Case Report
Subacute Sclerosing Panencephalitis Masquerading as eclampsia: A Case Report and Review of Literature
Sauvik Paul, Bhuwan Jain, Sohan Paikray*, Richa Singh Chauhan, Md Sabah Siddiqui, Saravana Sukriya and Rohini Rokkam
Department of General Medicine, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India
*Corresponding author:Sohan Paikray, Department of General Medicine, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India. E-mail Id: sohanpaikray@gmail.com
Article Information:Submission: 01/08/2025; Accepted: 15/09/2025; Published: 20/09/2025
Copyright: © 2025 Paul S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction: Subacute sclerosing panencephalitis (SSPE) is a rare, progressive neurological disorder caused by persistent measles virus infection. While typically seen in children, adult and postpartum presentations are uncommon and diagnostically challenging.
Aim: To provide the readers a valuable clinical insight to the diagnostic challenges posed by rare neurological conditions presenting outside their usual demographic, and underscores the potential of emerging treatment strategies to improve outcomes in SSPE.
Case: A 26-year-old postpartum female presented with behavioral changes, high-grade fever, and myoclonic jerks that began during pregnancy. She later developed decorticate posturing and hypothalamic dysfunction. CSF and serum analysis revealed elevated anti-measles antibodies. MRI and EEG findings supported the diagnosis of SSPE.
Results: The patient was treated with Intravenous Immunoglobulin (2 g/kg over 5 days) and Isoprinosine (100 mg/kg/day). Marked clinical improvement was observed, including resolution of jerks and improved Glasgow Coma Scale score. This combination therapy showed potential benefit in early SSPE.
Aim: To provide the readers a valuable clinical insight to the diagnostic challenges posed by rare neurological conditions presenting outside their usual demographic, and underscores the potential of emerging treatment strategies to improve outcomes in SSPE.
Case: A 26-year-old postpartum female presented with behavioral changes, high-grade fever, and myoclonic jerks that began during pregnancy. She later developed decorticate posturing and hypothalamic dysfunction. CSF and serum analysis revealed elevated anti-measles antibodies. MRI and EEG findings supported the diagnosis of SSPE.
Results: The patient was treated with Intravenous Immunoglobulin (2 g/kg over 5 days) and Isoprinosine (100 mg/kg/day). Marked clinical improvement was observed, including resolution of jerks and improved Glasgow Coma Scale score. This combination therapy showed potential benefit in early SSPE.
Keywords:SSPE; IVIg; Isoprinosine; Measles
Introduction
Subacute sclerosing panencephalitis (SSPE) is an uncommon,
slowly progressive disease of the central nervous system postulated
to be caused either by the mutated measles virus or an immunemediated
mechanism attributed to anti- measles antibody. The annual incidence of the disease is approximately 1 case per 1 million population, with a male predilection occurring between 5 to 15 years
although unusual ages of occurrence, between 2-35 years have been
reported. The clinical course unfurls in stages with psycho-intellectual
disturbances leading onto convulsive and motor manifestations.
The final stage is characterized by myoclonic jerks, development of spasticity, decorticate posturing, and hypothalamic dysfunction in the form of hyperpyrexia and flushing.[1]
The final stage is characterized by myoclonic jerks, development of spasticity, decorticate posturing, and hypothalamic dysfunction in the form of hyperpyrexia and flushing.[1]
Case Presentation
A 26 years old female with an obstetric score of P3L3 on twenty
second day of her postpartum period, presented to the hospital with
complaints of behavioral changes for preceding ten days in the form
of irrelevant talks and high-grade fever documented to be 1040F.
