Case Report
Morvan Syndrome with CASPR2 and LGI1 Positivity Triggered by Anabolic Steroid Exposure: A Case Report
Sai Bharath BV*, Saroja AO, Naik KR and Sumanth CV
Department of Neurology, Jawaharlal Nehru Medical College, Belagavi, Karnataka, India
*Corresponding author:Dr. Venkata Sai Bharath, Boyina, Department of Neurology, Jawaharlal Nehru Medical College, Belagavi, Karnataka, India. Email Id: boyinasaibharath158@gmail.com
Article Information:Submission: 04/08/2025; Accepted: 09/09/2025; Published: 11/09/2025
Copyright: © 2025 Sai Bharath BV, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Morvan syndrome is a rare autoimmune disorder involving both peripheral and central nervous systems. Patients typically present with continuous muscle twitching (myokymia), cramps, stiffness, fasciculations and autonomic dysfunction including hyperhidrosis, arrhythmias and blood pressure instability. Central nervous system involvement manifests as insomnia, psychiatric symptoms, memory impairment, and occasionally seizures. We report a 27-yearold man who presented with insomnia, severe myalgia, generalized myokymia, autonomic instability, and anxiety following anabolic steroid use. Nerve conductions revealed repetitive after-discharges and needle electromyography revealed myokymic discharges. Serum was strong positivity for CASPR2 and weak positivity for LGI [1] antibodies. The patient responded well to corticosteroids and intravenous immunoglobulin. This case report highlights a rare autoimmune neurological syndrome potentially triggered by anabolic steroid exposure.
Keywords:Morvan syndrome; CASPR2; Neuromyotonia; Anabolic steroids
Introduction
Morvan syndrome is a rare autoimmune neurological disorder
characterized by peripheral nerve hyperexcitability, autonomic
instability, and encephalopathy. It is often associated with antibodies
to voltage-gated potassium channel complex (VGKC) proteins,
including CASPR2 and LGI [1]. Morvan syndrome features
pronounced peripheral nerve hyperexcitability, clinically manifesting
as neuromyotonia. Patients often experience spontaneous muscle
twitching (myokymia), muscle cramps, stiffness, and fasciculations.1
Autonomic dysfunction is one of the hallmark features of
Morvan syndrome and include hyperhidrosis and cardiovascular
dysregulation such as tachycardia, bradycardia, or labile blood
pressure.[2] Central nervous system manifestations include severe
insomnia and increased psychomotor activity, often described as
“agrypnia excitata”—a state of extreme and persistent sleeplessness
with psychomotor and autonomic hyperactivity. Other features
include hallucinations, confusion, agitation, irritability, psychosis,
seizures, cognitive deficits and memory impairment.[3] Anabolic
steroids may modulate immune responses and have been speculated
to predispose susceptible individuals to autoimmune conditions and
can also cause neuroexcitotoxicity and neuronal degeneration when
given in supraphysiological doses.[4]
Case Report
A 27-year-old man presented with progressive severe
generalized myalgia, paraspinal pain, excessive sweating, anxiety,
and insomnia for 2 months. Twenty days before admission, he
developed multifocal twitching of limb muscles at rest. He had a
History of anabolic steroid intake 10 weeks preceding the symptom
onset. There were no other neurological or systemic symptoms.
