Research Article
A Study of Factors Affecting Surgical Outcome In Patients of Idiopathic Normal Pressure Hydrocephalus Treated With Programmable Ventriculoperitoneal Shunt
Rana A1, Ghimire N2*, Sing H3 and Sing D3
1Department of Neurosurgery, Consultant Neurosurgeon Mathura, India
2Department of Neurosurgery, Lecturer, Neurosurgeon, Nepalgunj Medical College Kohalpur-5, Banke, Nepal
3Department of Neurosurgery, Fifth floor, A block, GIPMER, Delhi India
*Corresponding author: Ghimire N, Department of Neurosurgery, Lecturer, Neurosurgeon, Nepalgunj Medical College Kohalpur-5, Banke, Nepal Email: nirajghimirebarca@gmail.com
Article Information: Submission: 17/11/2022; Accepted: 28/07/2023; Published: 31/07/2023
Copyright: © 2023 Rana A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction: A triad of symptoms: gait disorder, cognitive impairment, and urinary incontinence with communicating Hydrocephalus and normal CSF pressure define the Normal Pressure Hydrocephalus (NPH). iNPH has reported incidence between 0.5–5.5 cases per 100,000 per year Secondary NPHoccurs after head trauma, subarachnoid hemorrhage, or other brain insults. When no such predisposing factors are identified, the syndrome is idiopathic NPH (iNPH).
Aims and Objectives: The aim and objective of the study was1)To assess surgical outcome after programmable ventriculoperitoneal shunt in idiopathic NPH and, 2) To assess relation of opening pressure of ventricle with surgical outcome and functioning of programmable VP shunt in idiopathic NPH.
Methodology: A prospective observational study was done in the Department of Neurosurgery, GIPMER, for one year after obtaining institutional ethical clearance among 15 patient who meet diagnostic criteria for idiopathic NPH according to international guidelines for NPH 2008. The collected data were entered in Microsoft Excel. Data were analyzed and statistically evaluated using the SPSS-PC-25 version.
Results: A total of 15 patients were included in the study. The mean age of the patient was 67.53±3.18 years. There were 13 (86.7 %) males and 2 (13.3%) females. The mean duration of gait abnormalities, urinary incontinence, and dementia were8.80 ±3.55, 7.07 ±2.66, and 5.87 ±2.23 months respectively.
Conclusion: Rapid establishment of optimum programmable pressure valve setting improve patient outcome as well as reduce medical cost by preventing over drainage and shortening hospitalization time
Aims and Objectives: The aim and objective of the study was1)To assess surgical outcome after programmable ventriculoperitoneal shunt in idiopathic NPH and, 2) To assess relation of opening pressure of ventricle with surgical outcome and functioning of programmable VP shunt in idiopathic NPH.
Methodology: A prospective observational study was done in the Department of Neurosurgery, GIPMER, for one year after obtaining institutional ethical clearance among 15 patient who meet diagnostic criteria for idiopathic NPH according to international guidelines for NPH 2008. The collected data were entered in Microsoft Excel. Data were analyzed and statistically evaluated using the SPSS-PC-25 version.
Results: A total of 15 patients were included in the study. The mean age of the patient was 67.53±3.18 years. There were 13 (86.7 %) males and 2 (13.3%) females. The mean duration of gait abnormalities, urinary incontinence, and dementia were8.80 ±3.55, 7.07 ±2.66, and 5.87 ±2.23 months respectively.
Conclusion: Rapid establishment of optimum programmable pressure valve setting improve patient outcome as well as reduce medical cost by preventing over drainage and shortening hospitalization time
Keywords: INPH; Valve setting; Ventriculoperitoneal shunt
Introduction
In 1964,Doctor Salomon Hakim described a syndrome of
symptomatic Hydrocephalus with normal cerebrospinal fluid (CSF)
pressure.[1] A triad of symptoms: gait disorder, cognitive impairment,
and urinary incontinence with communicating Hydrocephalus and
normal CSF pressure define the Normal Pressure Hydrocephalus
(NPH). [2] Secondary NPH occurs after head trauma, subarachnoid
hemorrhage, or other brain insults.[3] When no such predisposing
factors are identified, the syndrome is idiopathic NPH (iNPH) [4].
iNPH has reported incidence between 0.5–5.5 cases per 100,000
per year.[5,6,7] The ventriculoperitoneal shunt is the primary
treatment in the management of iNPH.The programmable valve shunt
is commonly used for NPH nowadays. The valves in programmable
shunt are programmed and reset at the bedside, possibly reducing
the need for surgical revision. [3] Theoretically, after shunt,
there is reduced strain on ventricle walls, better perfusion, and possibly reestablishment
of functions. Hemodynamic assessments have shown
that this is better in the case of iNPH. [4,7] The relation between
perfusion and function and the growing complexities of the neural
network following shunting is another theorized declaration.[5,6,8]
Ventriculoperitoneal Shunt may cause under or over-drainage. If the
valve pressure is low, excess drainage may tear subdural veins leading
to subdural hematoma or hygroma [9-11].
