Research Article
Perspectives on Epilepsy Management among Indian Clinicians: A Cross-Sectional Study
Manjula S* and Krishna Kumar M
Department of Medical Services, Micro Labs Limited, Bangalore, Karnataka, India
*Corresponding author:Manjula S, Department of Medical Services, Micro Labs Limited, 31 Race Course Road, Bangalore, Karnataka, India. Email Id:drmanjulas@gmail.com
Article Information:Submission: 02/01/2024; Accepted: 27/01/2024; Published: 30/01/2024
Copyright: © 2024 Manjula S, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: While a majority of patients with epilepsy are able to maintain seizure control with one to two antiepileptic drugs (AEDs), many individuals require adjunctive therapy to achieve long-term remission. Hence, the implications of seizure differ according to the clinicians’ awareness about the patient’s
condition, knowledge about drugs and perspective about epilepsy treatment modalities. The current study aims in assessing the perspective of clinicians in management of epilepsy in India.
Methodology:A questionnaire-based cross sectional study was carried out among doctors in the major Indian cities. The study questionnaire included questions on prevalence, diagnosis, co- morbidities, lifestyle, patient’s awareness, compliance, and pharmacotherapy. A total of 93 doctors from major cities of all Indian states representing the geographical distribution shared their willingness to participate and provide necessary data.
Results:About 84 questionnaire booklets were distributed and 82 clinicians completed questionnaires and were collected personally by the study coordinators through the duration of 4 weeks. The responses reflected on the prevalence pattern of epilepsy in rural and urban India, the pattern of occurrences of generalized and partial seizures. The prescription pattern with levetiracetam and brivaracetam were unveiled as well.
Conclusion: Brivaracetam has emerged as a preferred choice, especially for newly diagnosed patients and those who do not respond adequately to levetiracetam. Its perceived advantages, including minimal adverse effects and improved efficacy, make it a valuable addition to the arsenal of antiepileptic drugs.
Methodology:A questionnaire-based cross sectional study was carried out among doctors in the major Indian cities. The study questionnaire included questions on prevalence, diagnosis, co- morbidities, lifestyle, patient’s awareness, compliance, and pharmacotherapy. A total of 93 doctors from major cities of all Indian states representing the geographical distribution shared their willingness to participate and provide necessary data.
Results:About 84 questionnaire booklets were distributed and 82 clinicians completed questionnaires and were collected personally by the study coordinators through the duration of 4 weeks. The responses reflected on the prevalence pattern of epilepsy in rural and urban India, the pattern of occurrences of generalized and partial seizures. The prescription pattern with levetiracetam and brivaracetam were unveiled as well.
Conclusion: Brivaracetam has emerged as a preferred choice, especially for newly diagnosed patients and those who do not respond adequately to levetiracetam. Its perceived advantages, including minimal adverse effects and improved efficacy, make it a valuable addition to the arsenal of antiepileptic drugs.
Keywords:Epilepsy; Seizure; Pharmacotherapy; Brivaracetam; Levetiracetam
Introduction
Epilepsy is one of the most common and disabling neurologic
conditions, yet we have an incomplete understanding of the detailed
pathophysiology and, thus, treatment rationale for much of epilepsy.
“Epilepsy” is the condition of recurrent, unprovoked seizures, where
a “seizure” is a paroxysmal alteration of neurologic function caused
by the excessive, hypersynchronous discharge of neurons in the brain
[1]. The majority of those with newly recognized epilepsy have many
seizures before diagnosis. Often, repetitive symptoms are necessary
to establish a diagnosis; moreover, close temporal proximity of
sequential seizures may be the reason patients seek medical care[1].
Most of the epilepsy patients reside in developing countries. About
10 million persons with epilepsy are there in India. Many people
with active epilepsy do not receive appropriate treatment for their
condition, leading to large treatment gap [3]. The pharmacological
armamentarium against epilepsy has expanded considerably over
the last three decades, and currently includes over 30 different
anti-seizure medications. The administration of antiepileptic drugs
(AEDs) was the first treatment of epilepsy. These are divided into
first-, second-, and third-generation AEDs. The commonly used
first-generation AEDs are phenytoin (PHT), phenobarbital (PB),
carbamazepine (CBZ), valproic acid (VPA), zonisamide (ZNS), and
clobazam (CLB). The third-generation drug includes lacosamide
(LCM) and eslicarbazepine acetate; others recently delivered are
included in the second generation. Post-second-generation AEDs
were commonly known as new AEDs. Gabapentin (GBP), topiramate
(TPM), lamotrigine (LTG), levetiracetam (LEV), and rufinamide
(RFN) are distributed as oral drugs [4].
