Case Report
Migraine Headache with Formed Visual Hallucinations: A Rare Case Presentation
Sharma M1*, Kushwaha S2 and Aravind G2
1Department of Psychiatry, Lady Hardinge Medical College, New Delhi, India
2Department of Neurology, Institute of Human Behavior and Allied Sciences, Delhi, India
*Corresponding author: Sharma M, Department of Psychiatry, Lady Hardinge Medical College, New Delhi, India E-mail:
mini271191@gmail.com
Article Information: Submission: 08/09/2021; Accepted: 21/01/2022; Published: 24/01/2022
Copyright: © 2022 Sharma M, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Abstract
Migraine headache is not an uncommon presentation in general population. It’s one among the leading 10 causes of disability and causes significant
impairment in daily functioning as well as socio-occupation functioning. Despite being significantly high in prevalence rates and having a negative impact on
quality of life it continues to be underdiagnosed and undertreated. Around a third of population present with aura that may include ill-formed hallucinations
or zigzag lines, crescent and non-linear patterns that are rarely fully formed. We report a rare presentation of a patient will formed visual hallucination which
was difficult to diagnose due to various neuropsychiatric differentials. After extensive evaluation and neuro-imaging to rule out other medical, neurological
and psychiatric causes patient was started with management for migraine on which a good response was seen. Formed visual hallucinations are rare
presentation in classic migraine but more complex hallucinations can occur in migraine coma and familial hemiplegic migraine.
Introduction
Headache disorders are the most common disorders of the
nervous system. Among these painful and disabling disorders
common cause of primary headache are-migraine, tension-type
headache, and cluster headache. Chronic headache disorder affects
coping of an individual that predisposes the individual to other
illnesses like anxiety, depression and insomnias. Headache disorders
also causes suffering, impairment of quality of life and adds to the
financial burden on society [12].
Migraine is a debilitating neurological condition that presents
with moderate to severe unilateral and throbbing, often associated
with sound sensitivity, light sensitivity, nausea, and vomiting [13].
Migraine headache is a common presentation in clinical practice
having a prevalence of 15% - 29% in the general population [1].
Approximately 90% of people in the US experience headache during
their lifetime. Migraine is the second leading cause of years lived with
disability worldwide [11]. It is seen that, migraine and severe headache disproportionately affects women, with the overall prevalence being
20.7% in females while 9.7% in males [2]. Around 31% of migraine
has an aura [3], where visual hallucinations can present as classic aura
of migraine, although these are less common manifestation while
seen in migraine coma and familial hemiplegic migraine [4]. The
classic visual aura mostly starts as a flickering, uncolored, unilateral
zigzag line in the centre of the visual field that gradually progresses
toward the periphery, often leaving a scotoma, that lasts less than
30 minutes (and almost always lasts less than 60 minutes) and may
have variations such as colored patterns may also occur [5]. Fully
formed visual hallucinations are a very rare presentation with classic
migraine and require a detailed neuro-psychiatric evaluation to rule
out common causes with visual hallucination like migraine coma and
familial hemiplegic migraine and psychosis.
Case Presentation
A 24 years female presented to OPD of a tertiary neuro-psychiatric institute with complaints of sudden onset severe pulsatile
unilateral headache lasting for 4-5 hours for past 3years which was
initially occurring once in a month associated with nausea and
phonophobia, partially relieved with oral analgesic medications.
There was an increased progression of severity, duration and
frequency of episodes noted over past one and a half year leading to
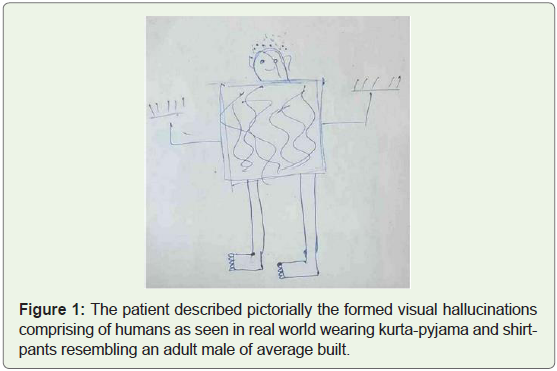
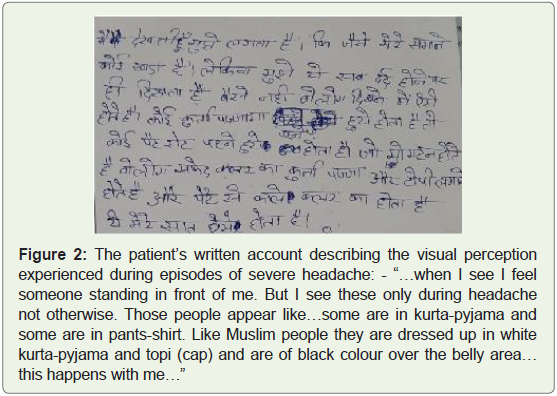
dysfunction in day-to-day activity of the patient. Over past one year,
onset of severe headache would now be associated with perception
of some strange people (usually 3 in number- 2 adults and a child)
with scary faces around the patient. They would be described by the
patient to be wearing white kurta-pyjamas like Muslim attire or shirt
and pants which would be seen vividly in her clear conscious state
not under her control and would last along with headache for around
10-12 hours and would never occur in absence of headache (
Figure 1&2). She would report about presence of strange people around
her which was considered to be part of witchcraft and patient visited
multiple faith healers for around 6-8 months but all these efforts were
futile. Considering further deterioration in her condition and daily
occurrence of these visual phenomena and severe headache over past
2 months help was sought from health facility.
