Case Report
A Case of Neuronal Hyperexcitability Syndrome
Jenix Nathan*, Shobana N, Sacratis, Selvakumar CJ and Sadeesh Kumar
Department of Neurology, Coimbatore Medical College Hospital, India
*Corresponding author: Jenix Nathan, Department of Neurology, Coimbatore Medical College Hospital India. E-mail Id: jenixnathan@gmail.com
Article Information: Submission: 24/09/2023; Accepted: 28/10/2023; Published: 31/10/2023
Copyright: © 2023 Jenix N, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Morvan syndrome is an autoimmune disorder characterized by
autoimmune antibodies directed against Voltage-gated potassium
channel (VGKC) [1]. Leading to peripheral nerve hyperexcitation
causing muscle cramps, myokymia, fasciculation, neuropathic pain
and dysautonomia. VGKC are transmembrane channels complexed
with various proteins, such as leucine-rich glioma-inactivated protein
1 (LGI1), contact in-associated protein 2 (CASPR2) and contactin
[2]. Morvans syndrome can be post-infectious, autoimmune,
paraneoplastic or could be aggravated by toxins too.
Case Report
13 years female presented with painful crampsand twitching
in bilateral forearms, hands, thighs, and soles along with excessive
irritability and decreased sleep she was apparently normal till 3
months back then developed, Subacute onset progressive painful
cramps involving back of thighs, forearms and both hands following
a fever episode. Fever was of high grade lasted for three days, not
associated with diarrhea, cough with expectoration, Headache altered
sensorium. Pain progressively increased in intensity with tremors and
palpitation. Patient also noticed Wide spread muscle twitching in both
upper and lower limbs. She also gave history of excessive sweating
in both palms and feet. Significant History of itching and peeling of
skin in both hands and feet since 1 month. Her mother gave history
of Excessive irritability and behavioral abnormality, decreased sleep,
only 2 -3 hours of sleep per day. No history suggestive of weakness
of limbs. No history suggestive of loss of pain touch sensation. No
history suggestive of unsteadiness or difficulty in coordination. No
history of altered bowel and bladder sensation. No history of difficulty
in speech. No history suggestive of cranial nerve involvement. No
history of LOC, Seizures, Trauma. General Examination Revealed
Patient conscious alert, peeling of skin noticed in palms and soles,
Hyperhidrosis noticed in palms and soles [Figure 1a,1b,2].
HMF examination showed normal status with a Mini Mental
Status Examination (MMSE-30/30). Cranial nerve examination
revealed no deficits. Motor examination of muscle tone, power
was normal and all DTR are present. Sensory examination was
normal. Coordination normal. Fasciculation seen in trunk and limbs
provisional diagnosis of neuromyotonia is made and case is worked
up

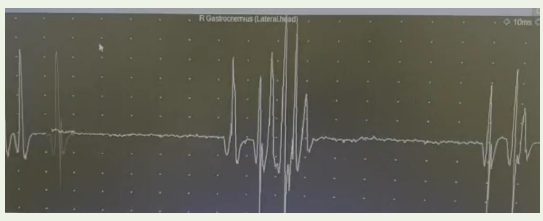
EMG was done and it showed myokymic potentials with couplet
and triplets.
ANA and ANCA – Negative
Antibody against Voltage Gated Potassium Channel (VGKC) revealed
Antibody to LGI 1-Positive
Antibody against CASPR - Positive
CT Chest and CT Abdomen done to rule out malignancy and revealed no malignancy.
MRI Brain and EEG was normal.
Treatment Given
IV steroids given for three days followed by
Intravenous Immunoglobulin 2g/kg body weight over five days.
Tab. Carbamazepine 200 mg BD
Symptoms relieved well following treatment and she was discharged.
ANA and ANCA – Negative
Antibody against Voltage Gated Potassium Channel (VGKC) revealed
Antibody to LGI 1-Positive
Antibody against CASPR - Positive
CT Chest and CT Abdomen done to rule out malignancy and revealed no malignancy.
MRI Brain and EEG was normal.
Treatment Given
IV steroids given for three days followed by
Intravenous Immunoglobulin 2g/kg body weight over five days.
Tab. Carbamazepine 200 mg BD
Symptoms relieved well following treatment and she was discharged.