Aims and Objectives:
1) To assess surgical outcome after programmable ventriculoperitoneal
shunt in idiopathic NPH
2) To assess relation of opening pressure of ventricle with surgical
outcome and functioning of programmable VP shunt in
idiopathic NPH.Materials and Methods
The prospective observational study was done in the Department
of Neurosurgery, GIPMER, for one year after obtaining institutional
ethical clearance.
Inclusion criteria: Patient meet diagnostic criteria for idiopathic
NPH according to international guidelines for NPH 2008.
Exclusion criteria: Patients with pace maker
Outcome variable: Opening pressure of ventricle, Mini-mental
state examination score (MMSI), Japanese scale score (JSINPH),
Evans index, Callosal angle, and Final setting of programmable shunt.
Sample size calculation: As per Convenience, sample size was 15.
Patients with typical clinical features: urinary incontinence, gait
disturbance and dementia and compatible image findings suggesting
iNPHhad a preoperative assessment which consists of Mini-Mental
State Examination (MMSE), Japanese Scale for Idiopathic Normal
Pressure Hydrocephalus (JSINPH), Evans ratio and Callosal angle. The
MMSE is a test introduced by Folstein in order to evaluate the general
patterns of dementia disorders. The JSINPH is a tool to access the
patients’ clinical background. It measures the three main symptoms
in different degrees of presentation, and can be easily performed in
the preoperative period and as an evaluation questionnaire and in the
follow-up of the patients. Patient then underwent Tap Test (TT) in
which 40 ml of CSF was drained by lumbar puncture. Gait assessment
was done 3 hours and 72 hours after the T.T.
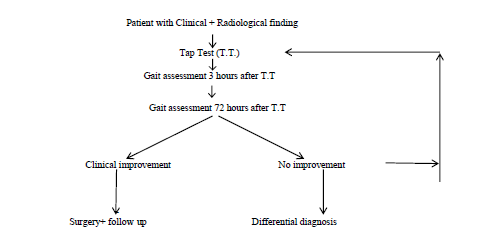
The patient who had improved gait following tap test underwent
ventricular peritoneal shunt (CODMAN) through an externally
adjustable magnetic radiopaque with anti-siphoning valve a
programmed to different drainage pressure.
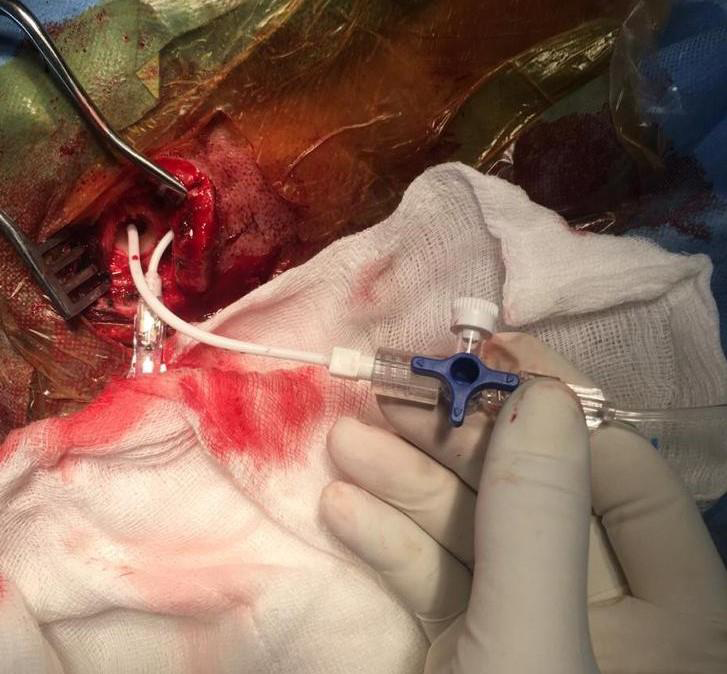
After making burr hole, dura was cut and coagulated as per
standard method of ventricular tap. In order to prevent initial CSF
drainage, a three-way connector (TWC) was attached with the
proximal end of Ventricular puncture cannula. TWC was attached to
cutter line and the pressure recorded as per illustration [Figure 1,2]

The initial valve level was set according to the opening pressure
of the ventricle. The MMSE, JSINPH, Evans ratio and Callosal angle
were reassessed after 15 days. Patient who had underdrainage or over
drainage underwent valve pressure readjustment. Patients were kept
in 15 daysfollow up in first three months and then quarterly follow
up. The last follow up was done at nine months. The decision of
final pressure set point was made based on clinical and radiological
outcome variables: MMSE, JSINPH, Evans ratio and Callosal angle.