He had resting tachycardia (115/minute), normal blood pressure
and hyperhidrosis. Cognitive functions, cranial nerves, and
sensations were normal. Muscle strength, bulk, and reflexes were
normal. Myokymia was present in limb muscles (lower > upper limb
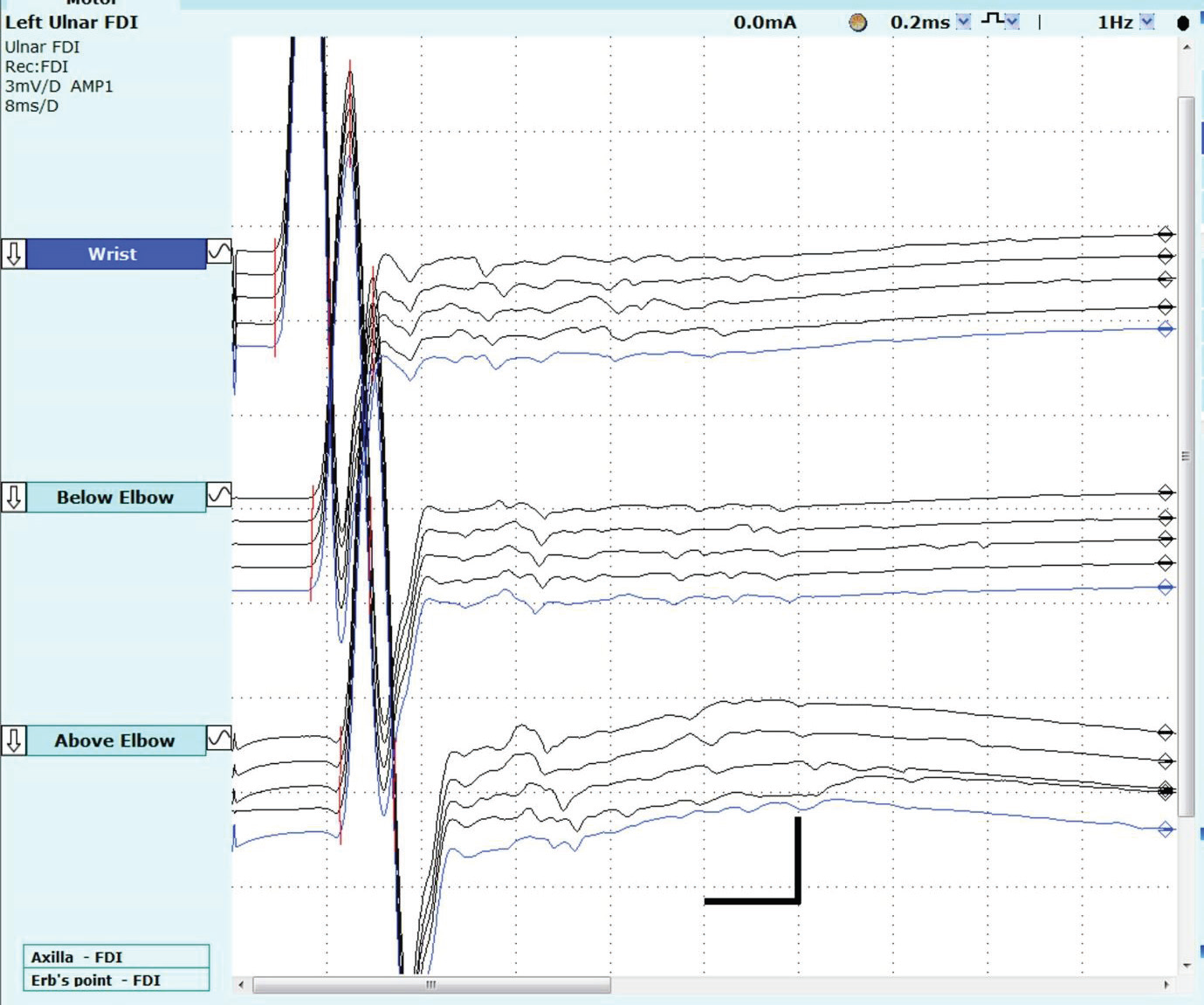
muscles). Motor and sensory nerve conduction parameters were
normal. However, after-discharges were seen following compound
muscle action potentials in median, ulnar, fibular and posterior tibial
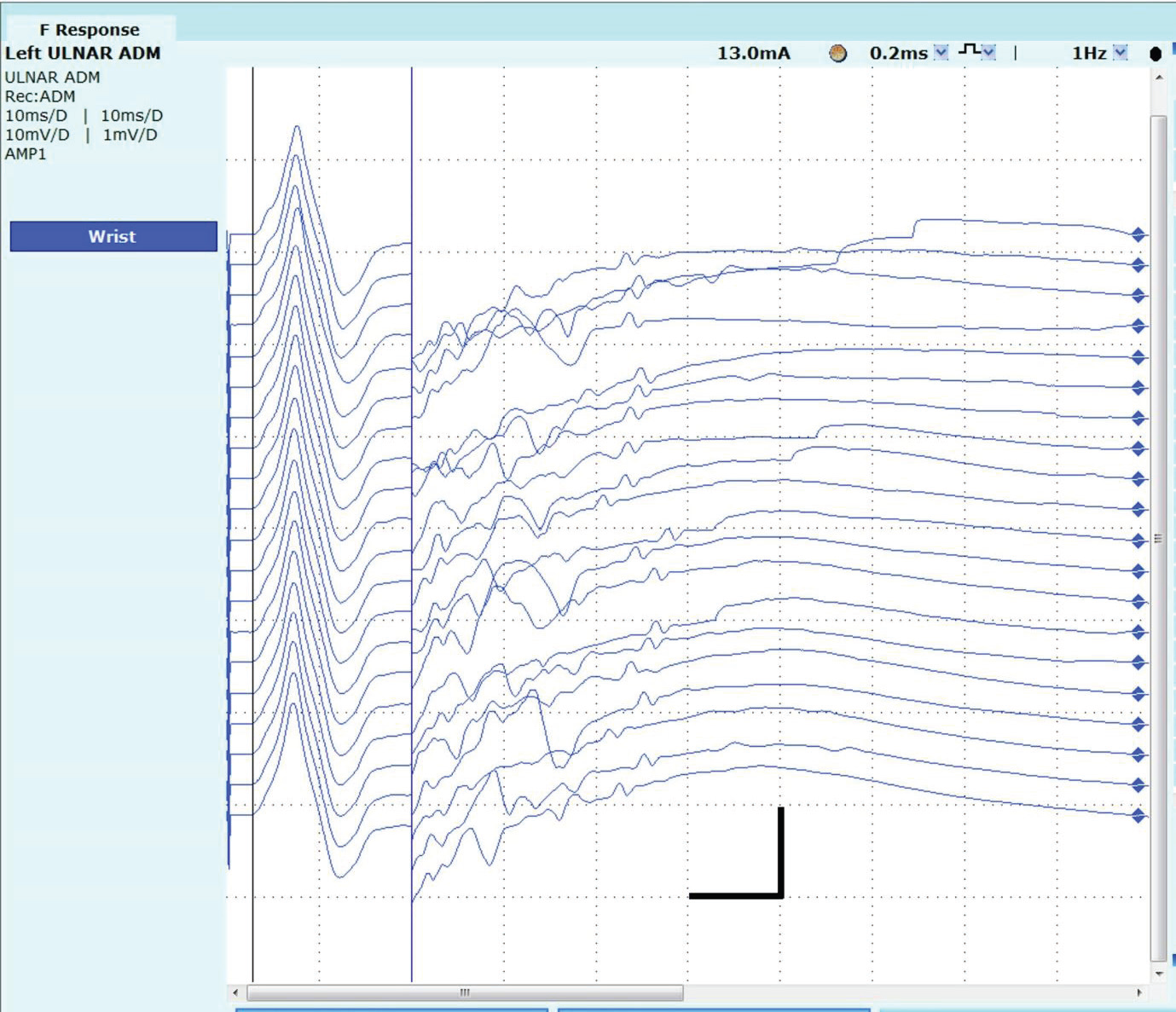
motor nerve conductions.[Figure 1] F – waves could not be identified
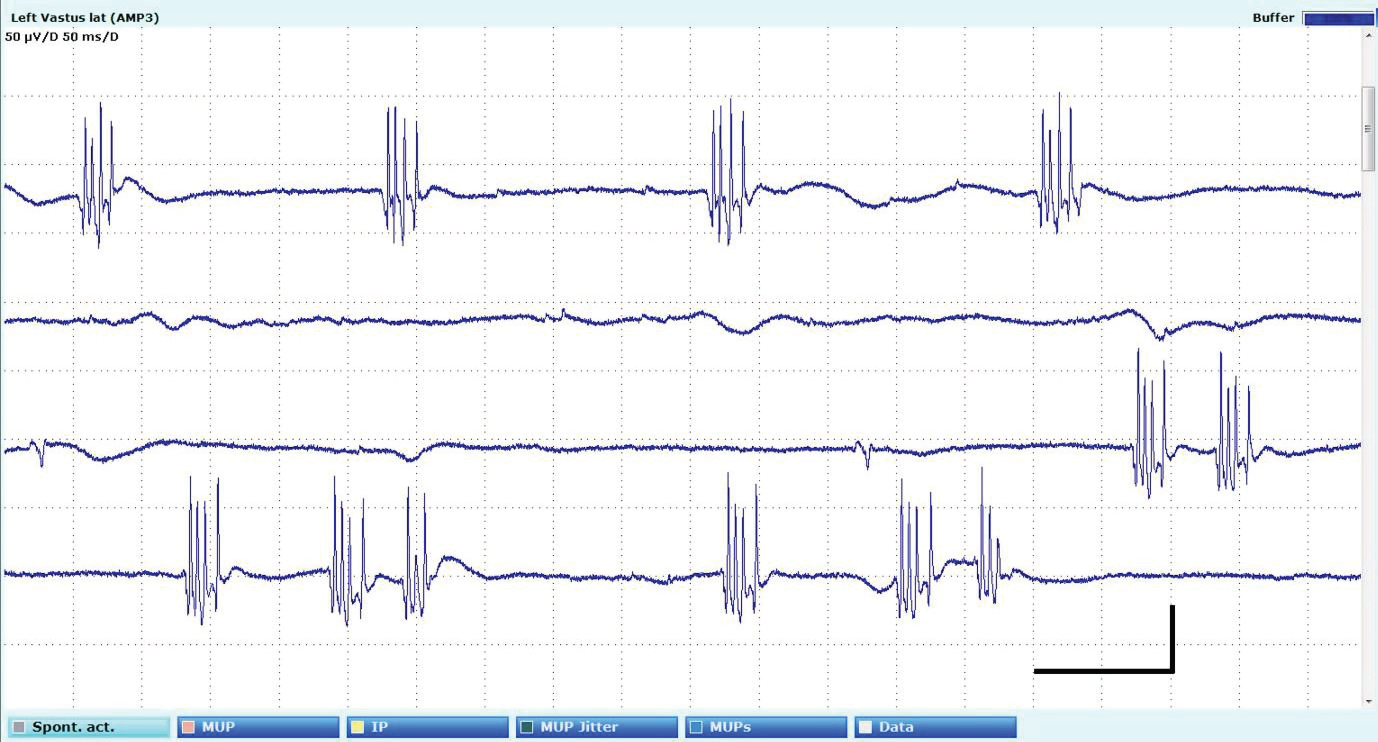
due to the after-discharges.[Figure 2] Electromyography revealed
myokymic discharges, sparse fasciculations and complex motor unit
potentials in limb and paraspinal muscles.[Figure 3] Mixed nerve and
cutaneous silent periods were normal in right abductor pollicis brevis.
Heart rate variability was reduced at rest and during deep breathing.
Hemogram, liver function tests, renal function tests, thyroid
