Case Report
Epstein–Barr Virus Meningoencephalitis Presenting with Extrapyramidal Symptoms in an Immunocompetent Adult Female: A Rare Case Report
Bhargav NP*, Naik KR, Saroja AO, Makandar Kutub, Sumanth CV and Triveni Ayanna
Department of Neurology, Jawaharlal Nehru Medical College and KLES Dr. Prabhakar Kore Hospital and MRC, Belagavi, Karnataka, India
*Corresponding author:Dr. Bhargav NP, Department of Neurology, Jawaharlal Nehru Medical College and KLES Dr. Prabhakar Kore Hospital and MRC, Belagavi, Karnataka, India. E-mail Id: npbhargav4271@gmail.com
Article Information:Submission: 07/08/2025; Accepted: 22/09/2025; Published: 26/09/2025
Copyright: © 2025 Bhargav NP, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Epstein–Barr virus (EBV) is an infrequent yet important cause of meningoencephalitis, especially in immunocompetent individuals. [1] We present young patient, previously healthy woman who developed progressive neuropsychiatric and motor symptoms following a ritualistic holy dip. Her course wascomplicated by rural tremors, dystonia, rigidity, and quadriparesis. Despite broad-spectrum antimicrobial and antiviral therapy, the clinical response was initially limited. CSF polymerase chain reaction (PCR) ultimately revealed EBV as the causative pathogen. The patient underwent prolonged hospitalization
with supportive neuro-rehabilitative care and gradual clinical recovery. This case emphasizes the need for high suspicion of EBV in atypical neuro-infections and the importance of early PCR-based diagnosis.
Introduction
[1]Epstein–Barr virus (EBV), a member of the Herpesviridae
family, is among the most prevalent human viruses globally, with
over 90% of the adult population estimated to be seropositive. [2]
Though primarily recognized for causing infectious mononucleosis,
EBV is also associated with a variety of malignancies, autoimmune
conditions, and—less commonly—central nervous system (CNS)
disorders. [3] Neurological manifestations of EBV are under reported
in the immunocompetent population due to their subtle presentation
and diagnostic challenges. Nevertheless, when CNS involvement does
occur, the consequences can be severe and long-lasting. [4] EBV has
the capacity to infect both epithelial cells and B lymphocytes, leading
to latent infection within the host. [5] The neurological sequelae
may stem from direct viral invasion of the CNS or, more commonly,
from immune-mediated processes. The virus can enter the CNS via
hematogenous spread or through retrograde axonal transport. The
resulting clinical syndromes can include encephalitis, meningitis,
cerebellitis, myelitis, cranial nerve palsies, and movement disorders
such as parkinsonism or opsoclonus-myoclonus. In some cases,
acute disseminated encephalomyelitis (ADEM) or Guillain–Barré
syndrome may also occur.
Case Presentation
A 24-year-old lady, recently married, presented with subacute
neurological symptoms for 15 days after participating in a religious
holy dip at Murudeshwar. Initially asymptomatic, she developed
high-grade fever with chills that persisted for over a week. This was
followed by the insidious onset of severe diffuse headache, giddiness,
and visual disturbances characterized by blurring and diplopia. Over
the next few days, she experienced progressive unsteadiness of gait,
behavioral changes including altered sensorium, and involuntary
movements of the limbs.
She had no history of seizures, trauma, animal bites, recent vaccination, skin rash, ear discharge, herpes zoster or arthralgia. There was no significant past medical and surgical history. The symptoms progressed to include dysarthria, emotional lability, and difficulty in performing daily activities, prompting hospital admission.
She had no history of seizures, trauma, animal bites, recent vaccination, skin rash, ear discharge, herpes zoster or arthralgia. There was no significant past medical and surgical history. The symptoms progressed to include dysarthria, emotional lability, and difficulty in performing daily activities, prompting hospital admission.
Clinical Examination
On admission, she was febrile with a pulse rate of 120 bpm and
blood pressure of 120/80 mmHg. She had a normal respiratory rate
and oxygen saturation at room air. General examination revealed
evidence of purulent vaginal discharge and lax anal sphincter are
raising concern for a systemic or neurogenic cause.
