Case Report
Paraneoplastic Limbic Encephalitis in Non-Hodgkin’s Lymphoma
Solav SV*, Shailendra VS, Khajindar GS, Rajlaxmi RJ, Hemant BR, Solav AS, and Suresh LB
Department of Nuclear Medicine, SPECTLAB, Nuclear Medicine Services, Sr No, 268, BavdhanBK, Pune. India
*Corresponding author: Shrikant V Solav, Department of Nuclear Medicine, SPECTLAB, Nuclear Medicine Services, Sr No, 268, Bavdhan BK, Pune. India. Email Id:drsolav1@gmail.com
Article Information: Submission: 23/09/2023; Accepted: 24/10/2023; Published: 27/10/2023
Copyright: © 2023 Solav SV, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Limbic encephalitis can be either non-paraneoplastic or paraneoplastic manifestation of various malignancies such as carcinoma of lung (small cell), ovary, breast, testis, GI tract, hepatobiliary etc. Patients usually present with acute or subacute onset of delirium, seizures, dementia, personality changes, etc. Differentiation between non-paraneoplastic and paraneoplastic limbic encephalitis is done by exclusion of malignancy. PET CT scan helps in detection of occult primary. Presented here is a case of paraneoplastic limbic encephalitis secondary to High grade B cell Non-Hodgkin’s lymphoma..
Introduction
Paraneoplastic limbic encephalitis is a type of paraneoplastic
neurological syndrome (PNS). It a non-metastatic manifestation that
does not occur secondary to any of associated complications such as
metabolic derangement, infection, nutritional imbalance or ischemia.
It is a cancer associated immune mediated disorder of the nervous
system that may precede the detection of malignancy by several
months. [1] The most commonly associated malignancies are that of
lung cancers, testicular tumours and breast cancers.
Non paraneoplastic limbic encephalitis is an autoimmune
disorder associated with antibodies to neuronal cell surface or synaptic
receptors. Common presentations include personality changes,
irritability, depression, seizures, confusion, memory loss, etc. CSF
usually shows elevated proteins, lymphocytes, immunoglobulin G.