Diagnosing epilepsy after a single unprovoked seizure when there
was high risk for recurrence may or may not lead to a decision to initiate
treatment. The proposed practical definition may provide support to
a physician who wants to treat a patient with high recurrence risk
after a single unprovoked seizure. However, a treatment decision was
distinct from a diagnosis, and should be individualized depending
upon the desires of the patient, the individual risk-benefit ratio
and the available options. The physician should weigh the possible
avoidance of a second seizure with associated risks against the risk
for drug-related side effects and costs for the patients. To be clear,
the diagnosis of epilepsy and a decision to treat were two related but
different issues. Many neurologists treat for a time after an acute
symptomatic seizure (for example, with Herpes encephalitis), with
no implication of epilepsy. In contrast, patients with mild seizures,
with seizures at very long intervals, or those declining therapy might
go untreated even when a diagnosis of epilepsy is beyond dispute.
Clinicians will have to individualize a determination of whether
epilepsy is resolved.While a majority of patients with epilepsy are
able to maintain seizure control with one to two antiepileptic drugs
(AEDs), many individuals require adjunctive therapy to achieve longterm
remission. Hence the implications of seizure differ according
to the clinicians’ awareness about the patient’s condition, knowledge
about drugs and perspective about epilepsy treatment modalities
[5,6]. Despite the availability of new anti-epileptic drugs during the
past three decades, repeated outcome analyses showed that > 30% fail
to achieve prolonged seizure freedom with medical treatment.
New treatment methods were needed to improve seizure
control while not affecting the patient’s quality of life by adverse
effects.Brivaracetam (BRV), an analog of levetiracetam (LEV), was
discovered during a target-based rational drug discovery program.
Although preclinical and post-marketing studies suggested broad
spectrum of efficacy, BRV is currently only approved as monotherapy
and adjunctive therapy of focal-onset seizures in patients age 4
years and older. Studies suggested that behavioral adverse events
were likely to be less frequent and less severe with BRV than LEV.
Therefore, switching to BRV may be considered for patients who have
seizure control with levetiracetam (LEV), but who cannot tolerate
its behavioral adverse effects [7]. BRV treatment could improve
psychobehavioral adverse events such as aggression and depressive
symptoms associated with previous LEV treatment.However, because
of a small number of patients and descriptive nature of the results,
the quality of evidence was low [8]. Understanding the prevalence,
treatment options, and prescription behavior in the context of
epilepsy is crucial for improved patient management and enhanced
quality of life. This study explores the current landscape of epilepsy
in India, focusing on pharmacotherapy, epidemiology, and the
latest developments in treatment, with a comparative analysis of
two commonly used antiepileptic drugs such as brivaracetam and
levetiracetam.
Methods
We carried out a cross sectional, multiple-response questionnaire
based survey among clinicians specialized in treating epilepsy patients
in the major Indian cities from June 2022 to December 2022.
Questionnaire:
The questionnaire booklet titled brivaracetam in epilepsy
management was sent to the physicians who were interested to
participate. The study questionnaire included 20 items about current
recommendations, clinical observations, and clinical experience of
specialists in the management of epilepsy. The study was conducted
after receiving approval from Bangalore Ethics, an Independent
Ethics Committee which is recognized by the Indian Regulatory
Authority, Drug Controller General of India.Participants:
Convenience sampling method was adopted where an invitation
was sent to leading clinicians who were expertise in managing
epilepsyin the month of March 2022 for participation in this Indian
survey. About 84 doctors from major cities of all Indian states
representing the geographical distribution shared their willingness
to participate and provide necessary data. Those physicians were
included and asked to complete the questionnaire without discussing
with peers. A written informed consent was obtained from each
neurologist’s prior initiation of the study. Clinicians who were
expertise in other specialities and were not provided informed
consent were excluded from the study.Statistical analysis:
The data were analyzed using descriptive statistics. Categorical
variables were presented as percentages to depict their distribution.
The frequency of occurrence and the corresponding percentage were
used to represent the distribution of each variable. To visualize the
distribution of the categorical variables, pie, and bar charts were
created using Microsoft Excel 2013 (version 16.0.13901.20400).Results
About 84 questionnaire booklets were distributed to clinicians,
in that 82 physicians completed questionnaires and were collected
personally by the study coordinators through the duration of 4 weeks.
