Case Report
Focal Encephalocele Secondary to Type II Sternberg ’s Canal Defect –A Rare Phenomenon
Mohammed A* and Shastry GN
Department of General Medicine, Kanachur Institute of Medical Sciences, Mangalore, Karnataka, India
*Corresponding author: Dr. Arfaz Mohammed, Postgraduate Resident, Department of General Medicine, Kanachur Institute of Medical Sciences, Mangalore, Karnataka, India. E-mail Id: drarfazmd@gmail.com
Article Information: Submission: 28/08/2025; Accepted: 17/09/2025; Published: 19/09/2025
Copyright: © 2025 Mohammed A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Sternberg’s canal (lateral craniopharyngeal canal) is an embryonic remnant from incomplete fusion of the greater wings of the sphenoid with the basisphen oid, potentially predisposing to temporal lobe encephaloceles into the sphenoid sinus. The complications seen in this condition are CSF rhinorrhea, recurrent meningitis, seizures, misdiagnosed nasal mass.
Case Presentation: A 23‑year‑old male experienced recurrent headaches for one year, initially treated as vascular headache without relief. CT brain revealed focal thinning of the left sphenoid sinus superolateral wall. MRI demonstrated a focal encephalocele abutting the infraorbital segment of the optic n erve, consistent with a Type II Sternberg’s canal defect. This patient was treated with surgical repair.
Discussion: Four types of sphenoid sinus defects are recognized based on location related to the foramen rotundum (FR) and vidian canal (VC)—Type II defects are medial to FR and are rare. Radiological imaging (CT and MRI) is essential for accurate diagnosis and surgical planning. Treatment could be conservative by using a temporary lumbar drain for small leaks or surgical management can be done by e ndoscopic endonasal repair or open transcranial repair. While most focal encephaloceles due to Sternberg ’s canal defect are isolated, they can be associated with neurocutaneous syndromes like NF1 (sphenoid wing dysplasia with basal encephalocele).
Conclusion: Type II Sternberg’s canal defects, though rare, should be considered in unexplained chronic headaches or spontaneous CSF rhinorrhea. Early imaging facilitates diagnosis and guides neurosurgical intervention.
Case Presentation: A 23‑year‑old male experienced recurrent headaches for one year, initially treated as vascular headache without relief. CT brain revealed focal thinning of the left sphenoid sinus superolateral wall. MRI demonstrated a focal encephalocele abutting the infraorbital segment of the optic n erve, consistent with a Type II Sternberg’s canal defect. This patient was treated with surgical repair.
Discussion: Four types of sphenoid sinus defects are recognized based on location related to the foramen rotundum (FR) and vidian canal (VC)—Type II defects are medial to FR and are rare. Radiological imaging (CT and MRI) is essential for accurate diagnosis and surgical planning. Treatment could be conservative by using a temporary lumbar drain for small leaks or surgical management can be done by e ndoscopic endonasal repair or open transcranial repair. While most focal encephaloceles due to Sternberg ’s canal defect are isolated, they can be associated with neurocutaneous syndromes like NF1 (sphenoid wing dysplasia with basal encephalocele).
Conclusion: Type II Sternberg’s canal defects, though rare, should be considered in unexplained chronic headaches or spontaneous CSF rhinorrhea. Early imaging facilitates diagnosis and guides neurosurgical intervention.
Keywords:Sternberg’s canal, encephalocele, sphenoid sinus, CSF leak, headache
Introduction
Sternberg’s canal, also known as the lateral craniopharyngeal
canal, results from the incomplete fusion of sphenoid ossification
centers and may serve as a weak point in the skull base, predisposing
to her niation of the temporal lobe into the sphenoid sinus. While
historically reported in up to 4% of adults, more recent imaging
studies suggest the incidence is significantly lower. Clinically,
patients may present with spontaneous CSF rhinorrhea, recurrent m
eningitis, or headache. The complications seen in this condition are
CSF rhinorrhea, recurrent meningitis, seizures, misdiagnosed nasal
mass.
