Case Report
Vein of Galen Malformations- An Insight to Undo the ‘Gordian Knot’ of Surgeons by Neuro-Interventional Radiologist
Avi Agrawal, Chandrika Makker, Kritika Agrawal* and Shankey Garg*
Department of Radiology, MMIMSR, Mullana, India
*Corresponding author: Kritika Agrawal and Shankey Garg, Department of Radiology, MMIMSR, Mullana, India
Email: doctorkritika3@gmail.com
Article Information: Submission: 10/08/2023; Accepted: 31/08/2023; Published: 05/09/2023
Copyright: © 2023 Agrawal A, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Vein of Galen malformations are rare and unique congenital malformations of the cerebral vasculature. It is due to direct arteriovenous fistulous connection of misshapen arteries in brain with a persistent embryonic precursor of Vein of Galen (Median Prosencephalic vein of Markowski) instead of connecting with the capillaries. We are reporting 2 cases of VGAM. The first case is of a middle-aged man
with intractable occipital headache with features of VOGM. The second case demonstrates antenatal diagnosis of VAGM in association with ventriculomegaly and cardiomegaly in routine antenatal scan at 30 weeks of gestation in a twin pregnancy. Considering the rarity of these lesions, there are very few studies that have been able to adequately diagnose VOGM. Thus, making this study radically essential
for continuing developments in the diagnostic aspects of diagnosing and managing these lesions.
Keywords: Vein of Galen Malformation; Arterio-Venous Fistula; Median Prosencephalic vein of Markowski; Middle-aged man; Twin pregnancy; Congenital malformations; Gordian knot; Congestive cardiac failure; Cerebral Venous hypertension; Embolization; Misshapen arteries; Aneurysmal Dilatation; Endovascular therapy; Varix Aneurysm
Introduction
VGAMs are rare arterio-venous fistulas (AVFs) constituting
<1% of all cerebral vascular malformations & represent 30% of
symptomatic vascular malformations in the pediatric age group.
These lesions are characterized by the presence of arterio-venous
shunts keeping MPV patent and causing high flow/ pressure related
aneurysmally dilated large midline venous pouch just behind the 3rd
ventricle [1]. Steinheil in 1895, made the first reference to a Galenic
malformation-referring to it as a ‘varix aneurysm’ [2].
Though these lesions are uncommon, they are of special interest to
the interventional neuroradiologist because endovascular therapy [3]
has proved itself to be an effective, and often the only safe therapeutic
modality.
Case 1
A 35 year old male patient presented with headache in the occipital
region for past five months. Patient was being evaluated for occipital
headache when his vitals were within normal range and all routine
lab reports were normal. Physical examination evaluated GCS to be
15/15 and the ophthalmological examination was also normal. There
was no history of seizures, loss of consciousness, ENT bleed, vomiting
or any other weakness.
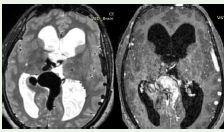
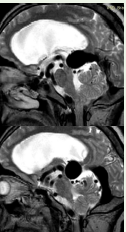
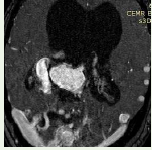
CEMR brain with MRA scan was performed, which revealed a
well-circumscribed T2W hypointense oval midline lesion measuring
approximately 30mm X 25mm X 23mm dorsal to the third ventricle
[Figure 1,2] in continuity with dilated straight sinus and dilated bilateral
transverse sinuses s/o Vein of Galen aneurysmal malformation with
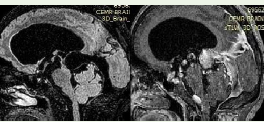
mass effect on midbrain causing compression of aqueduct resulting
in aqueductal stenosis and upstream hydrocephalus [Figure 3].
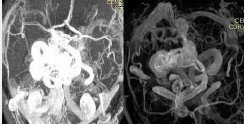
Multiple arterial feeders for VGAM originated from bilateral
PCAs and basilar artery [Figure 4]. It was drained by right internal
cerebral vein and right basal vein of Rosenthal with evidence of
multiple dilated venous channels from inferior sagittal sinus and
superficial cortical veins [Figure 5].
