Case Report
Revealing Primary CNS Vasculitis in the Shadow of Tuberculosis
Mukherjee A*, Kumari P, Rautiya V, Vyshnavi G, Sangharsh, Mahima M, Wasnik P, Pranita and Shukriya S
Department of Medicine, All India Institute of Medical Sciences (AIIMS), Raipur, Chhattisgarh, India
*Corresponding author:Avinash Mukherjee, Department of Medicine, All India Institute of Medical Sciences (AIIMS), Raipur, Chhattisgarh, India, Email Id: avinashmukherjee91@gmail.com
Article Information:Submission: 10/07/2025; Accepted: 29/07/2025; Published: 31/07/2025
Copyright: © 2025 Mukherjee A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction:Primary angiitis of the central nervous system (PACNS) is a rare and often under- recognized form of vasculitis confined to the CNS. It typically presents with non- specific neurological symptoms, making it difficult to distinguish from infections, malignancies, and demyelinating disorders, especially in regions endemic for tuberculosis.
Aim:To highlight the diagnostic challenges of PACNS in young individuals and emphasize the importance of a thorough differential workup in cases presenting with recurrent or treatment-resistant neurological symptoms.
Case:A 24-year-old previously healthy male presented with chronic holocranial headache and episodic neurological symptoms including slurred speech and altered sensorium. He was initially diagnosed and treated as a case of tubercular meningitis. However, recurrence of symptoms despite appropriate therapy prompted re-evaluation. MRI findings showed multiple micro-bleeds and perivascular enhancement with MR angiography showing “skipped” or “segmental” pattern of vessel involvement seen — a classical radiological hallmark of PACNS. CSF analysis and serologic workup ruled out infectious and systemic autoimmune etiologies. Based on imaging and exclusion of other causes, a diagnosis of PACNS was made.
Results:The patient was treated with intravenous methylprednisolone followed by oral steroids, low-dose aspirin, and rituximab. He showed significant clinical improvement with no recurrence on follow-up. The case underscores the value of revisiting diagnoses when initial treatment fails, especially in atypical presentations.
Aim:To highlight the diagnostic challenges of PACNS in young individuals and emphasize the importance of a thorough differential workup in cases presenting with recurrent or treatment-resistant neurological symptoms.
Case:A 24-year-old previously healthy male presented with chronic holocranial headache and episodic neurological symptoms including slurred speech and altered sensorium. He was initially diagnosed and treated as a case of tubercular meningitis. However, recurrence of symptoms despite appropriate therapy prompted re-evaluation. MRI findings showed multiple micro-bleeds and perivascular enhancement with MR angiography showing “skipped” or “segmental” pattern of vessel involvement seen — a classical radiological hallmark of PACNS. CSF analysis and serologic workup ruled out infectious and systemic autoimmune etiologies. Based on imaging and exclusion of other causes, a diagnosis of PACNS was made.
Results:The patient was treated with intravenous methylprednisolone followed by oral steroids, low-dose aspirin, and rituximab. He showed significant clinical improvement with no recurrence on follow-up. The case underscores the value of revisiting diagnoses when initial treatment fails, especially in atypical presentations.
Keywords:PACNS, Young Adult; Refractory Headache; Microbleeds; Rituximab; Tubercular meningitis mimics
Introduction
Primary angiitis of the central nervous system (PACNS) is an
uncommon and often elusive form of vasculitis, limited to the brain
and spinal cord without systemic involvement. First described in the
1950s, PACNS remains a diagnostic challenge due to its rarity, variable
clinical presentation, and absence of pathognomonic laboratory
findings. The condition can mimic a wide range of neurological
disorders, including infections (such as tubercular meningitis),
demyelinating diseases, malignancies, and RCVS. PACNS typically
presents with sub-acute headache, cognitive disturbances, focal
neurological deficits, or seizures. Due to its segmental involvement
and lack of systemic markers, the diagnosis is primarily one of
exclusion and often delayed.
In India, tuberculosis remains a common CNS pathology, further
complicating the diagnosis of PACNS. We present a case of a young
male initially treated as tubercular meningitis, who was later diagnosed
with PACNS after relapse of symptoms and detailed re-evaluation.
This case highlights the importance of considering PACNS in the
differential diagnosis of chronic or relapsing neurological symptoms,
particularly in TB-endemic regions.
Case Presentation
A 24-year-old male shopkeeper with no prior comorbidities
or addictions presented in July 2023 with persistent holocranial
headache of throbbing nature. The headache, initially mild, gradually
intensified over weeks. It was associated with blurring of vision
but not accompanied by photophobia, phonophobia, vomiting, or
diplopia.
He was evaluated at a local clinic, and based on cranial MRI and
cerebrospinal fluid (CSF) findings, a clinical diagnosis of tubercular
meningitis was made. He was initiated on anti- tubercular therapy
(ATT) per DOTS guidelines along with oral dexamethasone. The
patient showed initial improvement, with partial resolution of
headache symptoms. Repeat MRI with SWI sequencing was done
which demonstrated multiple blooming foci in pons, cerebellar
vermis and inferior cerebellar cortex. He was subsequently labelled as
TB-Reactivation and ATT was continued.