function tests, antinuclear antibody (ANA) profile and serum creatine
kinase were normal. CASPR2 antibodies were strongly positive, and
LGI1 antibodies were weakly positive by cell-based assay. Mi antibody
was positive on myositis panel. The Mi antibody positivity might be
an incidental finding and its significance could not be ascertained.
Magnetic resonance imaging of brain and spine were normal.
The patient received pulse-dose intravenous methylprednisolone
(1g /day) for five days followed by intravenous immunoglobulin (2
g/kg over 5 days). There was a significant reduction in insomnia,
autonomic dysfunction, and behavioral symptoms during the
hospital stay. During follow up at two months patient had resolution
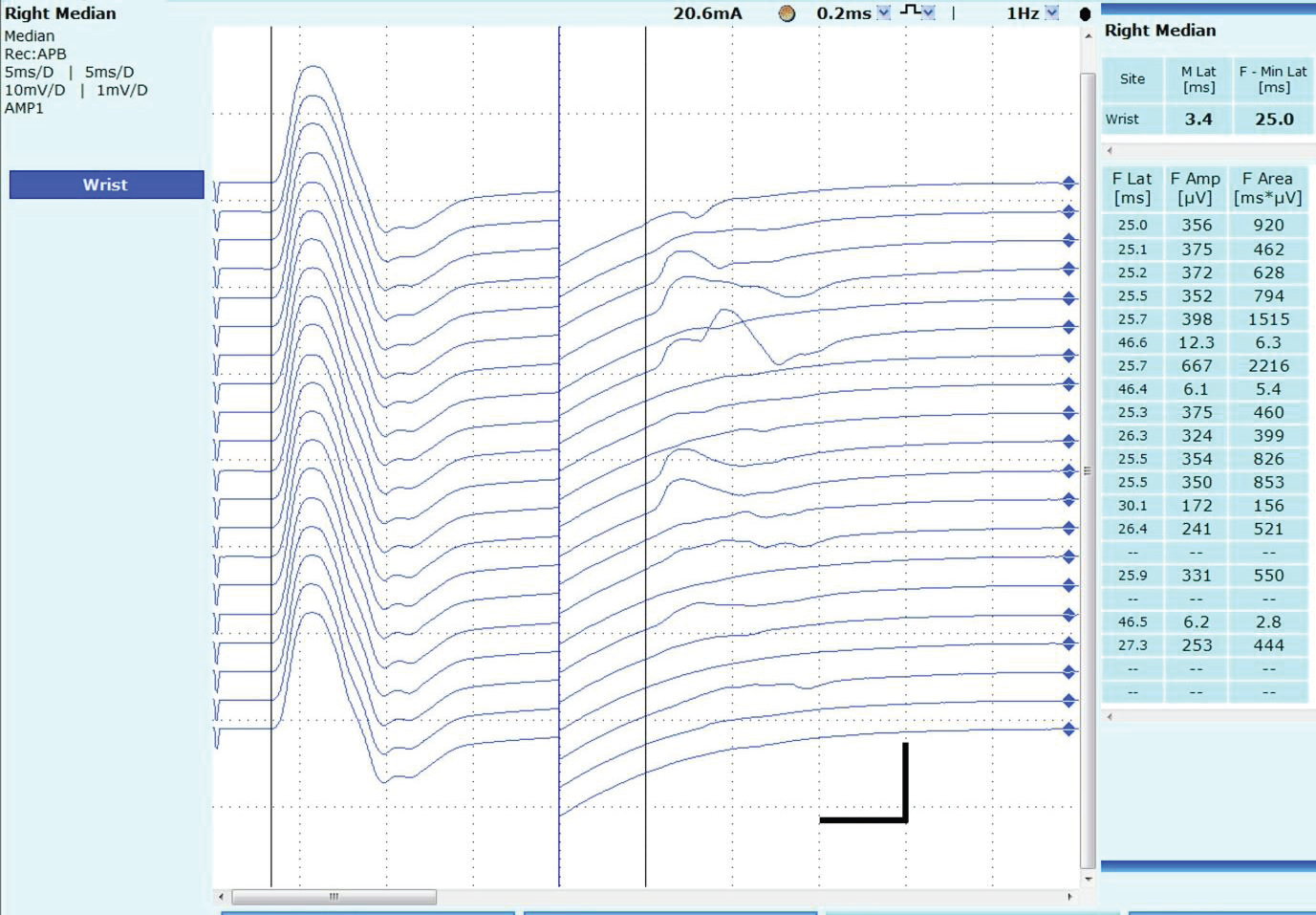
of pain, autonomic dysfunction, myokymia. Repeat motor nerve
conductions revealed disappearance of after-discharges with normal
F-wave responses. [Figure 4]. During follow-up, he was not initiated
on further immunomodulation therapy and repeat antibody testing