CSF workup for limbic encephalitis may or may not be indicative of
an auto immune process.
Case report
A 68-year-old male, presented with a seizure and postictal
delirium. There was a preceding weight loss of 7kgs in 1 month. Clinical
examination revealed normal vital signs and obtunded mental status.
Rest of the examination was unremarkable.
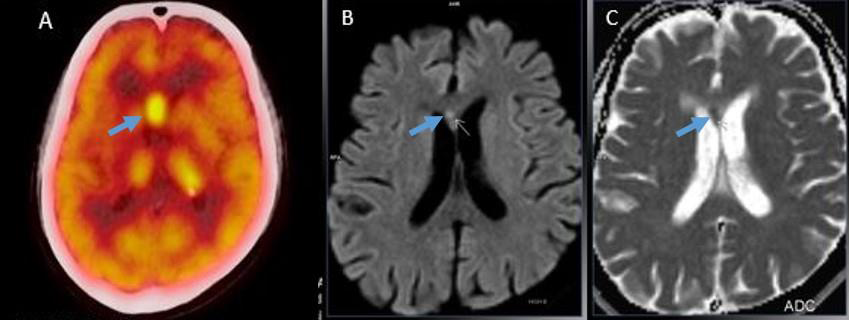
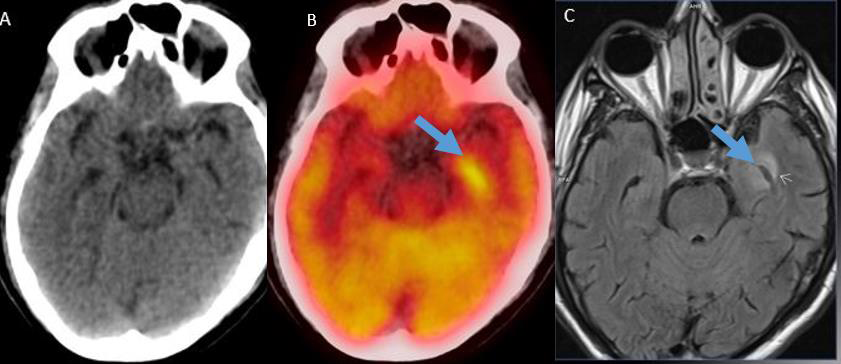
MRI brain showed focalaltered signal in the genu of corpus
callosum with restricted diffusion and asymmetric increased T2
hyperintense lesion in theleft mesial temporal lobe. FDG PET-CT
scan was done to look for occult primary. Brain images showed
increased FDG uptake in the genu of corpus callosum, left mesial
temporal lobe and caudate nucleus. The amygdala, head, body and
tail of hippocampus also showed increased FDG uptake (findings
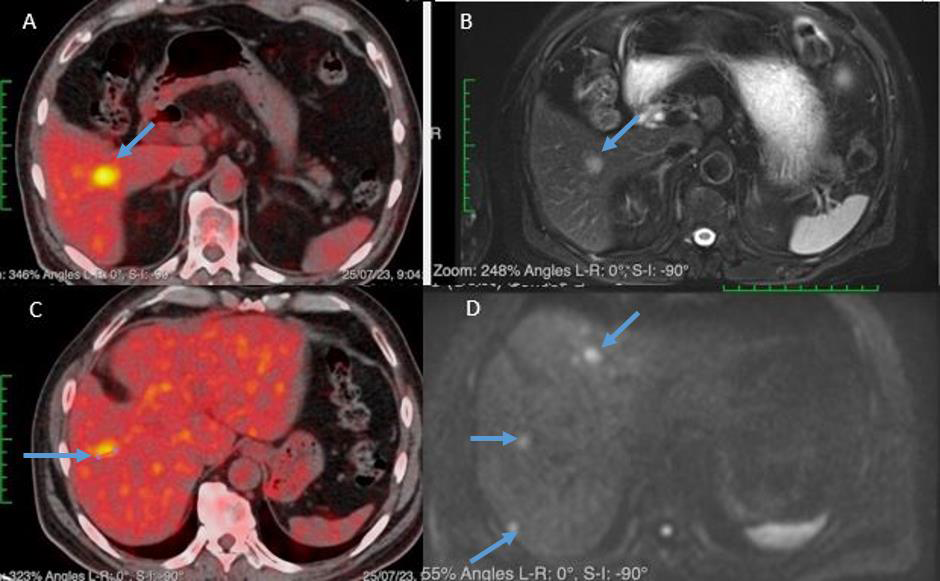
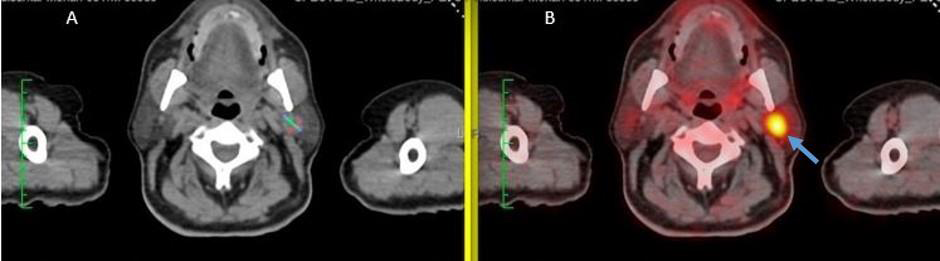
suggestive of limbic encephalitis). The wholebody images showed an
FDG avid lesion in the parotid and multiple FDG avid hypodense liver
deposits. MRI of liver revealed lesions in segments V, VII and VIII in
the right lobe, smaller lesions in the left lobe of liver with restricted
diffusion. Thus, a diagnosis of limbic encephalitis with occult primary
in left parotid was proposed with liver metastases. However, histology
from parotid lesion showed a benign lesion (Warthin’s tumor). Liver
biopsy was then done to reveal a diagnosis of Highgrade B- cell
lymphoma [Figure 1-4].
Discussion
Paraneoplastic syndrome is a set of signs and symptoms that are
expressed in the presence of a malignancy. The symptoms develop
when a malignant tumor causes changes in the body that are not
directly caused by cancer itself. Paraneoplastic syndromes may
affect different organ systems, most often the endocrine, neurologic,
rheumatologic, dermatologic and hematologic systems. The most
commonly associated malignancies include small cell lung cancer,
breast cancer, gynecologictumors and hematologic malignancies[2].