Case Report
A 23‑year‑old male without comorbidities presented with
recurrent headaches for one year; these were initially attributed to
vascular headache and failed to respond to treatment.
Investigations
• CT Brain:
Investigations
• CT Brain:
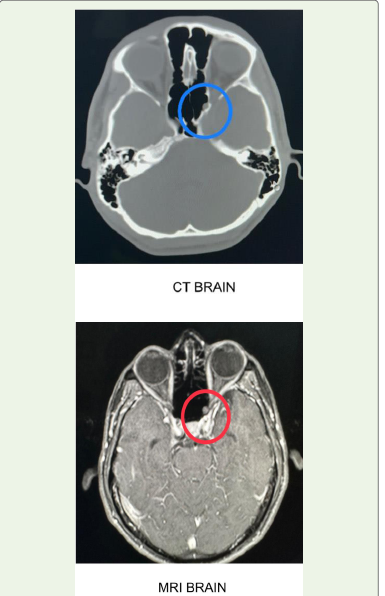
Revealed focal thinning and defect in the superolateral wall of the
left sphenoid sinus.
• MRI Brain:
Demonstrated encephalocele abutting the infraorbital optic nerve segment, consistent with a Type II Sternberg’s canal defect.
This patient chose surgical correction and underwent the same
• MRI Brain:
Demonstrated encephalocele abutting the infraorbital optic nerve segment, consistent with a Type II Sternberg’s canal defect.
This patient chose surgical correction and underwent the same
Discussion
Sphenoid sinus encephaloceles due to persistence of Sternberg’s
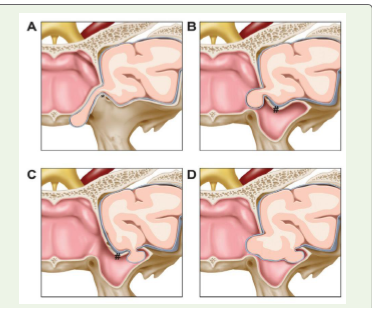
canal are exceedingly rare. Classification based on relation to FR and
VC:
- Type I: Medial to FR and VC (traditional Sternberg’s canal)
- Type II: Medial to FR
- Type III: Lateral to FR
- Type IV: Through enlarged FR into sphenoid sinus
Treatment could be conservative by using a temporary lumbar drain for small leaks or surgical management can be done by endoscopic endonasal repair or open transcranial repai r. While most focal encephaloceles due to Sternberg ’s canal defect are isolated, they can be associated with neurocutaneous syndromes like NF1 (sphenoid wing dysplasia with basal encephalocele).
Our case corresponds to a Type II defect, which is rarely r eported. Clinically, patients may present with CSF rhinorrhea, recurrent meningitis, visual disturbances, or persistent headaches. Radiological imaging with CT and MRI is essential for diagnosis, anatomical localization, and surgical planning.
- Type I: Medial to FR and VC (traditional Sternberg’s canal)
- Type II: Medial to FR
- Type III: Lateral to FR
- Type IV: Through enlarged FR into sphenoid sinus
Treatment could be conservative by using a temporary lumbar drain for small leaks or surgical management can be done by endoscopic endonasal repair or open transcranial repai r. While most focal encephaloceles due to Sternberg ’s canal defect are isolated, they can be associated with neurocutaneous syndromes like NF1 (sphenoid wing dysplasia with basal encephalocele).
Our case corresponds to a Type II defect, which is rarely r eported. Clinically, patients may present with CSF rhinorrhea, recurrent meningitis, visual disturbances, or persistent headaches. Radiological imaging with CT and MRI is essential for diagnosis, anatomical localization, and surgical planning.
Conclusion
Type II Sternberg’s canal defect represents a rare anatomical
variant that may manifest as chronic headaches or CSF leak.
Accurate diagnosis rests on high -resolution CT and MRI.
Prompt recognition and intervention are critical to prevent
complications like meningitis and to guide appropriate surgical repair.
References
Citation
Mohammed A, Shastry GN. Focal Encephalocele Secondary to Type II Sternberg ’s Canal Defect –A Rare Phenomenon. Indian J Neurol. 2025;6(1): 157.