Research Article
Prevalence of Subjective Cognitive Decline and its Associated Factors in Adults Aged 30 and Above in an Underprivileged Urban Area of Delhi, India
Mondal A1, Bansal K2, Santra S1, Kumar A1, Jain S1, Gupta S1, Sahil Ahuja1, Srivastava N1, and Virender Prakash Gautam1*
1Department of Community Medicine, Vardhman Mahavir Medical College and Safdarjung Hospital
2Johns Hopkins Bloomberg School of Public Health
2Johns Hopkins Bloomberg School of Public Health
*Corresponding author:Dr. Virender Prakash Gautam, Department of Community Medicine, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India. E-mail Id: drvpgautam@vmmc-sjh.nic.in
Article Information: Submission: 20/08/2025; Accepted: 12/09/2025; Published: 16/09/2025
Copyright: © 2025 Mondal A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background and Objectives: Subjective cognitive decline (SCD) is an early warning sign of dementia and a significant contributor to disability among older adults. There is a lack of research on SCD among adults aged 30 years and above in urban underprivileged populations in North India. This study aimed to estimate the prevalence of SCD and examine its associations with socio-demographic and health-related factors.
Methods: A cross-sectional study was conducted among 350 adults aged ≥30 years residing in a North Indian urban underprivileged community. SCD was assessed using the SCD-Q21 scale. Socio-demographic and co-morbidity data were obtained via a structured questionnaire. Associations were examined through chi-square test and multiple logistic regression analyses.
Results: SCD was present in 83 participants (23.7%). Prevalence was higher among illiterate individuals compared to those with higher education (34.2% vs. 13.8%) and among participants with co-morbidities versus those without (42.3% vs. 12.8%). Marital status was significantly associated with SCD (p < 0.001). In adjusted analyses, being unmarried (or corresponding marital status) was independently associated with higher odds of SCD (Adjusted OR, 3.24; 95% CI, 1.52–5.79), as was the presence of co‑morbid conditions (Adjusted OR, 3.08; 95% CI, 1.70–5.58).
Conclusions: Nearly one in four adults aged ≥30 years in this underprivileged urban setting report SCD. Given SCD’s potential progression to dementia, early routine screening particularly for unmarried individuals and those with co‑morbidities could enable preventive strategies to mitigate cognitive decline later in life.
Methods: A cross-sectional study was conducted among 350 adults aged ≥30 years residing in a North Indian urban underprivileged community. SCD was assessed using the SCD-Q21 scale. Socio-demographic and co-morbidity data were obtained via a structured questionnaire. Associations were examined through chi-square test and multiple logistic regression analyses.
Results: SCD was present in 83 participants (23.7%). Prevalence was higher among illiterate individuals compared to those with higher education (34.2% vs. 13.8%) and among participants with co-morbidities versus those without (42.3% vs. 12.8%). Marital status was significantly associated with SCD (p < 0.001). In adjusted analyses, being unmarried (or corresponding marital status) was independently associated with higher odds of SCD (Adjusted OR, 3.24; 95% CI, 1.52–5.79), as was the presence of co‑morbid conditions (Adjusted OR, 3.08; 95% CI, 1.70–5.58).
Conclusions: Nearly one in four adults aged ≥30 years in this underprivileged urban setting report SCD. Given SCD’s potential progression to dementia, early routine screening particularly for unmarried individuals and those with co‑morbidities could enable preventive strategies to mitigate cognitive decline later in life.
Keywords: Subjective cognitive decline; dementia precursor; SCD Q21 scale
Introduction
Cognition encompasses a range of mental processes, including
learning, memory, attention, and judgment, all of which are essential
for an individual’s daily functioning and overall quality of life. In
recent years, growing attention has been directed toward individuals
who report cognitive concerns—particularly memory-related
issues—despite exhibiting normal performance on standardized
neuropsychological assessments. This condition is known as
Subjective Cognitive Decline (SCD). [1,2]
SCD is characterized by a self-perceived experience of worsening
or more frequent episodes of memory loss or confusion in the absence
of measurable cognitive impairment on clinical testing.[3] Although
it is not a clinical diagnosis in itself, SCD is increasingly regarded as a
potential early manifestation of neurodegenerative disorders such as
Alzheimer’s disease. [4]
In India, the estimated prevalence of dementia among adults aged
≥60 years is 7.4%, with approximately 3 million people affected by
Alzheimer’s disease. [5,6] These statistics highlight the urgency of
early identification and management of cognitive decline to reduce
the associated healthcare burden. As a possible precursor to dementia,
SCD may play a crucial role in detecting neurodegeneration at an
earlier, more manageable stage potentially delaying its onset through
targeted interventions. [4,7]
Most studies on SCD have focused on individuals aged 60 years
and above, a group already at significant risk for Alzheimer’s disease
and related dementias.[8] However, rehabilitative interventions at
later stages often yield limited success.[9] There is a clear research
gap regarding SCD in younger populations, particularly in India.