However, in January 2025, he began experiencing episodes of
slurred speech, transient altered sensorium, and decreased verbal
output with excessive drowsiness. These episodes were spontaneous
and self-limiting. Levetiracetam 500 mg twice daily was started
empirically.
Despite initial improvement, symptoms recurred on tapering
steroids. This prompted further neurological evaluation.
The patient presented to our institution with the above complaints
and admitted for further workup.
Examination
On admission, the patient was alert, conscious, and oriented to
time, place, and person. Vitals were stable (BP 120/60 mmHg, HR
70 bpm, RR 22/min, SpO₂ 98%). There were no signs of systemic
involvement—no pallor, icterus, cyanosis, or edema.
• Neurological examination revealed:
Higher mental functions: Intact Cranial nerves: Normal Motor system: Normal tone and full power (5/5) in all limbs
Deep tendon reflexes: 2+
Plantar responses: Bilateral flexor
Sensory examination: Within normal limits
• Investigations
Complete Blood Count: Within normal limits
ESR: Elevated at 70 mm/hr
Liver and Renal Function Tests: Normal C3 and C4 Levels - within normal limits
• CSF Analysis (repeat):
• Neurological examination revealed:
Higher mental functions: Intact Cranial nerves: Normal Motor system: Normal tone and full power (5/5) in all limbs
Deep tendon reflexes: 2+
Plantar responses: Bilateral flexor
Sensory examination: Within normal limits
• Investigations
Complete Blood Count: Within normal limits
ESR: Elevated at 70 mm/hr
Liver and Renal Function Tests: Normal C3 and C4 Levels - within normal limits
• CSF Analysis (repeat):

Cells: 38 (lymphocytic predominance) Protein: 106 mg/dL
Glucose: 54 mg/dL (RBS: 102 mg/dL) CBNAAT: Not detected
AFB stain: Negative Cryptococcal antigen: Negative
CSF for Malignant cells: Negative
• Autoimmune Panel:
ANA: Negative
p-ANCA and c-ANCA: Negative Anti-AQP4 / Anti MOG:
Negative
Rheumatoid Factor and Anti-CCP: Negative
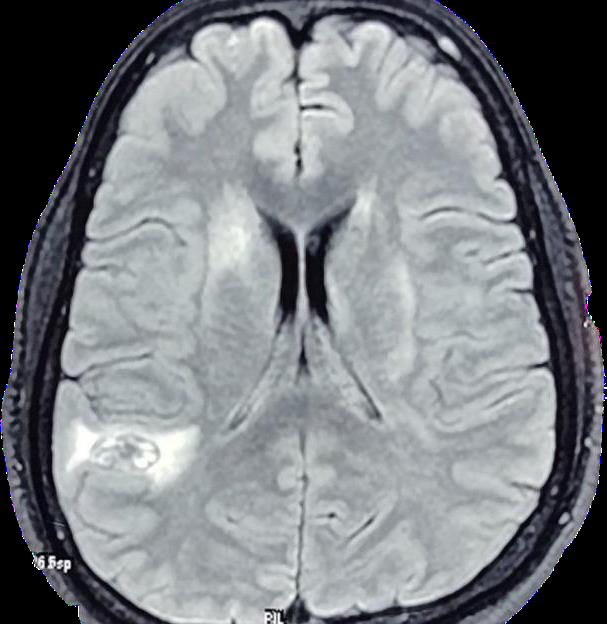
MRI Brain (sequential) with MR Angio and Whole Spine Screening::
Intra cerebral hematoma in right parieto occipital lobe with
peri-lesional edema
Multiple micro-bleeds and punctate microhemorrhages
dispersed in bilateral brain parenchyma
Confluent T2/FLAIR hyperintensities in bilateral deep
cerebral white matter.
Post-contrast imaging: Perivascular enhancement along
vessels in bilateral cerebral hemispheres
MR angiography: “Skipped” or “segmental” pattern of
vessel involvement seen — a classical radiological hallmark
of PACNS. This refers to alternating areas of stenosis and
normal-caliber segments across multiple intracranial vessels,
reflecting multi focal vasculitic inflammation.
MRI Spine Screening - With in normal limits with no
demyelinating lesionsAfter comprehensive evaluation, infectious etiologies such as TB
Meningitis, Neuro-syphilis and HIV related Vasculopathy were ruled
out with negative CSF CBNAAT, negative AFB staining, absence
of basal meningeal enhancement, negative VDRL serologies and
negative HIV serologies respectively.
Auto-immune mimics such as SLE, ANCA vasculitis, Rheumatoid
vasculitis and Bechet’s were ruled out as ANA, ANCA, RA, anti CCP
and C3, C4 levels were not suggestive along with absence of any
systemic sign/symptoms such as absence of any rash, hematuria,
hemoptysis, oral or genital ulcers.
Other Demyelinating diseases such as MS, NMO and MOG were
ruled out with the absence of any demyelinating lesions on MRI and
absence of Anti Aquaporin and MOG antibodies.