On probing the husband gave history that in second month of her gestation, she started to have brief involuntary jerky movements of the entire body resulting in backward fall. The patient’s consciousness remained intact through the episodes. She continued to experience such episodes about 8-10 per month up to the last trimester. These were suggestive of myoclonic jerks. She was neither a known case of hypertension nor was any recording of increased blood pressure made during pregnancy. She gave birth to a healthy female child on completion of term through a normal vaginal delivery in a primary health care center with no immediate postpartum complications. On Day 12 of the postpartum period, she presented with behavioral changes to a nearby health facility. Her condition deteriorated despite receiving some conservative management over the next ten days and she started to develop spasms with tonic movements of all four limbs and arching of the back both of which were short lived and recurrent. The episodes were aggravated by external stimulus but subsided on its own. Following such presentation, she was referred to our tertiary care center. There was no history of trismus, tongue bite, frothing from mouth, involuntary urination or defecation. History of yellowish discoloration of sclera, decreased urine output, focal neurological deficit or any drug/toxin exposure was absent in the patient. She had no raised blood pressure in any her pregnancies. The patient as a child was a defaulter in receiving all her vaccines including measles. At the age of 12 she was admitted to a health care facility with complaints of fever with rash that subsided on taking medications. No prior history of animal bite, trauma, unexplained weight loss, psychiatric illness in the past was reported.
On probing the husband gave history that in second month of her gestation, she started to have brief involuntary jerky movements of the entire body resulting in backward fall. The patient’s consciousness remained intact through the episodes. She continued to experience such episodes about 8-10 per month up to the last trimester. These were suggestive of myoclonic jerks. She was neither a known case of hypertension nor was any recording of increased blood pressure made during pregnancy. She gave birth to a healthy female child on completion of term through a normal vaginal delivery in a primary health care center with no immediate postpartum complications. On Day 12 of the postpartum period, she presented with behavioral changes to a nearby health facility. Her