Exploring SCD among adults aged 30 years and above, many of
whom are still in their productive years, could offer critical insights
into early prevention and promote healthy ageing across the life
course.[10]
Given the paucity of literature on SCD in younger adults within low-resource settings, this study was undertaken to estimate the prevalence of SCD and its associated factors among adults aged ≥30 years residing in an underprivileged urban area of Delhi. This setting presents unique challenges and valuable opportunities for improving the understanding of cognitive health in socioeconomically disadvantaged populations.
Given the paucity of literature on SCD in younger adults within low-resource settings, this study was undertaken to estimate the prevalence of SCD and its associated factors among adults aged ≥30 years residing in an underprivileged urban area of Delhi. This setting presents unique challenges and valuable opportunities for improving the understanding of cognitive health in socioeconomically disadvantaged populations.
Methodology
This was a community-based cross-sectional study conducted in
an underprivileged urban area of Delhi, India. The study population
consisted of adults aged ≥30 years residing in the area. A sampling
frame comprising individuals aged ≥30 years was prepared, and
participants were selected using simple random sampling.
Adults aged ≥30 years who were permanent residents of the study area were eligible for inclusion. Participants were excluded if they had a prior clinical diagnosis of cognitive impairment or mental illness, or they were unable to comprehend and respond to the questionnaire due to debilitating conditions or severe illness.
Adults aged ≥30 years who were permanent residents of the study area were eligible for inclusion. Participants were excluded if they had a prior clinical diagnosis of cognitive impairment or mental illness, or they were unable to comprehend and respond to the questionnaire due to debilitating conditions or severe illness.
The sample size was calculated based on a reported SCD
prevalence of 22.8% from a previous study by Narayanaswamy et al.
[11] Using the formula: 4PQ/L2, where P=22.8%, Q=77.2% (100-P),
and L=4.56 (20% of P), the required sample size was calculated to be
338.65. This was rounded to 350 to account for a 5% non-response
rate.
Data were collected using the SCD-Q21 scale, a validated questionnaire designed to assess SCD.[12] The tool was translated into Hindi and pilot-tested on 35 individuals (10% of the sample size) who were not included in the final analysis. The questionnaire also included sections on socio-demographic variables, selected lifestyle and health-related factors, and the presence of co-morbidities.
Trained field investigators conducted face-to-face interviews with participants at their residences. If a participant was unavailable during the initial visit, a second visit was made on the following day. Participants who could not be contacted after two visits were replaced through random selection from the remaining sampling frame until the desired sample size was achieved.
Data were entered and cleaned using Microsoft Excel and analyzed using IBM SPSS Statistics (v. 25). Categorical variables were summarized as frequencies and percentages, while continuous variables were presented as mean ± standard deviation. The chi-square test was used for analyzing associations between categorical variables, and the student’s t-test was applied to compare means of continuous variables. Multiple logistic regression analysis was performed to identify factors independently associated with SCD. Both crude and adjusted odds ratios (OR) with 95% confidence intervals (CI) were reported.
Data were collected using the SCD-Q21 scale, a validated questionnaire designed to assess SCD.[12] The tool was translated into Hindi and pilot-tested on 35 individuals (10% of the sample size) who were not included in the final analysis. The questionnaire also included sections on socio-demographic variables, selected lifestyle and health-related factors, and the presence of co-morbidities.
Trained field investigators conducted face-to-face interviews with participants at their residences. If a participant was unavailable during the initial visit, a second visit was made on the following day. Participants who could not be contacted after two visits were replaced through random selection from the remaining sampling frame until the desired sample size was achieved.
Data were entered and cleaned using Microsoft Excel and analyzed using IBM SPSS Statistics (v. 25). Categorical variables were summarized as frequencies and percentages, while continuous variables were presented as mean ± standard deviation. The chi-square test was used for analyzing associations between categorical variables, and the student’s t-test was applied to compare means of continuous variables. Multiple logistic regression analysis was performed to identify factors independently associated with SCD. Both crude and adjusted odds ratios (OR) with 95% confidence intervals (CI) were reported.
