Case Report
A Rare Case of Bilateral Duane’s Retraction Syndrome with Crocodile Tears, Hearing Loss, and Klippel Feil Syndrome (Wildervanck Syndrome)
Ravichandran R*, Lenin Shankar P and Ravi Kumar V
Department of Neurology, Thanjavur Government Medical College, Tamilnadu, India
*Corresponding author: Ravichandran R, Department of Neurology, Thanjavur Government Medical College, Tamilnadu, India
Article Information: Submission: 13/06/2023; Accepted: 11/07/2023; Published: 15/07/2023
Copyright: © 2023 Ravichandran R, et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
The Duane syndrome is a strabismus syndrome which is characterized by congenital non-progressive horizontal ophthalmoplegia which primarily affects the abducens nerve. Approximately 70% of the individuals with the Duane syndrome have an isolated disease and 30% of cases are associated with other congenital anomalies. A triad of Klippel–Feil anomaly Duane retraction syndrome, and hearing deficits is Wildervanck syndrome the estimated the prevalence is less than 1/1,000,000. We are presenting here, 26 year old male with a very rare case of bilateral Duane syndrome with hearing loss and klippel feil anomaly possible Wildervanck syndrome along with
addition feature of crocodile tears.
Keywords: Case report; Duane’s retraction syndrome; Klippelfeil syndrome; Wildervanck syndrome
Introduction
Duane Retraction Syndrome, is a congenital and non-progressive
strabismus syndrome characterized by complete or less often partial
absence of abduction, retraction of globe on adduction and narrowing
of palpebral fissure during adduction (induced ptosis) [1]. Advanced
neuroimaging, muscle electrophysiology and genetic analysis gave
better understanding of this form of strabismus, now considered a
congenital cranial dysinnervation disorder (CCDD), giving better
insights into the management of this challenging syndrome. This
may be primary due to absence of normal innervation or secondary
following aberrant innervations from other cranial nerves. CCDD
is a non-progressive entity and may also have associated bony
abnormalities [2].
Types of DRS (Hubers) [3]
Type 1 (70%–80%): Marked limitation of abduction with
minimally defective or normal adduction, globe retraction and
palpebral fissure narrowing in adduction, widening in abduction.
Type 2 (7%): Marked limitation of adduction with primary
position exotropia of the affected eye abduction normal or slightly
limited with globe retraction and palpebral fissure narrowing in
attempted adduction.
Type 3 (15%): Limitation or complete absence of adduction and
abduction with globe retraction and palpebral fissure narrowing in
attempted adduction.
Case Presentation
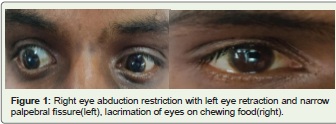
A 26-year-old male with history of horizontal eyeball movement
limitation of the both eyes since birth, profuse lacrimation of both
eyes when eating food since childhood. His birth, developmental
and family history were normal. On examination his best corrected
visual acuity was found to be 20/20 in both eyes. He had -3 abduction
deficit in both eyes and retraction of the globe and fissure-narrowing
on adduction in the both eyes. He also had short neck (height neck
ratio 14), bilateral high frequency hearing loss without anatomical
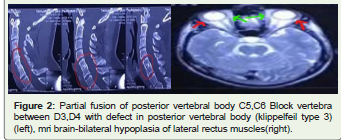
malformation. Other neurological examinations were normal.MRI
brain shows bilateral abducens nerve absent and smaller volume of
the bilateral lateral rectus muscles. CT spine shows partial fusion of
posterior vertebral body C5,C6 and blocked vertebra between D3,D4
with defect in posterior vertebral body (klippelfeil type 3) [Figure 1,2].
Discussion
Myofibers of extraocular muscles (EOM) are developed by a
condensation of the mesoderm around the eye. When the embryo
is 7 mm long, the EOMs form one mass supplied by the oculomotor
nerve. When the embryo is 8–12 mm long, this mass divides into
separate muscles. It is at this stage that the fourth and sixth nerves
arrive. Due to disturbing influences of unknown origin, the abducens
nerve fails to develop, causing branches of the oculomotor nerve to
remain in contact with the muscle mass that would later become
the lateral rectus [4]. Pfaffenbach et al. showed that sporadic forms
of DRS are at 10 to 20 times greater risk of having other congenital
malformations divided into mainly four categories: skeletal, auricular,
ocular, and neural [5].
Skeletal abnormalities include cleft palate, limb deformities,
phocomelia, vertebral anomalies, and spina bifida. Auricular
abnormalities include preauricular tags, pinna defects, and
sensorineural deafness. Neural defects involve the third, fourth, and
sixth cranial nerves.
Wildervanck syndrome, also known as cervico-oculo-acoustic
syndrome, constitutes a triad of Klippel–Feil anomaly (fusion of >1
cervical vertebra), Duane retraction syndrome, and hearing deficits
with a ten-fold female to male preponderance [6]. The Online
Mendelian Inheritance in Man (OMIM) database has estimated the
prevalence to be <1/1,000. A Medline search revealed that till date,
only 45 cases of Wildervanck syndrome with a complete triad have
been described .The interesting fact is that our patient presented with
additional clinical signs apart from the complete triad described by
Wildervanck.
Conclusion
Duane retraction syndrome may associated systemic defects
like Wildervanck syndrome. So it becomes imperative to perform
a thorough systemic examination to rule out other associated
congenital anomalies. our case is a probable Wildervanck syndrome
with crocodile tears which was very rarely reported in medical
literature.
References
Citation
Ravichandran R, Lenin Shankar P, Ravi Kumar V. A Rare Case of Bilateral Duane’s Retraction Syndrome with Crocodile Tears, Hearing Loss and Klippel Feil Syndrome (Wildervanck Syndrome). Indian J Neurol. 2023;4(1): 115.