Data entry and statistical analysis:
The collected data were entered in Microsoft Excel. Data were
analyzed and statistically evaluated using the SPSS-PC-25 version.Quantitative data were expressed in mean±standard deviation and depended on normality distribution difference between two comparable groups tested by students’ t-test (unpaired) or Mann Whitney’U’ test while comparing before and after treatment data Paired t-test or Wilcoxon sign rank test was used. Qualitative data were expressed in percentage. P’ value less than 0.05 was considered statistically significant.

Results
A total of 15 patients were included in the study. The mean age of
the patient was 67.53±3.18 years. There were 13 (86.7 %) males and
2 (13.3%) females. The mean duration of gait abnormalities, urinary
incontinence, and dementia were8.80 ±3.55, 7.07 ±2.66, and 5.87
±2.23 months respectively.
Discussion
Till date, a lot of research work has been done to calculate
the reference set point of PPV, but most of them have not been a
reliable option. There is a paucity of research work that has shown
an association between PPV set point based on opening pressure and
clinical and radiological outcomes. There are no specific criteria or
consensus made regarding when to call good outcomes and when
to call poor outcomes based on clinical and radiological parameters.
In our study, we tried to relate ventricular opening pressure to the
clinical and radiological outcome, and attempted to define the
reference cut to call good or poor clinical and radiological outcomes.
Duration and severity of symptoms were inversely proportional
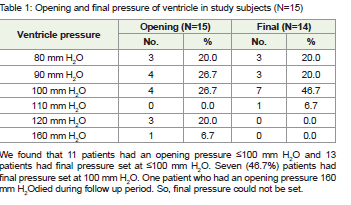
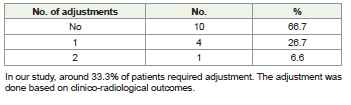
to the clinical and radiological improvement of the patient. In our
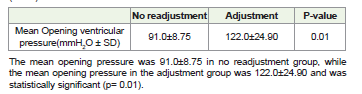
study, 33.3% of patients required adjustment in the PPV setting, and
most patients (7) had final pressure set at 100 mm H2O. The mean
opening pressure was 91.0±8.75 in no readjustment group, while the
Patient with opening pressure between 80 to 100 mm H2O, mean preop MMSE
was 21. Whereas it was less than 20 when opening pressure was above 120 mm
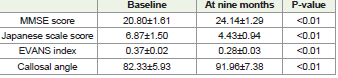
H2O. Following surgery, mini-mental score improved in all 14 cases with mean
increase in MMSE score was 2.65±1.20.The Japanese score has improved in all
14 cases who completed the study. The mean decrease in score was 1.92±0.95.
The Evans ratio has decreased in all cases who completed the study. The mean
decrease in the EVANS ratio was 0.081±0.05.At nine months, the callosal angle
has increased in all cases who completed the study following Programmable
VP shunt. The mean increase in the callosal angle at nine months duration was
10.62±2.36.All 14 patients who survived had significant clinical and radiological
improvement (P<0.01).
In our study, 13 patients had no complication. One patient developed subdural effusion, which was managed conservatively by increasing PPV pressure by 20 mm H2O.One patient showed no improvement even after two readjustment of ventricular pressure and died.
In our study, 13 patients had no complication. One patient developed subdural effusion, which was managed conservatively by increasing PPV pressure by 20 mm H2O.One patient showed no improvement even after two readjustment of ventricular pressure and died.
mean opening pressure in the adjustment group was 122.0±24.90 (p= 0.01). The improvement in both clinical and radiological outcome variables at 9 months were statistically significant (<0.01).
The classic triad of iNPH was present in all our patients while
literature showed triad to be in only 33%. [12] We observed gait
abnormalities to be the first symptoms to occur, followed by urinary
incontinence and then dementia, consistent with the literature data.
While there is no level I evidence on shunt surgery, several studies
have reported a beneficial outcome after shunt surgery in most
selected patients. We performed programmable VP shunt in all our
patients after calculating the risk-benefit ratio and PPV setting was
done based on ventricular opening pressure.