Ethical approval for the study was obtained from the Institutional
Ethics Committee. Participants were fully informed about the
study objectives and assured of their right to withdraw at any stage
without consequences. Written informed consent was obtained from
all participants. Confidentiality and anonymity were maintained
throughout the study.
Results
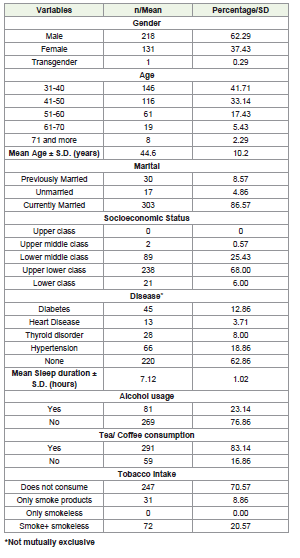
A total of 350 participants were included in the study. The
majority were in the age group of 31–40 years (n = 146, 41.71%),
followed by 41–50 years (n = 116, 33.14%). Most participants were
male (n = 218, 62.29%) and currently married (n = 303, 86.57%),
while 30 participants (8.57%) were previously married.
[Table 1]
In terms of socioeconomic status (based on the Revised Modified Kuppuswamy Scale, 2023), most participants belonged to the upperlower class (n = 238, 68.00%) and lower-middle class (n = 89, 25.43%). Commonly reported co-morbid conditions included hypertension (n = 66, 18.86%) and diabetes (n = 45, 12.86%), while a majority reported no known health issues (n = 220, 62.86%). (Table 1)
With respect to lifestyle behaviors, 291 participants (83.14%) reported regular consumption of tea or coffee, 81 (23.14%) consumed alcohol, and 247 (70.57%) reported not using any tobacco products. [Table 1]
In terms of socioeconomic status (based on the Revised Modified Kuppuswamy Scale, 2023), most participants belonged to the upperlower class (n = 238, 68.00%) and lower-middle class (n = 89, 25.43%). Commonly reported co-morbid conditions included hypertension (n = 66, 18.86%) and diabetes (n = 45, 12.86%), while a majority reported no known health issues (n = 220, 62.86%). (Table 1)
With respect to lifestyle behaviors, 291 participants (83.14%) reported regular consumption of tea or coffee, 81 (23.14%) consumed alcohol, and 247 (70.57%) reported not using any tobacco products. [Table 1]
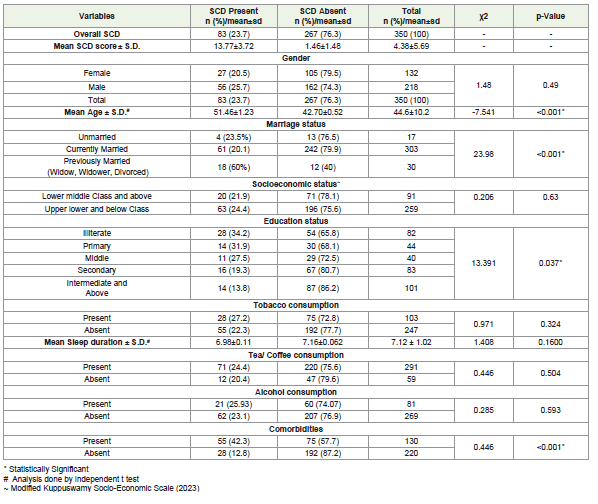
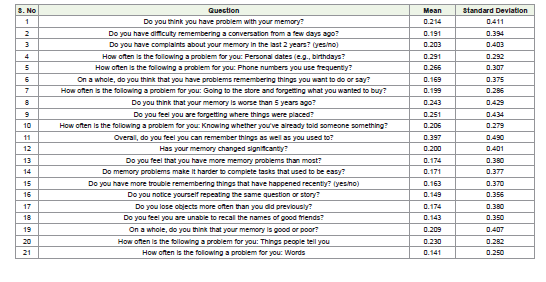
SCD was observed in 83 participants (23.7%). Detailed item-wise
responses from the SCD-Q21 scale are presented in [Table 2].