• Neurologically, she was confused, with a ‘Glasgow Coma Scale’ score of 14 (E4 V4 M6). Notably, she had dysarthria and dysphonia, though there was no facial asymmetry. Her optic fundi were normal with no papilledema, and pupils were reactive. She exhibited opsoclonus, rubral tremors, finger dystonia, generalized rigidity, and quadriparesis with a Medical Research Council (MRC) grade of 3–4/5. Deep tendon reflexes were brisk, plantar responses were extensor bilaterally, and neck stiffness was present—suggestive of meningeal irritation.
• Neurologically, she was confused, with a ‘Glasgow Coma Scale’ score of 14 (E4 V4 M6). Notably, she had dysarthria and dysphonia, though there was no facial asymmetry. Her optic fundi were normal with no papilledema, and pupils were reactive. She exhibited opsoclonus, rubral tremors, finger dystonia, generalized rigidity, and quadriparesis with a Medical Research Council (MRC) grade of 3–4/5. Deep tendon reflexes were brisk, plantar responses were extensor bilaterally, and neck stiffness was present—suggestive of meningeal irritation.
Investigations:
• Routine Laboratory Workup revealed low haemoglobin
(10.3 g/dl), Leucocytosis (Total leucocyte count of 26,100/
cumm) raised ESR of 36 mm/hr. Liver and renal function
tests within normal limits.• CSF Analysis revealed lymphocytic pleocytosis (total cells-40), normal protein and glucose levels. Meningitis panel is Positive for Epstein–Barr Virus DNA by PCR and antibodies for other viral markers were not detected
• Electrophysiological Studies: EEG revealed generalized slowing with diffuse theta and delta activity, Visual Evoked Potentials are within normal limits, Reduced amplitude of V wave with normal interpeak intervals on auditory evoked potential. Somatosensory Evoked Potentials (SSEP) revealed delayed central conduction in tibial nerve (Right 39.0 ms, Left 33.0 ms).
Treatment:
The patient was started on empirical treatment for
meningoencephalitis: Antibacterial (Ceftriaxone+Ampicillin),
antiviral (Acyclovir), Levodopa+carbidopa and trihexyphenidyl
for extrapyramidal symptoms, prophylactic antiseizure and
anticoagulation therapy as a part of DVT prophylaxis.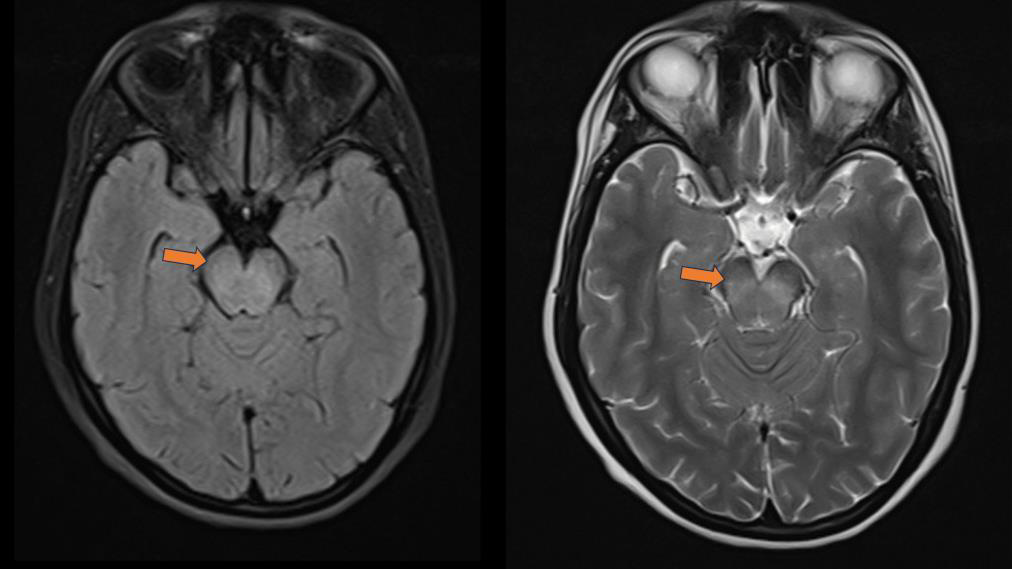
Despite treatment, her symptoms progressed initially with
persistent bulbar signs and behavioural abnormalities. Over several
weeks, multidisciplinary care, physiotherapy, and careful tapering of
medications led to steady improvement.