condition deteriorated despite receiving some conservative management over the next ten days and she started to develop spasms with tonic movements of all four limbs and arching of the back both of which were short lived and recurrent. The episodes were aggravated by external stimulus but subsided on its own. Following such presentation, she was referred to our tertiary care center. There was no history of trismus, tongue bite, frothing from mouth, involuntary urination or defecation. History of yellowish discoloration of sclera, decreased urine output, focal neurological deficit or any drug/toxin exposure was absent in the patient. She had no raised blood pressure in any her pregnancies. The patient as a child was a defaulter in receiving all her vaccines including measles. At the age of 12 she was admitted to a health care facility with complaints of fever with rash that subsided on taking medications. No prior history of animal bite, trauma, unexplained weight loss, psychiatric illness in the past was reported.
On general examination, the patient had a Glasgow Coma Scale
(GCS) of E2V2M3 with pulse rate of 120 beats/minute, blood pressure
of 128/74 mm of Hg, a respiratory rate of 28 breaths/minute. Patient
had decerebrate posturing with arching of the back interspersed with
myoclonic spasms. Deep Tendon Reflexes were exaggerated and
bilateral positive Babinski sign. Examination of other systems were
within normal limits.
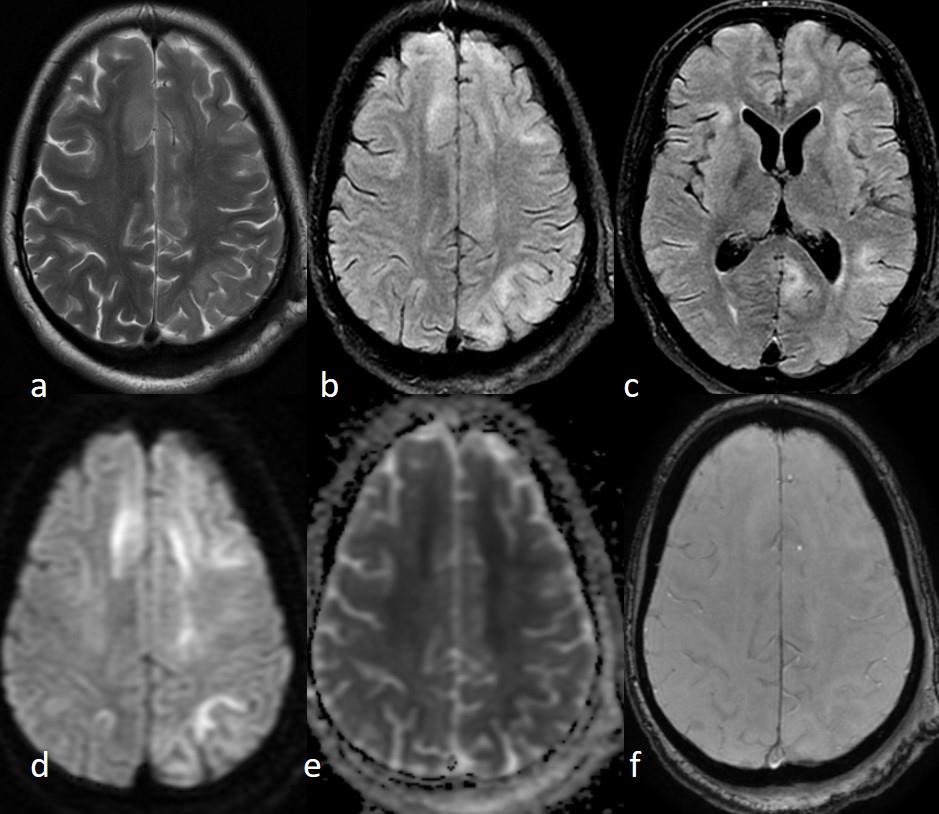
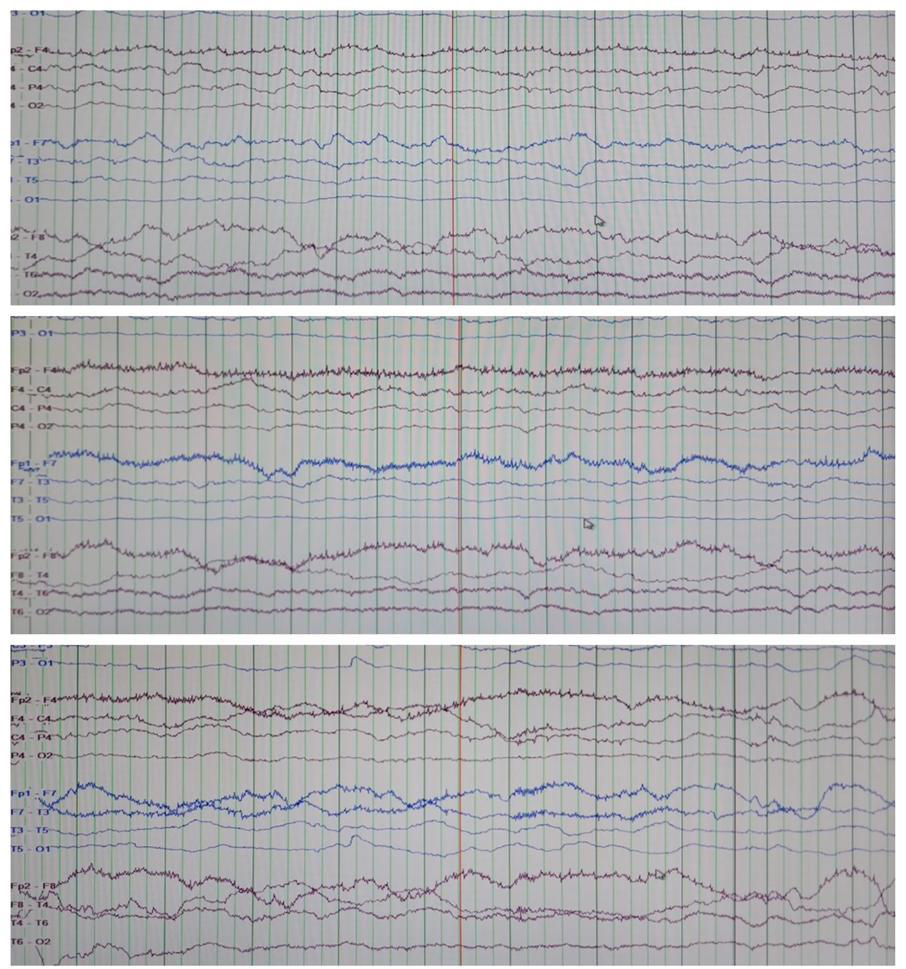
On investigation, CBC showed mild leukocytosis. The fever work-up which included peripheral blood smear to look for malarial parasites, rapid test for Dengue NS 1 antigen, serology for typhoid and paratyphoid causing organisms, blood cultures all of which were negative. The non-contrast enhanced CT scan (NCCT) head was normal. The initial Cerebrospinal fluid (CSF) analysis revealed mildly elevated protein (49.2 mg/dl) with normal cell count (2/mm3) and glucose concentration (67 mg/dl) and no growth on culture. Her CSF autoimmune panel was negative for Anti NMDA, AMPA1 and AMPA2, CASPR, LGI-1 and GABAB receptors. MRI Brain revealed patchy asymmetric confluent T2/FLAIR hyperintensities involving deep and subcortical white matter of bilateral frontal, left parietooccipital, temporal lobe, body and splenium of corpus callosum (Figure1). These findings were suggestive of subacute sclerosing panencephalitis (SSPE). On further workup of the CSF using Enzyme Immunoassay (EIA) confirmed raised anti measles antibody (CSF Ig G level= 298.46 U/ml) and total IgG (CSF total IgG= 22.09). The serology showed parallel results with a raised serum anti measles antibody (Serum IgG measles= 224.62 U/ml). The CSF/Serum quotient was elevated (3.23). The Electroencephalogram (EEG) done for the patient showed generalized background slowing in the deltatheta range. [Figure 2]
