Case Report
A Rare Case of Right Eight-and-a-Half Syndrome with Left-Sided Ataxia Secondary to Subacute Brainstem Infarction in a Diabetic-Hypertensive Male
Akshay Bhutada, Sangita Deka and Papori Borah
Department of Neurology, GMCH Guwahati, Assam, India
*Corresponding author:Dr Akshay Bhutada, Department of Neurology, GMCH Guwahati, Assam, India Email Id: akshaythegiant@gmail.com
Article Information: Submission: 17/07/2025; Accepted: 12/08/2025; Published: 15/08/2025
Copyright: © 2025 Bhutada A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Eight-and-a-half syndrome is a rare neuro-ophthalmological condition caused by a focal brainstem lesion involving the paramedian pontine reticular formation (PPRF), medial longitudinal fasciculus (MLF), and ipsilateral facial nerve fascicle¹. We report a 60-year-old diabetic-hypertensive male with right eight-and-a-half syndrome and contralateral cerebellar ataxia due to a subacute infarct in the right hemipons extending to the pontomedullary junction. The case illustrates a classic example of clinico-radiological correlation and
emphasizes the role of early neuroimaging.
Introduction
Eight-and-a-half syndrome, first described by Eggenberger in
1998, combines one-and-a-half syndrome with an ipsilateral lower
motor neuron (LMN) facial palsy [1]. The one-and-a-half syndrome
results from damage to the PPRF or abducens nucleus along with
the MLF on the same side, leading to horizontal gaze palsy and
internuclear ophthalmoplegia [1-4] When the lesion also involves the
adjacent fascicle of the facial nerve, an LMN facial palsy completes
the clinical picture[1]. The most common causes are brainstem
infarcts, demyelinating lesions, and tumors [2-5]. Due to the compact
neuroanatomy of the pons, such clinical findings can assist with
precise localization even before imaging [5].
Case Presentation
A 60-year-old right-handed male with a 10-year history of type
2 diabetes mellitus and systemic hypertension presented on day four
of symptom onset with acute giddiness, facial deviation to the left,
and unsteadiness while walking. He had no headache, vomiting,
seizures, trauma, fever, or focal limb weakness. He had discontinued
antihypertensives and oral hypoglycemics. No history of smoking,
alcohol, or familial neurological disorders was noted.
On general examination, the patient had a blood pressure of
150/90 mmHg and a pulse rate of 82 beats per minute, which was
regular. His fasting blood sugar was 230 mg/dL and postprandial
blood sugar was 389 mg/dL. There was no pallor, icterus, cyanosis,
lymphadenopathy, or pedal edema.
Neurologically, he was alert and oriented to time, place, and
person. Cranial nerve examination revealed conjugate right
horizontal gaze palsy with preserved vertical gaze, right internuclear
ophthalmoplegia characterized by failure of adduction of the right eye
and abducting nystagmus in the left eye, and right LMN facial palsy,
evidenced by flattened nasolabial fold and inability to puff the right
cheek or close the right eye tightly. Other cranial nerves were intact.
Motor system examination showed normal tone and power (MRC
grade 5/5) in all limbs. Deep tendon reflexes were brisk bilaterally,
and plantar responses were flexor. Sensory examination revealed no
abnormalities.
Cerebellar signs were evident on the left side, with limb ataxia,
dysdiadochokinesia, and past-pointing. The patient also displayed
truncal ataxia and walked with a wide-based gait, tending to veer to
the left.
Systemic examination of the cardiovascular, respiratory, and abdominal systems was unremarkable.
Systemic examination of the cardiovascular, respiratory, and abdominal systems was unremarkable.
Neuroimaging:
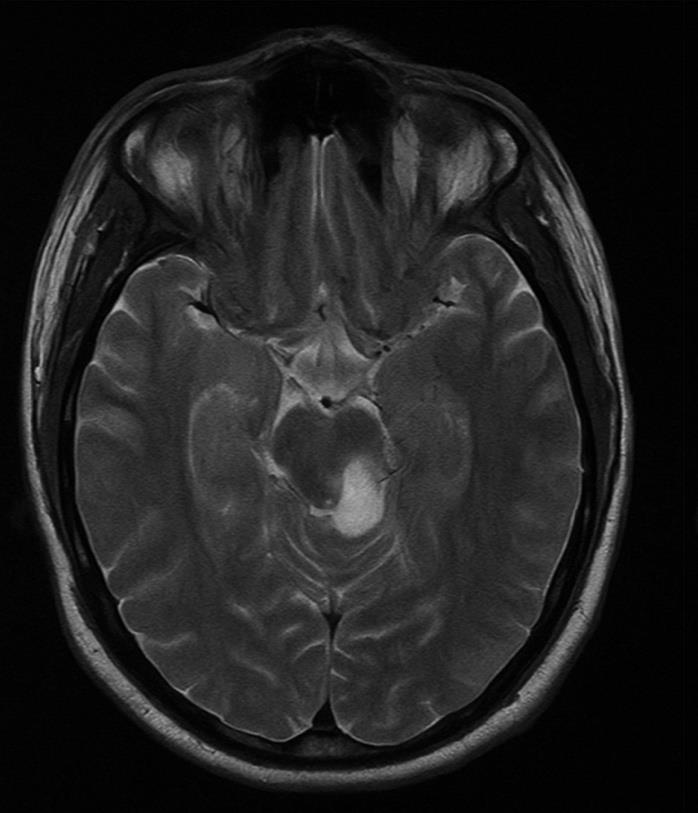
MRI of the brain and orbits (dated 11/06/2025) revealed a
subacute infarct involving both the dorsal and ventral aspects of the
right hemipons, extending inferiorly to the pontomedullary junction.