Discussion
Autoimmune disorders directed against voltage gated potassium
channel include Neuromyotonia, limbic encephalitis and Morvans
syndrome.[3]
Morvan syndrome described by Auguste Morvan,the term “la chorιe fibrillare” was first used by the French physician Augustine Marie Morvan [4]. It is a rare autoimmune disorder withauto antibodies against voltage-gated potassium channels (VGKC)., primarily two kinds of potassium channel proteins, CASPR2 and LGI1 [5]. LGI1- Ab and CASPR2-Ab are associated with Morvans syndrome, LGI1- Ab is usually linked with limbic encephalitis (LE), faciobrachial dystonic seizures, hyponatremia, and REM sleep behaviour disorders [6]. Morvan syndrome serum are usually directed against LGI1, CASPR2, or both, but CASPR2-Ab dominates [7]. It has both CNS and PNS manifestation.CNS manifestation include- severe insomnia, irritability, encephalopathy, dysautonomia. PNS manifestation include-painful cramps, myokymia, fasciculations, neuropathic pain [8]. It may also present with systemic features such as weight loss, skin lesions or pruritus. LGI1 is also located particularly in the hippocampus and CASPR2 in the hippocampus and cerebellum [9]. In many cases Morvan syndrome is paraneoplastic, being especially associated with thymoma and small cell lung cancer but it can also occur in the absence of any cancer [10]. It can also be associated with myasthenia gravis.There was direct association with indigenous medicines, formulations based on herbs, heavy metals, and various colloids. Brain MRI and PET scan of Morvan syndrome are usually normal, while electroencephalogram (EEG) sometimes shows diffuse slow waves, occasional 4–6 Hz theta wave activity, and a typical rapid eye movement (REM) with absence of non-rapid eye movement sleep (NREM) stage [11]. Electromyography is useful in diagnosis of Morvan syndrome, which is characterized by spontaneous myofiber activity with various denervation potentials [12]. Usually remission occurs following immunotherapy, spontaneous remission is less likely even death can occur due to autonomic dysfunction in untreated cases.
Morvan syndrome described by Auguste Morvan,the term “la chorιe fibrillare” was first used by the French physician Augustine Marie Morvan [4]. It is a rare autoimmune disorder withauto antibodies against voltage-gated potassium channels (VGKC)., primarily two kinds of potassium channel proteins, CASPR2 and LGI1 [5]. LGI1- Ab and CASPR2-Ab are associated with Morvans syndrome, LGI1- Ab is usually linked with limbic encephalitis (LE), faciobrachial dystonic seizures, hyponatremia, and REM sleep behaviour disorders [6]. Morvan syndrome serum are usually directed against LGI1, CASPR2, or both, but CASPR2-Ab dominates [7]. It has both CNS and PNS manifestation.CNS manifestation include- severe insomnia, irritability, encephalopathy, dysautonomia. PNS manifestation include-painful cramps, myokymia, fasciculations, neuropathic pain [8]. It may also present with systemic features such as weight loss, skin lesions or pruritus. LGI1 is also located particularly in the hippocampus and CASPR2 in the hippocampus and cerebellum [9]. In many cases Morvan syndrome is paraneoplastic, being especially associated with thymoma and small cell lung cancer but it can also occur in the absence of any cancer [10]. It can also be associated with myasthenia gravis.There was direct association with indigenous medicines, formulations based on herbs, heavy metals, and various colloids. Brain MRI and PET scan of Morvan syndrome are usually normal, while electroencephalogram (EEG) sometimes shows diffuse slow waves, occasional 4–6 Hz theta wave activity, and a typical rapid eye movement (REM) with absence of non-rapid eye movement sleep (NREM) stage [11]. Electromyography is useful in diagnosis of Morvan syndrome, which is characterized by spontaneous myofiber activity with various denervation potentials [12]. Usually remission occurs following immunotherapy, spontaneous remission is less likely even death can occur due to autonomic dysfunction in untreated cases.
Conclusion
Multidisciplinary approach is recommended for the management
of such cases. Our case describes the importance of clinical
examination and highlights the importance of pattern recognition in
neurology.
References
Citation
Jenix N, Shobana N, Sacratis, Selvakumar CJ, Kumar S. A Case of Neuronal Hyperexcitability Syndrome. Indian J Neurol. 2023;4(1): 123.