Patient had no abnormality on detailed neurological examination
and normal fundus examination. Along with this, detailed psychiatric
evaluation was done on which she was found to have normal mental
status. She had normal blood parameters on investigation. EEG and
brain imaging done (MRI brain) showed normal study.
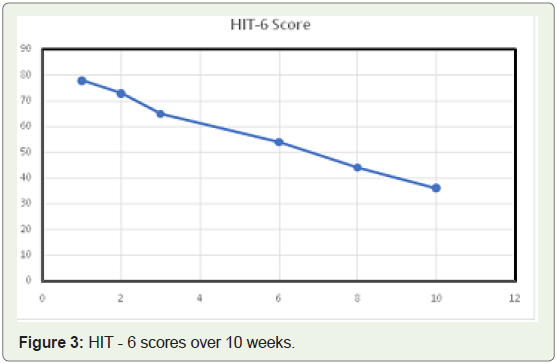
Patient was diagnosed to be a case of Classic migraine with visual
hallucinations with a score of 78 on HIT-6 (Headache Impact Test-6)
and severe disability with a score of 78 on MIDAS (Migraine Disability
Assessment) (Figure 3) (Table 1). The patient was put on Tablet
Propranolol 40mg, Tablet Flunarizine 5mg and Tablet Naproxen
500mg SOS over 3-4 weeks. On follow up she showed complete
resolution of visual hallucinations and a subjective reduction of 40%
in severe headache intensity and frequency. Subsequently the dose of
Tablet Propranolol was increased to 80 mg and Tablet Flunarizine to
10mg per day on which good response (HIT-6 score = 36) was seen
over the next 6 weeks.

Discussion
Migraine with aura in which aura consists of visual and/or sensory
and/or speech/language symptoms, but no motor weakness, and is
characterized by gradual development, duration of each symptom
no longer than one hour, a mix of positive and negative features
and complete reversibility. Migraine with typical aura in which aura
is accompanied or followed within 60 minutes by headache with or
without migraine characteristics [6].
Diagnostic Criteria:
• Attacks fulfilling criteria for Migraine with typical aura
• Headache, with or without migraine characteristics,
accompanies or follows the aura within 60 minutes.Classic migraine is known to have ill formed visual phenomena
as a part of aura and presence of formed visual hallucinations is a rare
entity. Occurrence of visual hallucination is suggestive of occipital
pathology or occipital epilepsy which can present without any motor
symptoms. However, visual symptoms in epilepsy generally last less
than 5 minutes which start usually in the periphery of one temporal
visual field while, the auras in migraine generally start more to the
centre and expand to the periphery [7]. It was ruled out in index
case by neuroimaging and neurophysiological studies. They may also indicate peri-ictal psychosis when associated with seizure and hence,
psychiatric evaluation was done in the present case.
Another differential of young stroke was also kept which was
differentiated from migraine by lack of presence of classic aura
features (colours and zig-zag lines) in stroke [8]. Similarly, prolonged
and persistent aura which could be seen in cerebral infarction was
assessed and ruled out in light of neuroimaging.
Normal fundus examination and absence of monocular
visual symptoms differentiated the case from retinal migraine [9].
Moreover, lack of any other psychotic symptoms in form of delusions,
disorganized behavior/ speech and socio-occupation decline and
non-appearance of visual hallucination in headache-free state clearly
ruled out psychosis in the index case [10].
The index case after careful assessment and extensive evaluation
was diagnosed to be a rare case of Classic migraine with aura (formed
visual hallucinations) and had shown good response to Propranolol
and Flunarizine.
References
Citation
Sharma M, Kushwaha S, Aravind G. Migraine Headache with Formed Visual Hallucinations: A Rare Case Presentation. Indian J Neurol. 2022;3(1): 106.