There was no susceptibility artifacts noted on SWI sequences, and no
abnormal enhancement was seen on post-contrast T1 images. Mild
cerebral atrophy was observed, with a global cortical atrophy (GCA)
score of 2.MR TOF angiography showed no significant vascular narrowing, aneurysms, or arteriovenous malformations in the intracranial circulation. The bilateral posterior communicating arteries were hypoplastic.
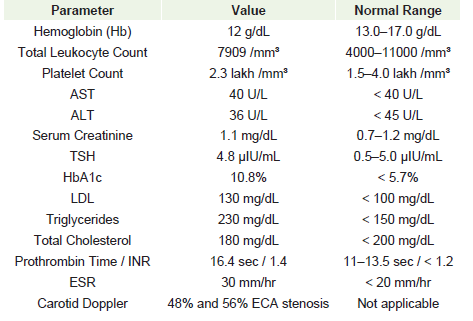
Carotid Doppler ultrasonography revealed 48% stenosis in the right and 56% in the left external carotid artery (ECA). The plaques were classified as Type II atherosclerotic, without ulceration or flow limiting internal carotid artery obstruction.
Final Diagnosis:
The patient was diagnosed with eight-and-a-half syndrome
secondary to a subacute infarct in the right hemipons. The left-sided
cerebellar ataxia was attributed to involvement of pontocerebellar
fibers. The infarct was likely due to underlying uncontrolled diabetes
mellitus, hypertension, and dyslipidemia.Treatment and Clinical Course:
The patient was admitted to the neurology ward and managed
conservatively. He was started on Aspirin 150 mg daily and
Atorvastatin 40 mg daily. Strict glycemic control was initiated with
insulin therapy. Antihypertensive therapy was optimized using
Amlodipine and Telmisartan. A structured physiotherapy program
was implemented, focusing on balance training, coordination, and
facial muscle rehabilitation.During the hospital stay, the patient remained hemodynamically stable and did not develop any new neurological deficits. He showed gradual improvement in gait and balance. He was discharged with instructions for continued physiotherapy, optimization of vascular risk factors, and regular follow-up.
Discussion
Eight-and-a-half syndrome is a rare brainstem disorder resulting
from a lesion affecting the horizontal gaze center, internuclear
connections, and ipsilateral facial nerve fascicle [1,4,5]. The lesion
usually localizes to the dorsal pontine tegmentum, as observed in
this case [5]. The presence of contralateral ataxia likely signifies
additional involvement of the right inferior cerebellar peduncle or
cerebellothalamic fibers at the pontomedullary level [5].
While Cho et al. reported eight-and-a-half syndrome due to
pontine infarction in a hypertensive patient without ataxia⁶, Salazar
et al. described brainstem infarcts with overlapping oculomotor and
cerebellar findings, but not a classic eight-and-a-half presentation [3].
Our case presents a comprehensive example of this rare syndrome with cerebellar involvement, implying a broader lesion. Elevated ESR and HbA1c along with extracranial stenosis indicate a small vessel vasculopathy, consistent with TOAST type 3 etiology [4,5]. The patient was managed per standard ischemic stroke protocols using antiplatelets, statins, glycemic control, and physiotherapy. Although the thrombolytic window had lapsed, early neurorehabilitation improved function and prevented complications.
Our case presents a comprehensive example of this rare syndrome with cerebellar involvement, implying a broader lesion. Elevated ESR and HbA1c along with extracranial stenosis indicate a small vessel vasculopathy, consistent with TOAST type 3 etiology [4,5]. The patient was managed per standard ischemic stroke protocols using antiplatelets, statins, glycemic control, and physiotherapy. Although the thrombolytic window had lapsed, early neurorehabilitation improved function and prevented complications.
Conclusion
This case emphasizes the value of clinical localization in diagnosing
complex brainstem syndromes. The co-occurrence of eight-anda-
half syndrome with contralateral cerebellar ataxia pointed to an
extensive lesion in the right pontine and pontocerebellar regions.
Prompt MRI aided in confirming the clinical suspicion. Effective
control of modifiable vascular risk factors and timely rehabilitation
significantly contributed to the patient’s recovery. A high index of
suspicion in similar presentations can lead to accurate localization
and better outcomes.
Declarations:
Informed consent was obtained from the patient. There is no
conflict of interest to declare. No funding was received for this study.
Ethics approval was not required for a single case report.References
Citation
Bhutada A, Deka S, Borah P. A Rare Case of Right Eight-and-a-Half Syndrome with Left-Sided Ataxia Secondary to Subacute Brainstem Infarction in a Diabetic-Hypertensive Male. Indian J Neurol. 2025;6(1): 152.