The study indicated that the prevalence of epilepsy was mostly in the
range of 21-30 patients in a month as responded by 39% of target
doctors. Also, another 33% of respondents treat 11-20 patients in
an average month. Only 21% of doctors reported that they consult
a maximum of epilepsy of 31-40 cases per month. Less than 10 cases
were seen by 6% of the doctors.The study also reported that 65% of
respondents observed that epilepsy cases are most common in both
Rural and Urban. Incidentally, Rural population solely has more
cases 21% of epilepsy than urban with 13%.
Generalized tonic-clonic seizure (48%) and partial onset seizure
(48%) were the most common forms of epilepsy presented by the
patients during clinical practice. Myoclonic seizure was the least form
of epilepsy observed (5%). The study suggested that 49% of doctors
require an add on drug to 5-10 patients per month while 41% of
patients need add on drug therapy for 10-15 patients in a month.
Only 9% of doctors said that they need add on drug for epilepsy for less
than 5 patients. It was observed that 49% of doctors treat mostly 11-20
patients with partial onset seizure in their clinical practice, followed by
21% of respondents treat 21-30% of the patients who require an add
on drug for epilepsy. Another 22% of doctors see 6-10% of patients
who need an add on drug for epilepsy and 9% of doctors see only
less than 5% of epilepsy patients. Further, 56% of doctors consider
brivaracetam as the most preferred drug for newly diagnosed epilepsy
followed by levetiracetam by 27% of respondents, sodium valproate
by 10% and carbamazepine by 7% of the respondents[Figure 1].
The prescribing pattern of the study reported mostly, 38% of
doctors prescribe levetiracetam for 31-40% of partial onset seizure
patients which was the highest percentage prevalence. Another 33%
of doctors prescribed levetiracetam for 21-30% of the partial onset
seizure patients. On the other hand, only 15% of doctors prescribe
less than 40% and greater than 40% of partial onset seizure patients
are on Levetiracetam each. Also, the study observed that 39% doctors
conveying 21-30% of their patients treated with levetiracetam remain
uncontrolled. Another 35% of doctors observed that less than 10%
of their patients treated with levetiracetam remain uncontrolled. The
lowest incidences were reported by 18% of doctors at 11-20% and
7% of doctors at 31-40% of their patients treated with levetiracetam
remain uncontrolled.
Both behavioural and psychiatric adverse effects were the most
common reason for discontinuation of levetiracetam as suggested
by 55% of the respondents. Another 27% doctors attributed
behavioural adverse effects and 18% considered psychiatric adverse
effects as the reason discontinuation of levetiracetam. The study also
reported that 73%of doctors prescribe brivaracetam for the patients
failed on levetiracetam which was the maximum choice of the target
doctors. Oxcarbazepine of 12% and valproic acid of 10% were the
immediate choices of preference if Levetiracetam fails. Additionally,
40%of doctors reported their patients experiencing behavioural
changes with levetiracetam to 10-20% of their patients while 30% with
less than 10% of patients experiencing behavioral changes and 29%
have experienced with 20-30% of patients having behavioural changes
with levetiracetam.
When the study analyzed the response of doctors regarding
the percentage of patients experiencing behavioral changes with
levetiracetam shifted to brivaracetam, the study reported 38% of
doctors conveying behavioural changes with levetiracetam to 10-
20% of their patients while 23% have experienced with less than
10% of patients and 29% have experienced with 20-30% of patients

with behavioural changes with levetiracetam shifted to brivaracetam.
The study also revealed that 44% of doctors reported that 20-30%
of patients in their practice after shifted to brivaracetam from
levetiracetam has shown improvement in efficacy and behavioural
changes. Another 38% of doctors said 10-20% of patients in their
practice after shifted to brivaracetam from levetiracetam presented
improvement in efficacy and behavioural changes. The least number
of doctors reported that 15%of patients in their practice after shifting
to brivaracetam from levetiracetam had improvement in efficacy and
behavioural changes.
About 39% of doctors observed 30-50 patients with partial onset
seizure on brivaracetam in their clinical practice and another 38% of
doctors observed that less than 30 patients were with partial onset
seizure patients on brivaracetam in their clinical practice. Another
38% of doctors observed that less than 30 patients were with partial
onset seizure patients on brivaracetam in their clinical practice.
