Case Report
Osteochondroma of Occipital Bone Projecting into Foramen Magnum, A Rare Site for a Common Tumor-A Case Report
Gunjan Jindal, Amit Shrivastava*, Akarshit Mahajan and Maichael Goodwin
Department of Radiodiagnosis, MMIMSR, Mullana, Haryana, India
*Corresponding author: Dr. Amit Shrivastava, Assistant Professor, Department of Radiodiagnosis, MMIMSR, Mullana, Haryana, India E-mail- dr.amitsrivastava@gmail.com Phone No- +919100750718
Article Information: Submission: 04/08/2023; Accepted: 25/08/2023; Published: 28/08/2023
Copyright: © 2023 Jindal G, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
A 15 year old male with no comorbidities presented with complaints of electric shock like sensation in nape of the neck associated with dizziness, involuntary movement in right upper limb and occasional headache presented to neurology department. On investigations, osteochondroma arising from occipital bone was diagnosedwhich was projecting into foramen magnum causing severe compression of spinal cord. Only one such case has been described previously in literature. The patient was successfully treated with surgery and had relief of symptoms on follow up.
Keywords: Osteochondroma, Occipital bone, Foramen magnum, Spinal cord compression
Introduction
The appearance of an osteochondroma in the form of an
intracranial tumour is a very rare phenomenon. These tumours
show a predilection for the base of the skull, probably due to
the presence of numerous synchondroses there [1]. Although
intracranial osteochondromas are known to cause neurological
deficits, intracranial osteochondromas with neurological deficits
are very rare and the literature contains only sporadic case reports.
Osteochondromas are benign, cartilage-covered bone tumours that
protrude from the outer surface of the bone and contain a medullary
cavity that is continuous with the underlying bone [2]. These tumours
grow slowly and malignant transformation is rare; however, they
can affect local structures such as nerves, blood vessels or tendons
and sometimes cause cosmetic problems. Osteochondromas are
true tumours arising from endochondral ossification during skeletal
development, usually in the metaphyseal regions of long bones.
Continued growth of the lesion results in subperiosteal bone growth
with a cartilaginous cap protruding from the bone surface. The bony
prominence of an osteochondroma, whether sessile or pedunculated,
merges into the underlying bony cortex and medullary cavity [3].
Case Presentation
A 15 year old male with no comorbidities presented with
complaints of electric shock like sensation in nape of the neck
associated with dizziness, involuntary movement in right upper
limb and occasional headache since 20 days. There was no history of
vomiting, limb weakness, altered bowel/bladder habits or any trauma.
On examination, GCS was E4V5M6 and there were no deficits, nerve
palsies or cerebellar signs. All the routine investigations were within
normal limits.
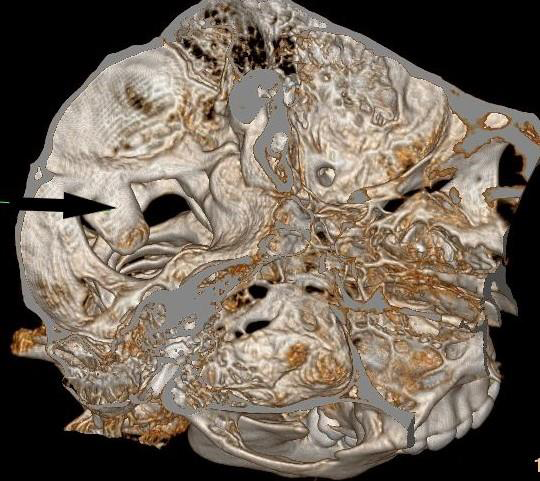
A non-contrast CT scan of patient’s head showed a bony
projection along posterior aspect of foramen magnum protruding
into the spinal canal, which was given as osteochondroma [Figure 1].
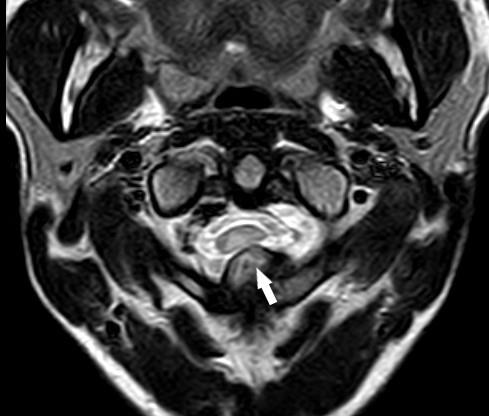
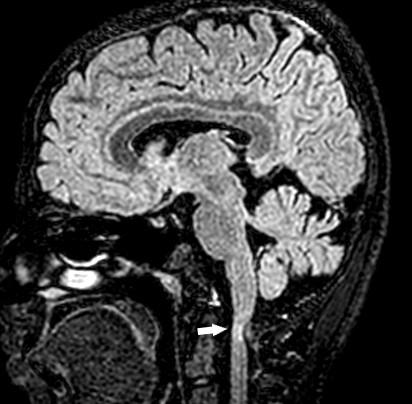
MRI of brain demonstrated a 3.8cm x 1.3cm pedunculated bony outgrowth from occipital bone causing compression at foramen magnum with altered signal intensity in spinal cord [Figure 2,3].
