Case Report
Spinal Cord Cavernoma Presenting as Acute Transverse Myelitis
Jasti Shivani*, Shobana N, Sacrates M, Selvakumar CJ and Sadeeshkumar V
Department of Neurology, Coimbatore Medical College and Hospital, Coimbatore, Tamil Nadu, India.
*Corresponding author:Shivani Jasti, Department of Neurology, Coimbatore Medical College and Hospital, Coimbatore, Tamil Nadu, India. E-mail Id: shivanijasti49@gmail.com
Article Information: Submission: 04/08/2025; Accepted: 02/09/2025; Published: 06/09/2025
Copyright: © 2025 Shivani J, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
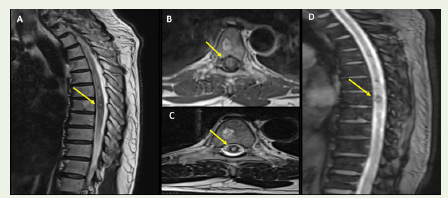
A 67-year-old male presented with history of acute onset bilateral
lower limb weakness, decreased sensation below umbilicus and
urinary retention which progressed within a span of 12 hours to
reach its nadir. Neurologic examination revealed paraplegia, absent
deep tendon reflexes in lower limbs, bilateral absent plantar responses
and impaired touch, pain, temperature, joint-position and vibration
sensation below T10 dermatome, indicative of spinal-cord pathology
around D7-D8 vertebral levels . MRI of the dorsolumbar spine showed
a cavernous malformation at D7 vertebral level with surrounding
haemorrhage and oedema extending about 13cms longitudinally
[Figure 1A-D].
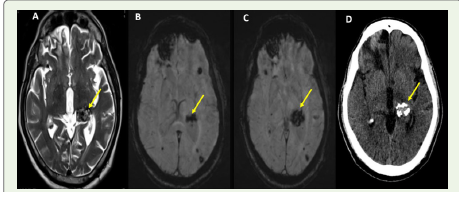
The screening MRI of the brain revealed multiple cavernous
malformations of bilateral cerebral hemispheres [Figure 2A-D].
Cavernous malformations of the spinal cord are rare entities,
comprising 5% of intramedullary spinal cord lesions [1]. Unlike
their intracranial counterparts, spinal cavernomas have an increased
tendency to bleed. The clinical presentation of spinal cord cavernomas
can be varied, ranging from limb paraesthesias when the lesion is
occult to debilitating spinal cord syndromes such as paraplegia,
progressive myelopathy to acute transverse myelitis [2] when there
is haemorrhage into the cavernoma. Our case highlights the acute
presentation of spinal cord cavernoma due to haemorrhage.
References
Citation
Jasti Shivani, Shobana N, Sacrates M, Selvakumar CJ and Sadeeshkumar V Spinal Cord Cavernoma Presenting as Acute Transverse Myelitis. Indian J Neurol. 2025;6(1): 154.