelial growth factor (VEGF)
and also imaging techniques such as Transcranial Colored Doppler
(TCD) have been assessed to address the effect of rTMS on Post
stroke cognitive impairnment (PSCI) recovery [16]. There are reports
suggesting that 10 Hz rTMS applied over L-DLPFC area is effective
in reducing post-stroke depressive symptoms but reducing PSD will
have any functional outcome in stroke recovery has not been studied
in detail yet. In this work, middle cerebral artery (MCA) ischemic
stroke depressed patients were provided the 10 Hz L-DLPFC rTMS
treatment for major depression. By comparing the effect of same
rTMS treatment in same type of post-stroke depressed patients we
can answer whether PSD treatment with rTMS can have any direct
effect on motor recovery.
Our results suggest that 10 Hz rTMS over L-DLPFC area is
effective in reducing BDI-II score of depression in post-stroke
depressed patients but no major difference was noted in Barthel Index
scores for motor recovery. This suggests that excitatory rTMS has no
immediate beneficial effect on motor recovery. In a nut shell, these
findings strongly suggest that L-DLPFC excitatory rTMS treatment
is very helpful in PSD recovery but it is less likely to enhance motor
recovery in ischemic stroke patients. We would like to mention that
our findings are strongly in line with the previous findings on the
effect of excitatory L-DLPFC rTMS treatment on PSD treatment
and functional/motor recovery [7,8]. In conclusion, this study
compliments earlier studies on the beneficial role of rTMS in PSD
recovery. Future studies will be conducted to check the long-term
benefits of rTMS treatment on motor recovery.
Acknowledgements
Dr. Gupta is thankful to Indian Council of Medical Research
(ICMR) for providing him the Research Associate fellowhip (Ref. No.
3/1/3/92/Neuro/2018-NCD-I) and Prof. Achal Kumar Srivastava for
providing the lab facility.
Conflict of Interest:
All authors declare no conflict of interest.References
Citation
Gupta R, Kumar N, Srivastava AK. Effect of Excitatory repetitive Transcranial Magnetic Stimulation over Left Dorsolateral Prefrontal Cortex on Depression and Motor-recovery in Ischemic Stroke Patients. Indian J Neurol. 2025;6(1): 160.