Case Report
Cerebral Ptosis- A Masquerade to Glasgow Coma Scale
Nehali B Maiya, Ganesh KM, Pooja PS, Chandan GS and Padmakumar AV
Fortis Hospitals, Bannerghatta Road, Bengaluru, Karnataka. India
*Corresponding author:Dr Nehali B Maiya, Fortis Hospitals, Bannerghatta Road, Bengaluru, Karnataka. India. E-mail Id: nehalimaiya13@gmail.com
Article Information:Submission: 14/07/2025; Accepted: 05/08/2025; Published: 07/08/2025
Copyright: © 2025 Maiya NB, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
List of abbreviations:
GCS- Glasgow Coma Scale; CT- Computed Tomography; NIHSSNational
Institute of Health Stroke Scale; MRI- Magnetic Resonance
Imaging; MCA- middle cerebral artery; ICU- Intensive Care UnitIntroduction
The Glasgow Coma Scale (GCS) was first described by Graham
Teasdale and Bryan Jennett in 1974. It is still widely used as a clinical
scale to assess a patient’s depth of impaired consciousness and coma
following an acute brain injury [1]. The GCS has scores between 3 and
15, 3 being the worst and 15 the best. It measures three parameters:
eye response (E), verbal response (V), and motor response (M).
Ptosis can be unilateral or bilateral, partial or complete, occurs in
cases of cerebral ischemic or hemorrhagic stroke, without involvement
of brainstem or without involvement of ocular mechanism can be
termed as cerebral ptosis [2]. It is associated with higher frequency of
gaze preference to side of lesion as well as upgaze limitation compared
to patients without cerebral ptosis [2]. Fewer studies are conducted to
ascertain the GCS score in patients with cerebral ptosis. We describe a
case where cerebral ptosis caused a documentation of spuriously low
GCS and highlight the importance of detailed ptosis examination in
acute cerebrovascular accidents patients.
Case description
A 69-year-old male presented to the emergency room in the
window period of acute ischemic stroke with complaints of left sided
weakness with slurred speech. GCS on arrival was 15/15 with National
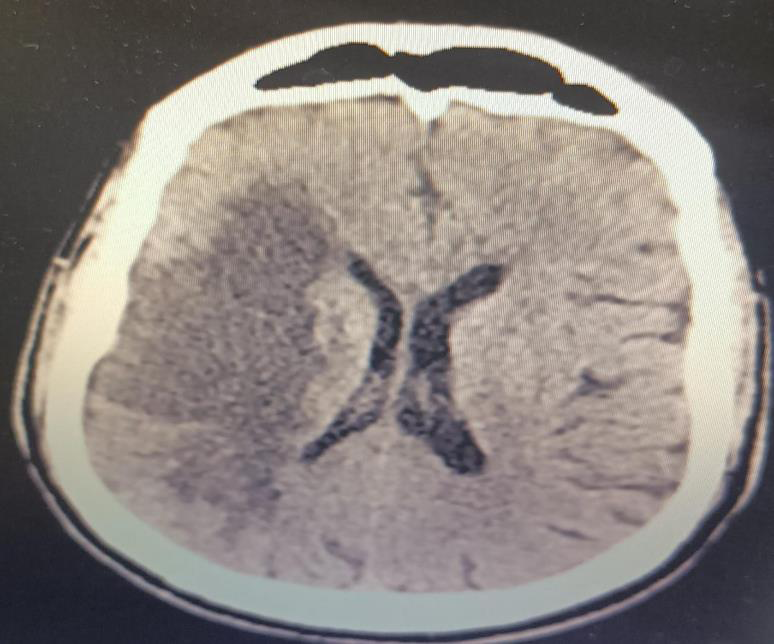
Institute of Health Stroke Scale (NIHSS) of 8. Magnetic Resonance
Imaging (MRI) showed acute ischemia involving the right MCA
(middle cerebral artery) with M1 cutoff and no distal flow [Figure 1]
Patient underwent mechanical thrombectomy and was admitted
to Intensive Care Unit (ICU) for neuromonitoring. An Improvement
in motor power was noted on the left side with power of -3/5 with
GCS of E4V5M6. 48 hrs. post thrombectomy GCS of the patient was
noted to be E1V5M6 despite promptly following verbal commands.
With low GCS, emergent computer tomography (CT) of brain was
performed which showed subtle hyperintensities in the right posterior
peninsular white matter suggestive of minimal hemorrhages within
the infarct with mild mass effect on the right lateral ventricle with no
midline shift. [Figure 2]


Conservative strategies such as anti-edema measures along with
supportive care were continued. The patient continued to have GCS
of E1V5M6. Repeat CT brain done on day 5 showed similar findings
of the previous. Diagnosis of cerebral ptosis was done according to
Manconi’s criteria.
GCS as a prognostic indicator of neurological deterioration was
not considered in this case. Conservative management was continued
and by day 15, improvement in ptosis was noted.
Discussion
The Glasgow Coma Scale (GCS) has been used as a standard tool
to describe the extent of impaired consciousness. The scale assesses
patients based on three aspects: eye-opening, motor, and verbal
responses [3]. Assessing each of these separately provides a clear
picture of a patient’s neurological state.
Assessment of responsiveness with the Glasgow Coma Scale is
widely used to guide early management of patients with any kind
of acute brain injury [3]. Decisions to be taken in more severely
impaired patients include emergent management such as securing
the airway and triaging to determine the need of immediate patient
transfer to initiate the appropriate neurological intervention.