Nearly 77% of doctors confirmed that there were partial onset seizure
patients of brivaracetam on monotherapy in their clinical practice.
Only 23% of doctors responded contrarily on the same. About 39% of
doctors presented that they have put on the drug with 30-50 patients
as monotherapy and another 38% of doctors conveyed monotherapy
with less than 30.
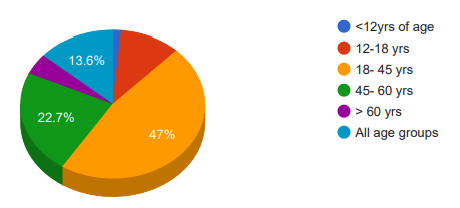
The study indicated that 47% of doctors opined that 18-45
years as the most common age group whom brivaracetam is being
prescribed. The next most observed age group was 45-60 years as
recalled by 23% of respondents [Figure 2]. Almost two third doctors
prescribe brivaracetam 100 mg/day in their clinical practice, only 17%
of doctors recommended 50 mg/day and 10% of doctors prescribed
75 mg/day.
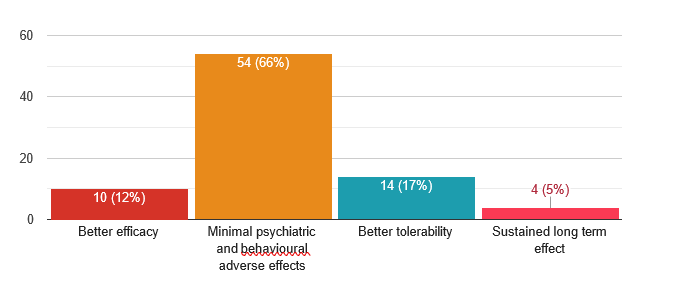
Almost two third doctors prescribe brivaracetam because of its
minimal psychiatric and behavioural adverse effects. Another 17%
of doctors prescribe brivaracetam due to its better tolerability and
12% due to its better efficacy. Sustained long term effect was the
least mentioned by the doctors by 5% of doctors[Figure 3]. As per
the study report, 34% of doctors opined that 21-30 individuals were
seizure free with brivaracetam as compared to levetiracetam whereas
30% of doctors consider 31-40 individuals were seizure free with
brivaracetam as compared to levetiracetam. Another 18% of doctors
consider less than 20 individuals were seizure-free with brivaracetam
as compared to levetiracetam in their clinical practice while only 16%
of doctors observed that more than 40 individuals were seizure-free
with brivaracetam as compared to Levetiracetam in their clinical
practice.
Discussion
The study indicated that a significant number of doctors in
India were managing epilepsy cases in their clinical practice. The
high number of cases highlighted the substantial burden of epilepsy
in the country, necessitating effective treatment strategies.The
overall prevalence (3.0-11.9 per 1,000 population) and incidence
(0.2-0.6 per 1,000 populations per year) data from recent studies in
India on general population were comparable to the rates of highincome
countries (HICs) despite marked variations in population
characteristics and study methodologies. There was a differential
distribution of epilepsy among various sociodemographic and
economic groups with higher rates reported for the male gender,
rural population, and low socioeconomic status. A changing pattern
in the age-specific occurrence of epilepsy with preponderance
towards the older age group is noticed due to sociodemographic and
epidemiological transition[9].
The study revealed that epilepsy was prevalent in both urban
and rural areas. However, it’s noteworthy that rural areas have a
slightly higher prevalence. This could be attributed to various factors
such as limited access to healthcare, lower awareness, and different
environmental influences. Based on the total projected population of
India in the year 2001, the estimated number of people with epilepsy
would be 5.5 million. Based on a single study on the incidence of
epilepsy, the number of new cases of epilepsy each year would be
close to half a million. Because rural population constitutes 74% of
the Indian population, the number of people with epilepsy in rural
areas will be approximately 4.1 million, three fourths of whom will
not be getting any specific treatment as per the present standard[10].
Generalized tonic-clonic seizures and partial-onset seizures were
the most commonly encountered forms of epilepsy in clinical practice.
Approximately 20-25% of cases were classified as generalized seizures
[11]. The findings of our study as reported form the physicians align
with global trends in epilepsy presentation.
The study suggested that a significant proportion of patients
require add-on drugs for epilepsy management. This highlighted
the challenges in achieving seizure control with monotherapy and
emphasized the importance of optimizing treatment regimens. On
a survival curve analysis, a comparative study done by Pipek et al.,
combination therapy was observed to be superior to levetiracetam
and lamotrigine monotherapies, and non-inferior to valproic acid
monotherapy. Patients without adequate seizure control with these
medications in monotherapy, benefited from combination therapy.