SCD was found to be significantly associated with age, marital status, education level, and presence of co-morbidities. The mean age of participants with SCD was significantly higher (51.46 ± 1.23 years) compared to those without SCD (42.70 ± 0.52 years) (p < 0.001). Marital status was significantly associated with SCD (p < 0.001), with the highest prevalence among previously married individuals (60.0%), followed by unmarried (23.5%) and currently married (20.1%) participants. Education level also showed a significant association (p = 0.037), with higher prevalence among illiterate participants (34.2%)
SCD was found to be significantly associated with age, marital status, education level, and presence of co-morbidities. The mean age of participants with SCD was significantly higher (51.46 ± 1.23 years) compared to those without SCD (42.70 ± 0.52 years) (p < 0.001). Marital status was significantly associated with SCD (p < 0.001), with the highest prevalence among previously married individuals (60.0%), followed by unmarried (23.5%) and currently married (20.1%) participants. Education level also showed a significant association (p = 0.037), with higher prevalence among illiterate participants (34.2%)
compared to those with higher education (13.8%). Participants with
co-morbidities had a significantly higher prevalence of SCD (42.3%)
than those without (12.8%) (p < 0.001).
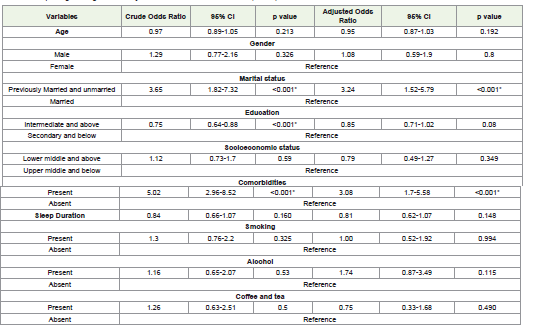
After adjusting for potential confounders, marital status and comorbidities remained significantly associated with SCD. Previously married individuals had significantly higher odds of SCD with crude OR = 3.65 (95% CI: 1.82–7.32, p < 0.001) and adjusted OR = 3.24 (95% CI: 1.52–5.79, p < 0.001).
Also, participants with co-morbidities also had higher odds of SCD with crude OR = 5.02 (95% CI: 2.96–8.52, p < 0.001) and adjusted OR = 3.08 (95% CI: 1.70–5.58, p < 0.001). Other factors— including age, education level, socioeconomic status, tobacco use, alcohol consumption, and caffeine intake—did not show statistically significant associations in the multiple logistic regression analysis. [Table 3]
After adjusting for potential confounders, marital status and comorbidities remained significantly associated with SCD. Previously married individuals had significantly higher odds of SCD with crude OR = 3.65 (95% CI: 1.82–7.32, p < 0.001) and adjusted OR = 3.24 (95% CI: 1.52–5.79, p < 0.001).
Also, participants with co-morbidities also had higher odds of SCD with crude OR = 5.02 (95% CI: 2.96–8.52, p < 0.001) and adjusted OR = 3.08 (95% CI: 1.70–5.58, p < 0.001). Other factors— including age, education level, socioeconomic status, tobacco use, alcohol consumption, and caffeine intake—did not show statistically significant associations in the multiple logistic regression analysis. [Table 3]
Discussion
This community-based study was conducted among 350 adults
aged ≥30 years residing in an underprivileged urban area of Delhi,
India. The mean age of the participants was 44.6 years, with a majority
being male (62.29%) and currently married (86.57%). While existing
literature has primarily focused on SCD prevalence in individuals
aged ≥60 years, with some extending the lower limit to 45 years,
this study is, to the best of our knowledge, the first to assess SCD
prevalence in adults aged ≥30 years in North India. [5,9,11,13]
We found the prevalence of SCD to be 23.7%, which is comparable to findings from other regions of India such as Bangalore (22.8%) and Karnataka (21.5%), and also to international studies conducted in Korea (17.4%–29.4%), China (18.8%), and in pooled global cohort data (25.6%).[11,14-16] A notably higher prevalence (45.2%) was reported in a study from Chennai, where participants were recruited from elderly care homes, hospitals, and health camps; the higher burden of co-morbidities in that population (e.g., >50% with diabetes or hypertension) may partly explain the increased SCD prevalence, compared to the present study, where 12.86% had diabetes and 18.86% had hypertension.[13]
Consistent with our findings, multiple studies have reported a significant association between SCD and various co-morbidities, including diabetes, ischaemic heart disease, thyroid disorders, anaemia, and gout.[17-19] A study from Italy also revealed that co-morbidities exert a mild but measurable effect on cognitive functioning.[20] In our study, participants with co-morbidities had over three times higher adjusted odds of experiencing SCD, reinforcing the need to consider co-morbidity as a key risk factor.
Marital status also emerged as a significant determinant of SCD. Participants who were previously married (divorced, separated, or widowed) had significantly higher odds of SCD, which aligns with findings by Roh et al.[17] In contrast, studies by Menon J et al and Lin et al did not find significant associations between marital status or co-morbidities and cognitive impairment.[13,19] However, these discrepancies may be attributed to methodological differences particularly the lack of adjustment for confounders in the former and limited covariate adjustment in the latter.