A Multidisciplinary team decision was made to excise the mass. Intraoperatively a bony lesion arising from the posterior part of foramen magnum rim was identified and drilled out and sent for histopathological examination. The post-op period was uneventful. On follow up, patient had relief of symptoms with complains of occasional headache.
Histopathology report demonstrated an osteogenic lesion with a hyaline cartilaginous cap. The lesion was composed of lamellar bone with fatty intertrabecular marrow spaces. No evidence of malignancy was noted. Overall features were suggestive of an osteochondroma.
MRI of brain demonstrated a 3.8cm x 1.3cm pedunculated bony outgrowth from occipital bone causing compression at foramen magnum with altered signal intensity in spinal cord [Figure 2,3].
A Multidisciplinary team decision was made to excise the mass. Intraoperatively a bony lesion arising from the posterior part of foramen magnum rim was identified and drilled out and sent for histopathological examination. The post-op period was uneventful. On follow up, patient had relief of symptoms with complains of occasional headache.
Histopathology report demonstrated an osteogenic lesion with a hyaline cartilaginous cap. The lesion was composed of lamellar bone with fatty intertrabecular marrow spaces. No evidence of malignancy was noted. Overall features were suggestive of an osteochondroma.
Discussion
Osteochondromas are not true neoplasms, rather they are
developmental lesions and hence also called as osteocartiagenous
exostosis. Osteochondroma is the most common tumour of the bone,
and it occurs mostly in the epiphysis of the long bones. The key feature
of osteochondromas is that they are in continuity with the parent bony
cortex and medullary canal. They can be sessile or pedunculated and
typical feature is that they grow away from the epiphyses of the parent
bone. A cartilaginous hyaline cap is present which if grows more than
1.5 cm in thickness suggest malignant transformation. Malignant
transformation is a rare complication and occurs only in about 1% of
patients with solitary osteochondroma.Although osteochondromas
are the most common benign tumour of skeletal bones, they are rare
in the skull and the incidence of intracranial osteochondromas ranges
from 0.1% to 0.2% of all intracranial tumours [4,5]. It is possible that
the true incidence of cranial osteochondromas is underrepresented
due to their often asymptomatic nature. An osteochondroma can
become symptomatic from mechanical irritation of the cranial nerves,
soft tissue, or vascular compression, trauma, or fracture [6]. As in the
case described, the presence of a tumour in the foramen magnum can
be recognized immediately on the basis of neurological symptoms.
Osteochondromas can be single or multiple; The latter is
associated with an autosomal dominant inherited syndrome called
hereditary multiple exostosis (HME). HME demonstrates almost
complete penetrance especially in males and are mostly diagnosed in
early childhood by the age of 10-12 years. In addition to cosmetic
deformities, features such as fractures, vascular involvement,
neurological sequelae, overlying bursa and malignant changes are
rarely observed [7].
Osteochondromas rarely arise in the skull and very few
cases have been reported. Only sporadic case reports of skull
base osteochondroma are available in literature. Most of these
osteochondromas presented with cranial nerve palsies. However, in
our case the osteochondroma arising from occipital bone was causing
compression at cervicomedullary junction. We could find only 1 case
of basi-occiput osteochondroma growing into foramen magnum
similar to our case.In this case the patient presented with gradual
gait difficulty,weakness of all the limbs and persistent dull pain in the
occipitocervical region [8].
Other bone lesions to consider in the differential diagnosis
include meningiomas, monostotic fibrous dysplasia, osteomas,
osteoblastomas, osteoblastic metastases, giant cell tumours, and
eosinophilic granulomas.
Surgical resection is the only treatment for these lesions and is
recommended in patients with symptomas related to osteochondroma
or in patients in whom malignant transformation is suspected [9].
Conclusion
Osteochondromas are the most common benign bone tumours,
but are extremely rare in the skull. Although osteochondromas rarely
become malignant and are usually asymptomatic, they should be
included in the differential diagnosis of skull tumours. Comprehensive
imaging, including CT and MRI, along with histopathological evaluation is essential for accurate diagnosis and optimal patient management. Despite potentially catastrophic symptoms, these
tumours are pathologically benign and complete resection often
results in a long-term cure.
References
Citation
Jindal G, Shrivastava A, Mahajan A, Goodwin M. Osteochondroma of Occipital Bone Projecting into Foramen Magnum, A Rare Site for a Common Tumor-A Case Report. Indian J Neurol. 2023;4(1): 117.