Decisions in less severely impaired patients include the need for
neuroimaging, admission for observation or discharge [3]. Serial
Glasgow Coma Scale assessments are done in monitoring the
clinical course of a patient and to decide on their management. In a
comparative study by Gennarelli et al, it was demonstrated that the
existence of a continuous, progressive association between increasing
mortality after a head injury and decreases in GCS Score from 15 to
3 [4]. Even though, GCS is one of the most powerful clinical tools
to prognosticate, neither the GCS score nor any single tool alone
should be used to predict a patient’s outcome. This is because the
prognostic implications of the score are influenced by factors such
as diagnosis,need of mechanical ventilation, age of the patient and
clinical indices such as pupillary dysfunction and conditions such as
cerebral ptosis.
Ptosis or blepharoptosis is defined as an abnormally
low‑positioned eyelid [2]. Ptosis can be congenital or acquired with
neurogenic, myogenic, mechanical and traumatic causes [2]. Cerebral
ptosis which is a rarer cause of acquired ptosis, can be partial or
complete, unilateral or bilateral without brainstem involvement [5].
Diagnosis of cerebral ptosis is made by inclusion criteria of Manconi as
described in Table 1 above.There have been many theories regarding
the mechanism of insult leading to cerebral ptosis.The study done
by Manconi et al postulated that supranuclear disruption of ocular
and motor nerve pathways is the reason for oculomotor dysfunction
and cerebral ptosis [6]. In unilateral hemispheric involvement, eyelid
dysfunction can be seen with insult of frontal and parietal lobes as
cerebral ptosis. These eyelid abnormalities are more commonly
described with right hemispheric involvement as described by Vegda
et al [2]. Another study done by Johnston et al, reported resolution of
cerebral ptosis secondary to resolution of parietal dysfunction which
was seen in the right hemispheric infarct [7]. The right cerebral cortex
is postulated to be responsible for the tonicity of levator palpebrae
superioris activity [2]. In a study done by Averbuch-Heller et al it was
reported that bilateral ptosis was the first sign of imminent herniation.
However, the role of bilateral cerebral ptosis to be used as a clinical
tool to predict impending deterioration needs further research and
more reporting.
In our patient with right hemispheric involvement but with no signs of herniation, we asked a few questions to derive the information about his neurological status such as he was asked to tell his name, address, day/date and other personal details. He was also asked to follow simple commands such as protruding his tongue, holding the examiner’s fingers and lifting his left arm and leg (nonparetic side).
In our patient with right hemispheric involvement but with no signs of herniation, we asked a few questions to derive the information about his neurological status such as he was asked to tell his name, address, day/date and other personal details. He was also asked to follow simple commands such as protruding his tongue, holding the examiner’s fingers and lifting his left arm and leg (nonparetic side).
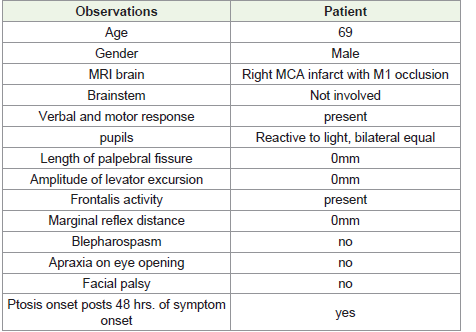
Other parameters such as vertical length of palpebral fissure,
amplitude of levator excursion, blepharospasm, apraxia of eyelid
opening, gaze preference, horizontal or vertical gaze palsy, pupillary
size, symmetry and pupillary light reaction, and presence of facial
palsy were examined and noted as done in the study by Vegda et al
[2].
Thus, we concluded that our patient had cerebral ptosis according
to the Manconi criteria.
Repeat CT brain did not show any increase in midline shift or cerebral edema. Conservative management was continued and patients’ clinical status improved on day 15.
In our patient there was no correlation noted between cerebral ptosis and worsening neurological status and hence cerebral ptosis should not be confused with reduced consciousness of the patient.
Repeat CT brain did not show any increase in midline shift or cerebral edema. Conservative management was continued and patients’ clinical status improved on day 15.
In our patient there was no correlation noted between cerebral ptosis and worsening neurological status and hence cerebral ptosis should not be confused with reduced consciousness of the patient.
Conclusion
Cerebral ptosis which can occur unilateral or bilaterally, is a rarely
described sign, physiological basis of which still remains unknown.
Paying attention to this often‑ignored neurological finding secondary
to fewer cases reported, may probably be useful in prognosticating
the outcome. Assessment of the patient and accurately identifying the
confounding factors in various neurological scores such as Glasgow
Coma Score is very vital and needs more research.
Clinical significance:
Clinical significance of this case report includes many learning
points such as, firstly, whenever there is a drop in GCS score of a
patient with hemispheric stroke, the possibility of cerebral ptosis
needs to be considered. Second, using alternative neurological
assessment tools in clinical suspicion of cerebral ptosis needs to
be explored. Finally, appropriate education of the bedside nurse
regarding the cerebral ptosis phenomenon is essential and the need
to assess other responses in GCS, like in our patient, is important to
identify worsening neurological status.Acknowledgement
We thank Dr Guruprasad, Consultant Neurology at Fortis
Hospital Bannerghatta road, for his valuable inputs.
References
Citation
Maiya NB, Ganesh KM, Pooja PS, Chandan GS, Padmakumar AV. Cerebral Ptosis- A Masquerade to Glasgow Coma Scale. Indian J Neurol. 2025;6(1): 149.