Discussion
This case report illustrates the varied and complex presentation of
‘Epstein–Barr virus meningoencephalitis’ in an immunocompetent
adult. The patient’s symptoms began with a febrile prodrome and
progressed to severe neurobehavioral, extrapyramidal, and bulbar
manifestations. There is no systemic evidence of Ebstein Barr virus
infection in our patient. EBV-related CNS involvement is relatively
rare in adults with intact immunity, its consequences can be
devastating, particularly when diagnosis and targeted supportive care
are delayed. [6]
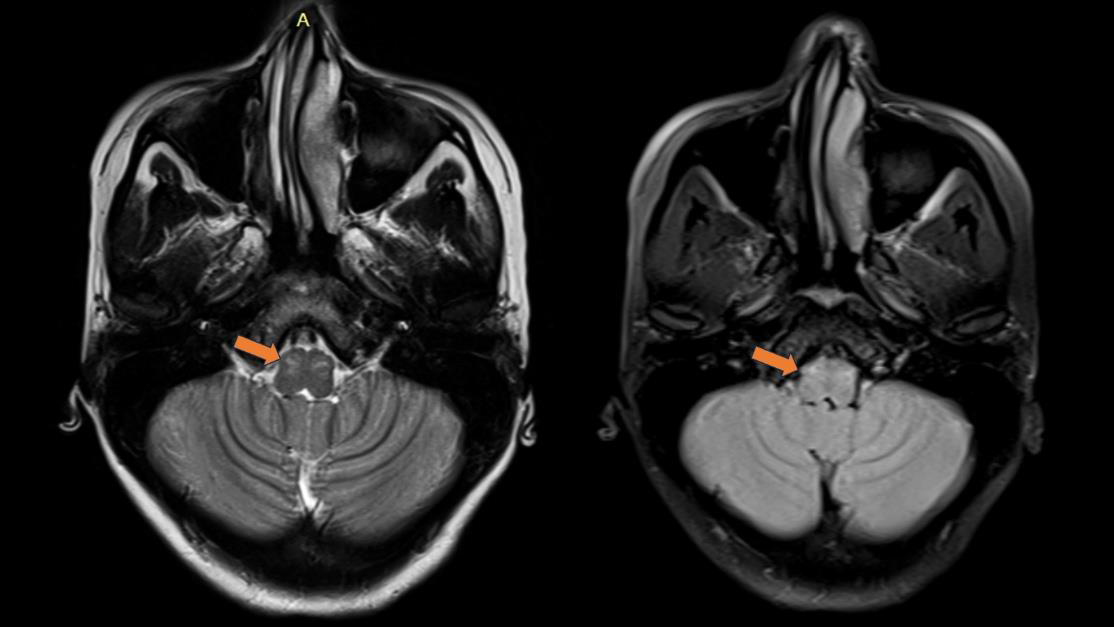
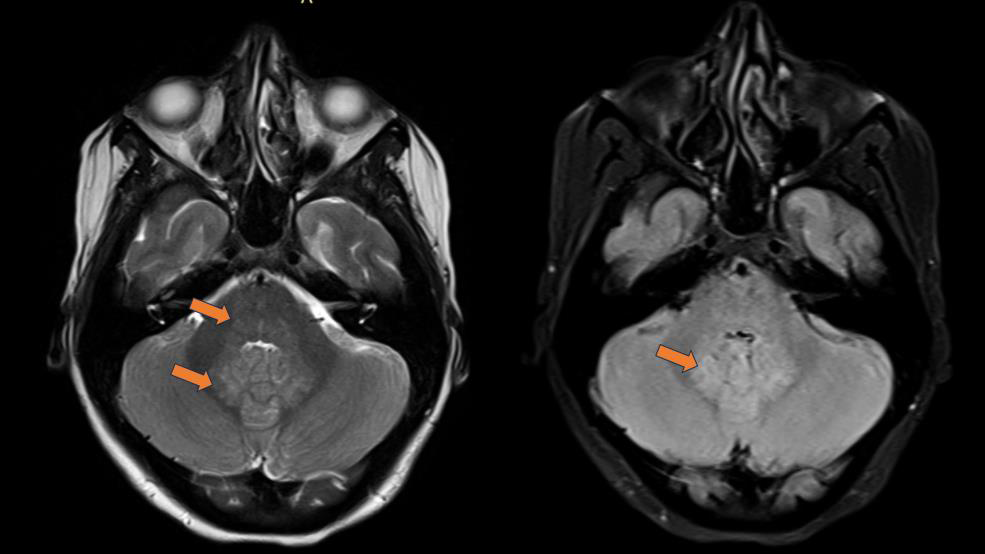
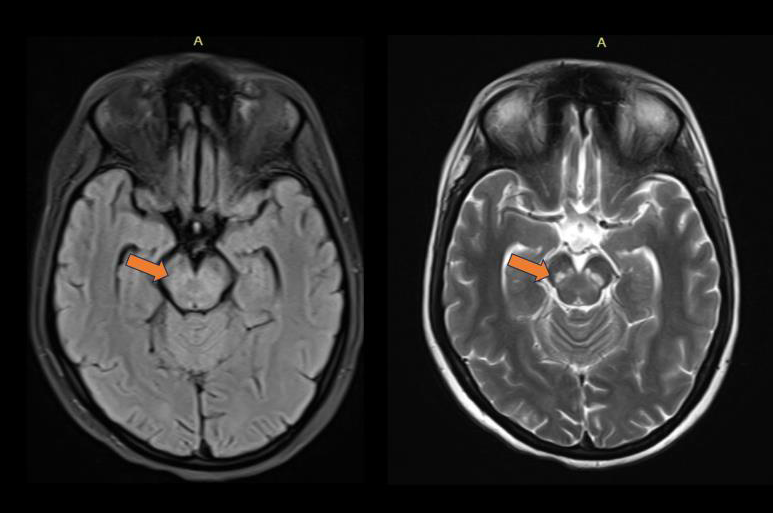
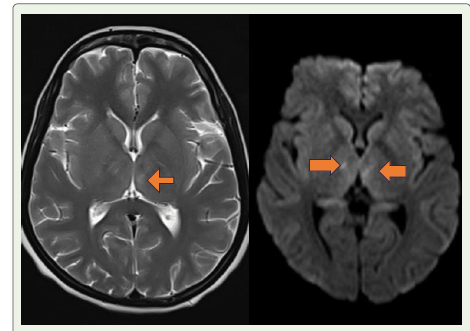
The extrapyramidal signs—including rubral tremors, rigidity,
and dystonia—suggest involvement of the basal ganglia or midbrain
tegmentum, a region frequently implicated in EBV encephalitis, as
documented in case series and radiological reviews. Opsoclonus
and dysarthria point toward cerebellar and brainstem involvement.
Behavioural disturbance like altered sensation and mood disturbance
suggests the involvement of thalamus (supratentorial region).
These diverse neuroaxis involvements reinforce the idea that EBVassociated
encephalitis does not follow a single anatomic pattern,
unlike HSV which typically involves the temporal lobes, or Japanese
encephalitis which has predilection for the thalami and substantia
nigra. Although there are nonspecific manifestations like vaginal
discharge and lax anal sphincter, they may be a secondary infection
and most unlikely in Epstein barr virus infection where vulval ulcers
are more common.
The pathophysiology is believed to be multifactorial, involving
both direct viral invasion and immunologically mediated damage.
EBV can disrupt the blood-brain barrier either directly or through
cytokine-mediated inflammation, allowing infiltration of activated
lymphocytes that contribute to neuronal injury. Molecular mimicry
and the generation of autoreactive antibodies are also hypothesized
mechanisms for the immune-mediated component, which may
explain some of the persistent symptoms even after viral clearance.