Based on imaging and exclusion of other differentials—including
CNS infections, Autoimmune /Systemic vasculitis, and Demyelinating
disorders—a diagnosis of Primary Angiitis of the Central Nervous
System (PACNS) was established.
Treatment and Follow-up
The patient was started on:
* Intravenous methylprednisolone pulse therapy (1 g/day for 3
days)
* Maintenance oral corticosteroids (Prednisolone)
* Aspirin 75 mg once daily
* Rituximab-based immunosuppressive therapy
The patient showed marked clinical improvement following
immunosuppressive therapy. At follow-up visits, there were no
further episodes of headache or altered sensorium. Neurological
examination remained normal, and he resumed daily activities
without limitations. Continued follow-up is planned to monitor for
disease recurrence or complications related to immunosuppressive
therapy.
Discussion
Primary angiitis of the central nervous system (PACNS) is an
elusive and often misdiagnosed condition, primarily due to its nonspecific
presentation and its overlap with more prevalent neurological
disorders, especially in tuberculosis (TB)-endemic regions. Our case
underscores the diagnostic complexity of PACNS and the critical
importance of maintaining a high index of suspicion when patients
fail to respond to standard therapies.
The initial misdiagnosis of tuberculous meningitis in our patient
reflects a common clinical pitfall in regions like India, where TB
remains a major public health concern. In this case, prolonged antitubercular
therapy (ATT) failed to produce sustained improvement,
and symptom relapse upon steroid tapering prompted reconsideration
of the diagnosis.
The turning point in diagnosis was the detailed review of
sequential MRI findings, which revealed microhemorrhages in the
cerebellum and brainstem, along with perivascular enhancement and
MR angiography revealing skipped and segmental pattern of vessel
involvement — features more characteristic of PACNS than TB. The
cerebrospinal fluid (CSF) analysis, while showing elevated protein
and lymphocytic pleocytosis, lacked evidence of TB, malignancy, or
systemic autoimmune disease. Negative CSF CBNAAT and ADA
levels further strengthened the case against a tuberculous etiology.
Histopathological confirmation through brain biopsy remains
the gold standard for PACNS diagnosis but is often impractical due
to the invasiveness and location of lesions. In such cases, a diagnosis
of exclusion based on clinical judgment, imaging, and laboratory data
becomes essential. This aligns with current diagnostic frameworks
that prioritize non-invasive tools when biopsy is not feasible.
Therapeutically, the patient’s significant improvement with immunosuppressive treatment — including intravenous methylprednisolone and rituximab — reaffirms the autoimmune nature of PACNS and the need for timely initiation of appropriate therapy.
Therapeutically, the patient’s significant improvement with immunosuppressive treatment — including intravenous methylprednisolone and rituximab — reaffirms the autoimmune nature of PACNS and the need for timely initiation of appropriate therapy.
Conclusion
This case exemplifies the diagnostic challenge posed by Primary
CNS Vasculitis (PACNS), particularly in TB-endemic regions where
infectious etiologies are often the first consideration. The patient’s
prolonged misdiagnosis as tuberculous meningitis, despite atypical
features and poor therapeutic response, underscores the need for
heightened clinical vigilance.
Early recognition of PACNS requires a combination of detailed neuroimaging, exclusion of mimics, and a multidisciplinary approach. This case also highlights the value of immunosuppressive therapy — especially the role of rituximab — in achieving favorable outcomes. Clinicians must consider PACNS in the differential diagnosis of young adults with chronic relapsing neurological symptoms unresponsive to conventional treatments.
Timely diagnosis and initiation of appropriate therapy are critical to preventing irreversible neurological damage and improving patient prognosis in this rare but treatable condition.
Early recognition of PACNS requires a combination of detailed neuroimaging, exclusion of mimics, and a multidisciplinary approach. This case also highlights the value of immunosuppressive therapy — especially the role of rituximab — in achieving favorable outcomes. Clinicians must consider PACNS in the differential diagnosis of young adults with chronic relapsing neurological symptoms unresponsive to conventional treatments.
Timely diagnosis and initiation of appropriate therapy are critical to preventing irreversible neurological damage and improving patient prognosis in this rare but treatable condition.
Authors’ Contribution:
All authors contributed equally to patient care, data collection,
literature review, and manuscript preparation. Dr. Pranita, Dr.
Wasnik P and Dr. Shukriya S led the case diagnosis and treatment
strategy along with supervised clinicaal decisions. All authors
reviewed and approved the final manuscript.Ethical Compliance: All procedures performed in this case were in accordance with the ethical standards of institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Conflict of Interest declaration: The authors declare that they have no conflict affiliations with or any organization or entity with any financial interest in the subject matter or materials discussed in this manuscript. The authors have no conflicts of interest to declare. Consent: Written and Informed consent of the patient and all authors were taken for publication of this case.
References
Citation
Mukherjee A, Kumari P, Rautiya V, Vyshnavi G, Sangharsh, et al. Revealing Primary CNS Vasculitis in the Shadow of Tuberculosis. Indian J Neurol. 2025;6(1): 148.