There are various techniques available in the literature for
programmable pressure valve setting. Preoperative CSF dynamics test
used by O Tsuji and K Sato in 1998. [13] In 2000, Miyaki et al gave a
new concept for the pressure setting of a programmable pressure valve
by measuring vivo shunt flow performed using a micro flow meter.
[14]A study by Zemack et al in 2002used adjustable valves in normal pressure
Hydrocephalus. In their study, the opening pressure setting
was decided based on the patient’s age, the duration of the underlying
disease, the size of the ventricles, and the curve profile, amplitude,
and opening pressure findings derived from a constant manometric
lumbar infusion test. In their study, the high (140–180 mm H2O)
opening pressure level was selected to avoid subdural hematomas in
elderly patients. [15] In 2008, Miyaki et al concluded QRT which was
reliable for reducing over-drainage complications and medical costs.
The readjustment rate was 40%. [16] In contrary, the readjustment
rate was 33.3% in our study. Kim et alkept initial valve-opening
pressures from 30 to180 mm H2O (mean, 102 ± 27.5 mm H2O) while
we set valve opening pressure based on ventricular opening pressure.
There were 154 adjustments in 81 operations (mean, 1.9 times) while
only five patients in our study needed readjustment, among which
4 improved after a single adjustment and one patient expired after
two adjustments. In Kim’s study, around 84% of patients improved
completely. There were 18 (22%) major complications: 7 subdural
hygroma, six shunt obstructions, and five shunt infections [17]. We
had 2 patients who developed complications among whom one
patient improved by increasing pressure setting by 20 mm H2O and
one patient died. In 120 patients, Ma and Sharma et al set Medtronic
Strata Adjustable Pressure valve set at 1.5 [18]. Patients had an
adjustment rate of 0.5 per follow-up visit to achieve the best clinical
outcome and avoid complications. Out of the improved 71 patients,
only 24% improved in all three symptoms while in our study all three
symptoms improved in all 14 survived patients. They needed valve
pressure adjustment at least once in 85 patients (mean number of 1.68
adjustments). In contrast, only 5 of our patients needed adjustment,
among whom four patients improved after a single adjustment. The
complications rate was 40% in Ma and Sharma’s study, while only 2 of
our patients developed a complication. They followed up the patients
for up to 19 months while we followed up only for nine months.
Our study showed opening valve pressure based on opening
ventricular pressure provides a better clue about the final pressure
setting in iNPH. Various studies have considered the improvement
in MMSE by 4 points, JSI by two scores, final callosal angle (>90degrees) and Evans index <0.3 to be good outcomes, but none of
those literature has compiled all four above mentioned clinical and
radiological tools to define the criteria of good outcome in postoperatively.
We considered the improvement in MMSE by 3 points,
JSI by two scores with final callosal angle (>90 degree)and Evans
index <0.3 to a good outcome. Nearly all our patients showed good
outcomes. Surprisingly, only 5 out of 15 patients required to readjust
the valve pressure.
We followed our patient up to 9 months, unlike other studies
that followed their patient for more than a year. The literature has
shown that over time these improvements start to regress. Larger
studies with longer follow up needed to support our evidence that
PPV setting based on ventricular opening pressure is more reliable
and effective technique while considering programmable VP shunt
in iNPH.
Limitations: Our Study was a single centre study. The sample size
was relatively small. The follow -up period of our study was 9 months.
Conclusion
The readjustment rate after setting the initial programmable
pressure valve according to opening ventricular pressure is 33%.
The factors affecting good outcome in patients of NPH are younger
age group, less duration and severity of symptoms, good preop
MMSE, less degree of ventricular dilatation. We also concluded that
improvement in MMSE by 3 points, improvement in JSINPH score by
2 score, final callosal angle >90 degree and final Evans ratio <0.3 could
be considered as good outcome and all these combined reference level
could give us idea when to stop readjustment. Rapid establishment
of optimum programmable pressure valve setting improve patient
outcome as well as reduce medical cost by preventing over drainage
and shortening hospitalization time. Larger studies with longer
follow up needed to support our evidence that PPV setting based on
ventricular opening pressure is more reliable and effective technique
while considering programmable VP shunt in iNPH.
References
Citation
Rana A, Ghimire N, Sing H, Sing D. A Study of Factors Affecting Surgical Outcome In Patients of Idiopathic Normal Pressure Hydrocephalus Treated With Programmable Ventriculoperitoneal Shunt. Indian J Neurol. 2023;4(1): 116.