was not done. His last follow up was through telephonic consultation
after 3 years of onset of symptoms. He currently has no recurrence of
symptoms and is independent for all activities of daily living.
Discussion
This patient exhibited the classic presentation of Morvan
syndrome with peripheral and central nervous system involvement
and antibody positivity for both CASPR2 and LGI1. He had a probable
trigger in the form of anabolic steroid exposure preceding the onset
of Morvan syndrome. VGKC complex antibodies are detected in
up to 72% of Morvan syndrome patients. Immunopathologically,
anti-VGKC antibodies lead to downregulation of potassium ion
channel function, resulting in lack of inhibition manifesting with
neuronal hyperexcitability which is seen clinically as neuromyotonia,
dysautonomia and CNS symptoms. [6,7] Peripheral neuronal
hyperexcitability can be demonstrated with motor nerve conduction
study which reveal repetitive after-discharges following the compound
muscle action potential, often obscuring the F-wave. Needle EMG
reveals myokymia, complex motor unit potentials and neuromyotonia.
Early immunotherapy with corticosteroids and intravenous
immunoglobulin therapy is critical for obtaining good clinical result.
Anabolic steroids may disrupt immune tolerance by altering
lymphocyte differentiation, cytokine production, and antibody
generation, serving as potential triggers for autoimmune neurological
syndromes.[4]
Conclusion
Morvan syndrome is a rare neurological disorder with both
peripheral nerve and central nervous system involvement. This case
report highlights the importance of recognizing atypical autoimmune
triggers such as anabolic steroids and the importance of initiating
early immunotherapy to ensure good neurological outcomes.
Conflicts of Interest:
The authors declare no conflicts of interest.References
Citation
Sai Bharath BV, Saroja AO, Naik KR, Sumanth CV. Morvan Syndrome with CASPR2 and LGI1 Positivity Triggered by Anabolic Steroid Exposure: A Case Report. Indian J Neurol. 2025;6(1): 155.