On investigation, CBC showed mild leukocytosis. The fever work-up which included peripheral blood smear to look for malarial parasites, rapid test for Dengue NS 1 antigen, serology for typhoid and paratyphoid causing organisms, blood cultures all of which were negative. The non-contrast enhanced CT scan (NCCT) head was normal. The initial Cerebrospinal fluid (CSF) analysis revealed mildly elevated protein (49.2 mg/dl) with normal cell count (2/mm3) and glucose concentration (67 mg/dl) and no growth on culture. Her CSF autoimmune panel was negative for Anti NMDA, AMPA1 and AMPA2, CASPR, LGI-1 and GABAB receptors. MRI Brain revealed patchy asymmetric confluent T2/FLAIR hyperintensities involving deep and subcortical white matter of bilateral frontal, left parietooccipital, temporal lobe, body and splenium of corpus callosum (Figure1). These findings were suggestive of subacute sclerosing panencephalitis (SSPE). On further workup of the CSF using Enzyme Immunoassay (EIA) confirmed raised anti measles antibody (CSF Ig G level= 298.46 U/ml) and total IgG (CSF total IgG= 22.09). The serology showed parallel results with a raised serum anti measles antibody (Serum IgG measles= 224.62 U/ml). The CSF/Serum quotient was elevated (3.23). The Electroencephalogram (EEG) done for the patient showed generalized background slowing in the deltatheta range. [Figure 2]
In view of poor GCS, the patient was intubated. Using biochemical
and clinico-radiological evidences the diagnosis of SSPE was made and
the patient was started on IVIg in the dosage of 2 g/Kg body weight
(BW) in divided doses over 5 days and Isoprinosine in the dosage of
100mg/Kg BW in three divided doses. After 10 days of starting the
medications, the patient started to show signs of improvement as her
myoclonic jerks resolved. She was also able to maintain breathing on
spontaneous ventilator mode and her GCS improved from E2V2M3
to E4VTM4. The patient was monitored in ICU for 2 months during
which her SSPE related symptoms such as the myoclonic jerks,
abnormal posturing had come to halt with low mood and behavioral
changes still persistent but unfortunately, she finally succumbed to
septic shock secondary to ventilator associated pneumonia.