Combination therapy appears to retain efficacy for longer periods, as
suggested by Pipek et al.[12].
Levetiracetam remains a commonly prescribed drug for partialonset
seizures, and a substantial percentage of patients are on this
medication. However, it’s crucial to address the uncontrolled cases
and side effects associated with its use. With a unique mode of action,
levetiracetam has opened the door to a new and convincing treatment
option for epilepsy. Due to its favorable profile concerning ease of
use, almost complete lack of interactions, and excellent efficacy and
tolerability it has been globally established as one of the leading AEDs.
The development of BRV, its derivative, was completed some years
later. Compared with Levetiracetam, brivaracetam, that acts more
selectively at the synaptic vesicle protein 2A (SV2A) binding site,
offers typically better tolerability in relation to psychiatric adverse
events[13-15]. The authors and other studies found that in patients
with these adverse events, an immediate switch from Levetiracetam
to brivaracetam was easily achieved with a practical routine[16].
Behavioral and psychiatric adverse effects were identified as the
primary reasons for discontinuing levetiracetam. This underscores
the importance of monitoring and managing side effects in
epilepsy patients. Our study observed 38% of doctors conveying the
prevalence of behavioral abnormalities among patients. The results
were similar to Oluwaseun Ogunsakin et al. where they concluded as
though, the drug has a convenient dosing regimen and was relatively
well tolerated, neuropsychiatric side effects can emerge beyond the
initial titration period and may be the most common reason for
drug discontinuation. Levetiracetam has been reported to cause
varying degrees of psychiatric adverse effects including behavioral
disturbance such as agitation, hostility and psychosis, and mood
symptoms and suicidality[17].
A significant proportion of doctors opted for brivaracetam when
patients failed to respond to levetiracetam. This transition suggested
confidence in brivaracetam’s potential to improve seizure control and
minimize adverse effects. As suggested by L. Abraira et al., the safety
and tolerability, an overnight switching to brivaracetam was safe
and well tolerated. This treatment can improve levetiracetam-related
neuropsychiatric AEs [18].The study reported that many patients
experience improvement in both efficacy and behavioral changes
after shifting to brivaracetam. This outcome supported the clinical
utility of brivaracetam in challenging cases.
A substantial number of doctors prescribe brivaracetam as
monotherapy for partial-onset seizures. This approach aligns with
the goal of simplifying treatment regimens and enhancing patient
compliance. Doctors perceive brivaracetam advantages to include
minimal psychiatric and behavioral adverse effects, better tolerability,
and improved efficacy. These factors contribute to its popularity
among physicians. A notable percentage of doctors believe that more
individuals achieved seizure freedom with brivaracetam compared
to levetiracetam. This finding underscored brivaracetam potential to
offer improved outcomes for epilepsy patients[19-21].
Despite these advancements, challenges such as uncontrolled
seizures and medication-related side effects persist. Therefore,
ongoing research and clinical monitoring are crucial to further
enhance epilepsy management in India and improve the quality of
life for individuals living with this condition.
Conclusion
The study’s findings shed light on the current landscape of
epilepsy management in India. With a significant number of cases
being managed by healthcare professionals, there was an emerging
need for effective treatment options that can address the diverse
needs and challenges presented by epilepsy patients. Brivaracetam
has emerged as a preferred choice, especially for newly diagnosed
patients and those who do not respond adequately to levetiracetam.
Its perceived advantages, including minimal adverse effects and
improved efficacy, make it a valuable addition to the arsenal of
antiepileptic drugs. Lack of sufficient response to anti-epileptic drugs
are common in seizure patients. Combination therapy has gained
attention as add-on medications presented pronounced prognosis
in epilepsy management. The intervention of brivaracetam had
been observed with minimum adverse effects, better tolerability and
enhanced efficacy. An overnight switching to the drug produced
effective management and finer seizure control in patients. Response
from clinicians comply very well with trial reports. Further trials
and studies on interactions and adverse effects of the drug are highly
recommended.
Acknowledgement
We would like to thank all the clinicians who were participated
in this study
References
Citation
Manjula S, Krishna Kumar M. Perspectives on Epilepsy Management among Indian Clinicians: A Cross Sectional Study. Indian J Neurol. 04 2024;5(1): 128.