Paraneoplastic encephalomyelitis is a group of neurological
manifestations associated with cancer related inflammation of the
brain or spinal cord or both. Autoantibodies targeting intracellular
epitopes are thought to cross-react between cancer and central
nervous system proteins, glycoproteins, and complex carbohydrates.
Associated diseases can include limbic encephalitis, encephalomyelitis,
subacute cerebellar degeneration, opsoclonus myoclonus, optic
neuritis and rapidly progressive sensory polyneuropathy. [3]
Limbic encephalitis is of two broad types: Infectious and
autoimmune limbic encephalitis [4].
Infectious encephalitis (IE) and autoimmune encephalitis
(AE) are symptomatically similar, however essentially different in
pathogenesis.
Infectious limbic encephalitis is the inflammation of the limbic
areas of the brain preceded by an infection (mostly bacterial or viral).
Autoimmune encephalitis refers to acute to subacute, progressive
inflammation of the brain associated with antibodies against neuronal
cell surface and synaptic protein [5].
Autoimmune encephalitis is further divided into paraneoplastic
and non-paraneoplastic.
Non-paraneoplastic limbic encephalitis is an inflammatory
process which is due to antigen-specific cellular and humoral immune
responses directed towards CNS neurons (more specifically neuronal
surface antigens or extracellular antigens).
Paraneoplastic limbic encephalitis is a rare paraneoplastic
syndrome that affects the mesial temporal lobe and presents with
cognitive dysfunction, seizure, change in personality, irritability,
hallucinations, disorientation, and/ or disruption of consciousness
and short-term memory loss in presence of, or preceding a
malignancy. 50% of patients will have lung cancer, 20% will have
testicular tumours, and 8% will have breast cancer [6]. IgG antibodies
in the serum and CSF directed against intracellular neuronal antigens
(unlike non-paraneoplastic) are expressed by tumour cells and are
called onco-neuronal antibodies [7].
After thorough clinical examination, imaging plays a crucial role
in aiding the diagnosis of limbic encephalitis. MRI with contrast
is considered to be the most sensitive imaging modality. Limbic
encephalitis mostly involves the mesial temporal lobes and limbic
systems and is demonstrated by cortical thickening and increased T2/
FLAIR signal intensity of these regions. Bilateral involvement of the
structure is more common than unilateral.Whereas, FDG PET scan
will show increased metabolic activity in the corresponding areas [8].
There are only a few case reports of Lymphoma presenting as
limbic encephalitis. Senthil Rajappa, et al. explained paraneoplastic
limbic encephalitis secondary to primary renal lymphoma [9].
Dögel D, et al. [10] and Thuerl C, et al. [11] published case reports of Non-Hodgkins lymphoma presenting with paraneoplastic limbic
encephalitis.
Soto-Rincón CA et al. [12] have reviewed Ian Carr’s article
wherein the association between memory loss and Hodgkin’s
lymphoma has been given the eponym of Ophelia syndrome.
Our patient was suspected with occult primary in the parotid
gland. However, the histology from parotid lesion showed Warthin’s
tumor. Liver biopsy was then done to reveal a diagnosis of High grade
B- cell lymphoma.
Thus, concluding that the neurological manifestations were a
set of paraneoplastic symptoms secondary to High grade B- cell
lymphoma.
Acknowledgement
The authors would like to thank all the physicians involved in
management of above case for allowing FDG PET-CT and MRI
studies in management of their patients, the patients who readily
provided consent for the tests, the technologists at SPECTLAB who
acquired good quality images viz Ranjit Mahajan, Parag Deshmukh,
Bhagyashree Auti, Ramdas Kale, Prathamesh Harale, Paresh Raut,
Kshitija Londhe, Shivam Bhasme, Shivsurya Nair and the ethics
committee members who provided guidance in carrying out this
study.
References
Citation
Solav SV, Shailendra VS, Khajindar GS, Rajlaxmi RJ, Hemant BR, et al. Paraneoplastic Limbic Encephalitis in Non-Hodgkin’s Lymphoma. Indian J Neurol. 2023;4(1): 122.