Discussion
We present this case to highlight the challenges a physician
faces while diagnosing and treating the medical conditions whose
manifestation is a rare phenomenon. The case becomes perplexing
when it starts to masquerade disorders of common settings and this
case gives its testimony. The recurrent episodes of involuntary jerky
movements followed by falls on her back persistently with which the
patient was struggling throughout her pregnancy is characteristic of
myoclonic jerks. The presence of tonic movements and spasms of
all four limbs with decorticate posturing reinforces the episodes to
be labelled as myoclonic jerks which were mislabeled as eclampsia.
Therefore, the differentiation between these two clinical entities
becomes significant as the appropriate treatment within stipulated
time is live saving. There have been several recorded cases of SSPE
manifesting during the gestational as well as postpartum period
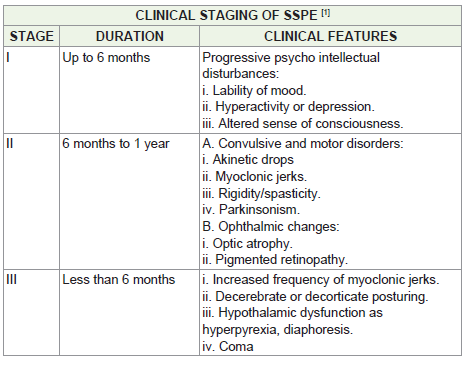
[9]. Furthermore, the suspicion was strengthened as the increase in
frequency of myoclonic jerks interspaced with behavioral changes
and decorticate posturing fall into the clinical staging of SSPE [Table 1].
The persistent and unresolved high-grade fever with negative
infectious and inflammatory markers may be attributed to the
hypothalamic origin of hyperpyrexia.
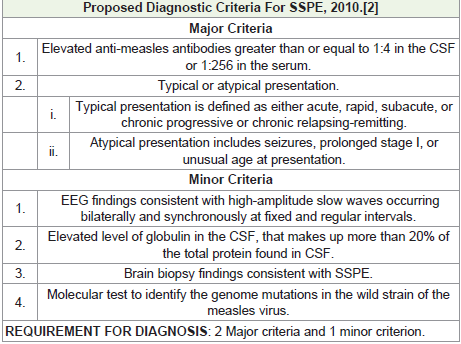
Evaluating for SSPE tends to be multi-faceted. It involves a set of
criteria [Table 2], with brain biopsy being the gold standard. In our
case, the atypical clinical presentation at an unusual age with elevated
serum and CSF anti-measles antibodies and total immunoglobulin
in the CSF, all align with diagnostic criteria [2], thus justifying
the diagnosis of SSPE. The findings on the MRI Brain function as
supporting evidence.
Although there is no documentation of any definitive therapeutic protocol, several treatment options have been used in the hope of halting the disease. Multiple drugs either in isolation or in combinations have been attempted to treat the condition of which Isoprinosine has been garnering a lot of attention. Isoprinosine or Inosine pranobex exerts multimodal actions, including antiviral and immunostimulatory properties.[4] In the largest study of Isoprinosine therapy by the International Consortium on SSPE, it was administered among 98 patients with SSPE, at multiple centers in the United States of America and Canada, with a duration up to 9.5 years. The actuarial probability of survival compared to control at 2, 4, 6, and 8 years was 78, 69, 65, and 61% (compared to 38, 20, 14, and 8%), respectively.[5] Isoprinosine’s beneficial effect on survival and neurological deficiencies has been achieved in one-third of cases of SSPE given at 50–100 mg/ kg/day as a monotherapy or combined treatment with Interferons (IFN) [6] .It has been reported that intraventricular IFN‐α treatment combined with Isoprinosine induced remission or stabilization in 44–55% of SSPE cases.[7] Although, the administration of IVIg in patients of SSPE has not been at par with other modalities in terms of its usage frequency but the results in term of recovery especially in the initial stages of management are worth highlighting. A cohort study reported temporary clinical improvement among patients who received IVIG therapy during the early stages of the disease [8]
Although there is no documentation of any definitive therapeutic protocol, several treatment options have been used in the hope of halting the disease. Multiple drugs either in isolation or in combinations have been attempted to treat the condition of which Isoprinosine has been garnering a lot of attention. Isoprinosine or Inosine pranobex exerts multimodal actions, including antiviral and immunostimulatory properties.[4] In the largest study of Isoprinosine therapy by the International Consortium on SSPE, it was administered among 98 patients with SSPE, at multiple centers in the United States of America and Canada, with a duration up to 9.5 years. The actuarial probability of survival compared to control at 2, 4, 6, and 8 years was 78, 69, 65, and 61% (compared to 38, 20, 14, and 8%), respectively.