In our case report, diagnostic confirmation was achieved through
CSF PCR, which remains the gold standard for identifying active EBV
infection in the CNS. This emphasizes the importance of including
EBV in multiplex PCR panels when evaluating undifferentiated viral
meningoencephalitis.
Treatment is typically supportive. Although acyclovir was
administered due to its activity against herpesviruses, evidence
for its efficacy against EBV in CNS infection remains limited. The
use of Levodopa and Trihexyphenidyl in this case was targeted at
controlling extrapyramidal symptoms. Adjunctive therapies for
movement disorders and psychotropic interventions for behavioural
disturbances are frequently required.
The patient’s prolonged hospital stay and slow neurological recovery reflect the chronic nature of post-viral sequelae. Behavioural disturbances including mood lability and pseudobulbar features, along with mild gait impairment, persisted for months despite overall improvement in motor power and coordination. These longterm outcomes are consistent with literature reports indicating that up to 25–40% of patients with EBV encephalitis may have residual neuropsychiatric symptoms.
Radiological follow-up, though not detailed in this case, can show resolution or progression to cerebral atrophy depending on the severity of the initial insult. Rarely, EBV encephalitis may lead to complications such as brainstem haemorrhage, subdural empyema, or transformation to CNS lymphoma, especially in immunocompromised patients.
The patient’s prolonged hospital stay and slow neurological recovery reflect the chronic nature of post-viral sequelae. Behavioural disturbances including mood lability and pseudobulbar features, along with mild gait impairment, persisted for months despite overall improvement in motor power and coordination. These longterm outcomes are consistent with literature reports indicating that up to 25–40% of patients with EBV encephalitis may have residual neuropsychiatric symptoms.
Radiological follow-up, though not detailed in this case, can show resolution or progression to cerebral atrophy depending on the severity of the initial insult. Rarely, EBV encephalitis may lead to complications such as brainstem haemorrhage, subdural empyema, or transformation to CNS lymphoma, especially in immunocompromised patients.
Comparative literature:
• N Soni et al. (2023) documented pediatric CNS involvement
by EBV, showing that extrapyramidal signs and cerebellar
dysfunction were among the presenting features, which were
also evident in our adult patient. [12]• Huang et al. (2021) described a rare case of EBV encephalitis complicated by brainstem hemorrhage in an immunocompetent adult, highlighting the need for high clinical suspicion and prolonged monitoring.[13]
• S Vyas et al. (2020) summarized radiological manifestations of EBV encephalitis, noting basal ganglia and thalamic involvement as key MRI features, consistent with our patient’s clinical profile. [14]
This case report exemplifies how Epstein–Barr virus can cause severe CNS disease even in healthy individuals. The atypical presentation, delayed diagnosis, and prolonged recovery underscore the need for greater awareness of this entity among neurologists, intensivists, and infectious disease specialists. Comprehensive evaluation including CSF PCR, neuroimaging, evoked potentials, and multidisciplinary rehabilitation is essential for optimal outcomes.
Conclusion
Epstein–Barr virus (EBV) meningoencephalitis, though rare in
immunocompetent individuals, can present with severe and atypical
neurological features such as extrapyramidal symptoms, opsoclonus,
and behavioral changes. This case report highlights the importance
of early CSF PCR testing for diagnosis and the need to consider EBV
in the differential diagnosis of unexplained meningoencephalitis.
Despite an initially poor response, the patient showed gradual
improvement with supportive care, symptomatic therapy, and
rehabilitation. Long-term follow-up is crucial, as neuropsychiatric
sequelae may persist. A high index of suspicion and multidisciplinary
care are essential for timely diagnosis and favourable outcomes in
such complex cases.
References
Citation
Bhargav NP, Naik KR, Saroja AO, Kutub M, Sumanth CV, et al. Epstein–Barr Virus Meningoencephalitis Presenting with Extrapyramidal Symptoms in an Immunocompetent Adult Female: A Rare Case Report. Indian J Neurol. 2025;6(1): 159