Due to the high rate of morbidity associated with VOGM, the
patient and his family members chose to continue on supportive
treatment and observation of VOGM.
Case 2
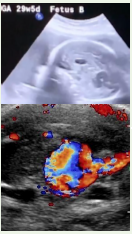
A 28-year-old pregnant woman presented for routine PNDT scan
at 30 weeks of gestation with twin pregnancy. On transabdominal
scan of fetus B, neuro-sonography revealed a tubular dilated anechoic
structure coursing from the splenium of the corpus callosum towards
the cisterna magna showing pulsatile and turbulent blood flow
draining through dilated falcine sinus and torcular herophili into
dilated transverse sinuses s/o Vein of Galen aneurysmal malformation
with mild cerebral ventriculomegaly (Figure 6). Cross-section of fetal
B’s chest demonstrated slightly enlarged area of fetal heart in relation
to area of chest s/o mild cardiomegaly. These findings of cerebral
venous hypertension & cardiomegaly were consistent with VOGM for
which counselling & neurosurgical consultation of parents was done.
Discussion
Development of the telencephalic choroid plexus is accompanied
by simultaneous differentiation of a transient venous structure which
drains the choroid plexuses & has been designated as MPV or the
primitive internal cerebral vein. By the 11th week, there is formation
of paired internal cerebral veins, which annex venous drainage of
choroid plexuses [6].
This results in the regression of the MPV, except for its most
caudal part, which joins the internal cerebral veins to form the vein
of Galen.
Principal feeders of the malformation are those that normally
supply the tela choroidea and the quadrigeminal plate. MPV, which
drains the shunt, lacks a fibrous wall and lies free in subarachnoid
space; therefore, it balloons out to a large size [7].
Prenatal ultrasound aids in identification of VGAM’s usually
in third trimester and its differentiation from other nonvascular
space- occupying lesions along with assessing the status of the fetal
cardiovascular system. It demonstrates the sonolucent venous sac
as a mass located posterior to the third ventricle with pulsatile flow
differentiating VOGMs from other midline cystic lesions [8].
Axial Brain CT scan demonstrates a well- defined, multilobulated,
intensely enhancing lesion within the cistern of velum interpositum.
Diffuse cerebral atrophy, periventricular white matter hypodensities
& dilated ventricular system are associated with features of cerebral
parenchymal damage.
Angiography remains the gold standard for evaluation of small
feeders supplying the fistula, as well as the dynamic aspects of venous
drainage of the normal brain and AV shunt [9].
MRI is the modality of choice for VOGMs, demonstrating the
location of fistula, presence of any nidus and relationship between the
different pathological arterial & venous components. MR angiography
is used as a noninvasive alternative to diagnostic angiographic studies
[10].
VOGMs are also associated with the Turner syndrome,
blue rubber bleb syndrome, supernumerary digits, hypospadias,
transposition of great vessels, aortic stenosis and right-sided aortic
arch [11].
Aggressive medical management postpones intervention until
the child is about 5 - 6 months, when intervention is easier and safer
[12]. Congestive cardiac failure (CCF) in a neonate that is refractory
to medical treatment is an indication for emergency embolization.
In neonates not presenting with cardiac failure, the aim would be
to prevent consequences of cerebral venous hypertension and thus
promote normal cerebral development [13]. AV fistulas are occluded
on the arterial side, using embolic agents such as coils, cyanoacrylates
and detachable balloons.
Conclusion
The varied and life-threatening clinical presentations and
distinctive complex angioarchitecture of VOGM makes it essential
for their early diagnosis; allowing a caring physician to understand
their embryological and pathophysiological aspects. Management of
these lesions – both in the prenatal/neonatal period and at the time
of definitive intervention, is challenging. Thus, in near future and at
current scenario; role of imaging is essential in making these lesions
now potentially curable with better prognosis & low morbidity.
References
Citation
Agrawal A, Makker C, Agrawal K, Garg S. Vein of Galen Malformations- An Insight to Undo the ‘Gordian Knot’ of Surgeons by Neuro-Interventional Radiologist. Indian J Neurol. 2023; 4(1): 118.