[5] Isoprinosine’s beneficial effect on survival and neurological deficiencies has been achieved in one-third of cases of SSPE given at 50–100 mg/ kg/day as a monotherapy or combined treatment with Interferons (IFN) [6] .It has been reported that intraventricular IFN‐α treatment combined with Isoprinosine induced remission or stabilization in 44–55% of SSPE cases.[7] Although, the administration of IVIg in patients of SSPE has not been at par with other modalities in terms of its usage frequency but the results in term of recovery especially in the initial stages of management are worth highlighting. A cohort study reported temporary clinical improvement among patients who received IVIG therapy during the early stages of the disease [8]
Along with the available literature on the treatment aspect of
SSPE, the possibility of autoimmunity being the underlying culprit
was also taken into consideration as the patient was a young female
with infective causes ruled out through CSF studies and also gave
history of perioral contraction and flickering. Therefore, in our case
patient was started on IVIg in the dosage of 2 g/Kg BW in over 5 days
and Isoprinosine in the dosage of 100mg/Kg BW/day. On the first
day of presentation, the patient was in stage III SSPE characterized
by myoclonic jerks, decorticate posturing, and hypothalamic
dysfunctions on Synchronized Intermittent Mandatory Ventilation
(SIMV) mode. On the 10th day of management, the patient started to
show signs of improvement as her myoclonic jerks resolved. She was
also able to maintain breathing on spontaneous ventilator mode and
her GCS improved from E2V2M1 to E4VTM4. The choice of treatment
modality chosen in this case can be labeled as a novel approach as the
combination of IVIg along with Isoprinosine has not been attempted
widely for cases of SSPE. As the patient finally succumbed to hospital
acquired pneumonia before coming back to her apparent state of
health prior to SSPE, therefore labelling the regimen described above
as the absolute treatment for SSPE lacks credibility as far as this case
is concerned. Although the regimen did produce significant effect in
controlling further progression of the disease.
Therefore, the early diagnosis and management using the regimen
not only promises hope for future trials for a standardized treatment
protocol for the disease but shall be an aid in devising a holistic
approach for the improvement in quality of life of such patients.
Conclusion and Clinical Significance
This case report highlights the challenges of diagnosing subacute
sclerosing panencephalitis in an atypical presentation. The patient’s
unusual age and clinical features led to a delay in diagnosis but a novel
combination of IVIg and Isoprinosine resulted in significant clinical
improvement. This case emphasizes the importance of maintaining a
broad differential diagnosis and increased awareness of SSPE. Early
diagnosis and innovative treatment strategies are crucial to improve
outcomes in this rare and debilitating disease. This report contributes
to the limited literature on SSPE.
Conflict of Interests:
The authors declare that they have no known competing financial
interests or personal relationships that could have appeared to
influence the work reported in this paper.Ethical Compliance:
All procedures performed in studies involving human participants
were in accordance with the ethical standards of the institutional and/
or national research committee and with the 1964 Helsinki Declaration
and its later amendments or comparable ethical standards.Conflict of Interest declaration:
The authors declare that they have no affiliations with or
involvement in any organization or entity with any financial interest
in the subject matter or materials discussed in this manuscript. The
authors have no conflicts of interest to declare.Consent:
Written and Informed consent of the patient and all authors were
taken for publication of this case.References
Citation
Paul S, Jain B, Paikray S, Chauhan RS, Siddiqui MS, et al. Subacute Sclerosing Panencephalitis Masquerading as eclampsia: A Case Report and Review of Literature. Indian J Neurol. 2025;6(1): 158.