We found the prevalence of SCD to be 23.7%, which is comparable to findings from other regions of India such as Bangalore (22.8%) and Karnataka (21.5%), and also to international studies conducted in Korea (17.4%–29.4%), China (18.8%), and in pooled global cohort data (25.6%).[11,14-16] A notably higher prevalence (45.2%) was reported in a study from Chennai, where participants were recruited from elderly care homes, hospitals, and health camps; the higher burden of co-morbidities in that population (e.g., >50% with diabetes or hypertension) may partly explain the increased SCD prevalence, compared to the present study, where 12.86% had diabetes and 18.86% had hypertension.[13]
Consistent with our findings, multiple studies have reported a significant association between SCD and various co-morbidities, including diabetes, ischaemic heart disease, thyroid disorders, anaemia, and gout.[17-19] A study from Italy also revealed that co-morbidities exert a mild but measurable effect on cognitive functioning.[20] In our study, participants with co-morbidities had over three times higher adjusted odds of experiencing SCD, reinforcing the need to consider co-morbidity as a key risk factor.
Marital status also emerged as a significant determinant of SCD. Participants who were previously married (divorced, separated, or widowed) had significantly higher odds of SCD, which aligns with findings by Roh et al.[17] In contrast, studies by Menon J et al and Lin et al did not find significant associations between marital status or co-morbidities and cognitive impairment.[13,19] However, these discrepancies may be attributed to methodological differences particularly the lack of adjustment for confounders in the former and limited covariate adjustment in the latter.
Like previous studies, in the present study, people with higher
education had lower odds of having SCD, although this association
no longer remained significant after adjusting for confounders.
[13,16,19] This indicates that different levels of educational attainment
may cause differences in SCD prevalence.
Although a higher proportion of males than females had SCD in our study, gender, age, and socioeconomic status were not statistically significant factors; this is supported by other studies in both Indian and international settings.[13,16-18] Lifestyle factors such as alcohol consumption, tobacco use, tea/coffee intake, and sleep duration were also not associated with SCD, which is consistent with prior studies. [19,21] However, Roh et al reported an association between alcohol use, female gender, and increased odds of SCD in a Korean cohort indicating possible cultural or demographic variations in risk factors. [17]
Regarding education, individuals with higher educational attainment exhibited a lower prevalence of SCD in bivariate analysis, although the association lost statistical significance in multiple logistic regression analysis. Similar trend has been observed in other studies as well, supports the cognitive reserve hypothesis, wherein education may offer a protective buffer against early cognitive decline. [13,16,19]
Although a higher proportion of males than females had SCD in our study, gender, age, and socioeconomic status were not statistically significant factors; this is supported by other studies in both Indian and international settings.[13,16-18] Lifestyle factors such as alcohol consumption, tobacco use, tea/coffee intake, and sleep duration were also not associated with SCD, which is consistent with prior studies. [19,21] However, Roh et al reported an association between alcohol use, female gender, and increased odds of SCD in a Korean cohort indicating possible cultural or demographic variations in risk factors. [17]
Regarding education, individuals with higher educational attainment exhibited a lower prevalence of SCD in bivariate analysis, although the association lost statistical significance in multiple logistic regression analysis. Similar trend has been observed in other studies as well, supports the cognitive reserve hypothesis, wherein education may offer a protective buffer against early cognitive decline. [13,16,19]
Conclusion
This study highlights a significant prevalence of SCD amongst
adults aged ≥30 years in an underprivileged urban area of Delhi.
Co-morbidities, especially diabetes and hypertension, were
strongly associated with SCD. Marital status, particularly being
previously married, was another key determinant. The rapid rise
of noncommunicable diseases and marital separation may further
exacerbate the risk of SCD. As SCD is an early indicator of dementia,
implementing early screening and targeted interventions focusing
on co-morbid conditions and social factors in socioeconomically
disadvantaged areas could delay or prevent the onset of dementia,
promoting healthier ageing outcomes. Addressing these risk factors
is crucial for improving public health in vulnerable populations.
References
Citation
Mondal A, Bansal K, Santra S, Kumar A, Jain S, et al. Prevalence of Subjective Cognitive Decline and its Associated Factors in Adults Aged 30 and Above in an Underprivileged Urban Area of Delhi, India. Indian J Neurol. 2025;6(1): 156.