Case Report
An Atypical Presentation with Extraocular Muscle Atrophy in Myasthenia Gravis Delaying Diagnosis
Patra AK*, Vanlalzami K and Ahmed N
Department of Neurology, Gauhati Medical College and Hospital, Guwahati, Assam, India
*Corresponding author: Patra AK, Department of Neurology, Gauhati Medical College and Hospital, Guwahati, Assam,
India; E-mail: aniltheeuphoria23@gmail.com
Article Information: Submission: 12/11/2021; Accepted: 06/01/2022; Published: 10/01/2022
Copyright: © 2022 Patra AK, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Abstract
A 14 year female presented with 10 year history of slowly progressive asymmetric bilateral ptosis and complete bilateral external opthalmoplegia without
involving pupil or vision, 1 month history of dysphagia, nasal intonation of voice and proximal muscle weakness without diurnal variation or Fatigability. MRI
showed normal brain with atrophied extraocular muscles. RNS hinted towards decremental response. Neostigmine challenge, Serum anti-AChR antibody
was positive. There was no thymic enlargement. Usually generalization of ocular myasthenia occurs within 2-3 years of onset but in this case it took almost
10 years. Lack of significant diurnal variation may go unnoticed by patient sometimes and may mislead the physician to a very close differential diagnosis of
CPEO. In this case, so many atypical features are there like lack of significant variation of symptoms, generalization after a stable disease course of 10 years, and associated extraocular muscle atrophy.
Keywords
Myasthenia gravis; Chronic progressive external opthalmoplegia(CPEO); Anti-AChR antibody (Anti-Acetylcholine receptor antibody)
Key Messages:
Learning point from this case is that every case of opthalmpoplegia deserves to be screened for possibilities of myasthenia gravis and
extraocular muscle atrophy should not be taken be indicative of CPEO without excluding possibilities of a treatable disease like myasthenia gravis.Introduction
Ptosis and external opthalmoplegia are common initial
presentation of myasthenia gravis. In long standing slowly progressive
cases diurnal variation and Fatigability may go unnoticed if mild
which can easily mislead to chronic external opthamoplegia especially
when associated with extraocular muscle atrophy in neuro-imaging.
Extraocular muscle atrophy can be rarely present in myasthenia
gravis. Usually generalization of ocular myasthenia occurs within 2-3
years but the duration varies in different studies.
Case Report
A 14 year female presented with 10 year history of slowly progressive asymmetric bilateral ptosis. The symptoms started at
the age of 4 years. The family member noticed that she has a fix gaze
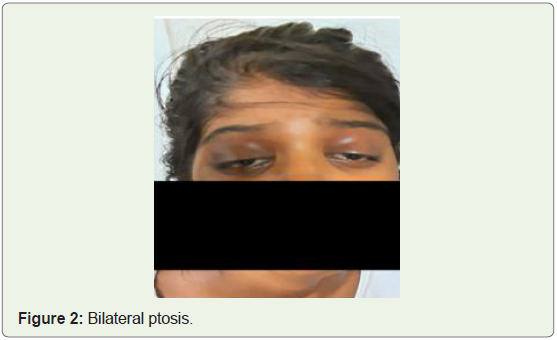
and unable to move her eyeballs. On ophthalmic examination there
was bilateral ptosis (interpalpebral fissure of 4mm on right, 3 mm
on left) with complete bilateral external opthalmoplegia without
involving pupil or vision. There was no significant history of diurnal
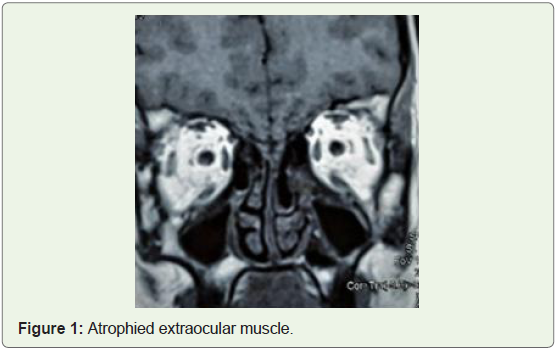
variation or Fatigability. On Suspicion of chronic progressive external
opthalmoplegia, MRI was done which showed a normal brain with
bilaterally atrophied extraocular muscles (Figure 1). Within 1 month
of initial presentation she again presented with dysphagia, nasal
intonation of voice and proximal muscle weakness. There was grade
4 power of proximal muscles, otherwise rest of motor and sensory
examinations were normal. This time we decided to do repetitive nerve stimulation which hinted towards decremental response.
Neostigmine challenge was given and ptosis as well as other symptoms
improved remarkably (Figure 2). All blood investigations including
CPK were normal. Her serum anti-acetylcholine receptor antibody
was positive (>8 nmol/l), anti-MuSK antibody negative ((0.2 U/ml).
There was no thymic enlargement in CT scan of chest. She improved
with pyridostigmine and prednisolone. Glycopyrrolate 0.5 mg twice
a day was started along with pyridostigmine 30 mg three times daily
orally with dose increase according to response. Patient was started
with 20 mg oral prednisone with 10 mg dose increase in every 2 weeks
till 1 mg/kg/day and maintained till improvement.
Discussion
Usually generalization of ocular myasthenia occurs within 2-3
years of onset but in this case it took almost 10 years [1]. Lack of
significant diurnal variation may go unnoticed by patient sometimes
and may mislead the physician to a very close differential diagnosis
of CPEO. Though extraocular muscle atrophy is uncommon finding
in myasthenia gravis, it may be misleading sometimes. In this case so
many atypical features are there like lack of significant variation of
symptoms, generalization after a stable disease course of 10 years and
associated extraocular muscle atrophy [2,3].
Conclusion
Learning point from this case is that every case of Ophthalmoplegia
deserves to be screened for possibilities of myasthenia gravis and
extraocular muscle atrophy should not be taken as an indication of
CPEO without excluding possibilities of a treatable disease like
myasthenia gravis.
References
Citation
Patra AK, Vanlalzami K, Ahmed N. An Atypical Presentation with Extraocular Muscle Atrophy in Myasthenia Gravis Delaying Diagnosis. Indian J Neurol. 2022;3(1): 105.