Case Report
Partial Visual Recovery after Delayed Surgery in a Case of Rhinogenic Optic Neuropathy: Report of a Case and Review of Literature
Sweksha Priya1, Sujata Guha1, Tanmoy Biswas1, Shamika Ghaisas1 and Md. Shahid Alam2*
1Department of Pediatric Ophthalmology and Neuroophthalmology, Aditya Birla Sankara Nethralaya, Kolkata, India
2Orbit Oculoplasty, Reconstructive & Aesthetic Services, Aditya Birla Sankara Nethralaya, Kolkata, India
*Corresponding author: Alam MS, Orbit Oculoplasty, Reconstructive & Aesthetic Services Aditya Birla Sankara Nethralaya Kolkata, India 700099, Email: mshahidalam@gmail.com
Copyright: © 2021 Priya S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Rhinogenic optic neuropathy is a clinical term used for optic neuritis or neuropathy caused by paranasal cysts or mucocele. Optic neuropathy associated
with sphenoid sinus mucocele is usually associated with poor prognosis. The prognosis in all these cases depends upon visual acuity at presentation and
duration of disease. Delay in surgery in all such cases leads to extremely poor visual outcome. We herewith report a rare case of rhinogenic optic neuropathy
that presented with complete loss of vision and had partial recovery of vision even after surgery being delayed for almost 3 weeks.
Introduction
Mucocele of sphenoid sinus is rare and constitutes 1% of all
paranasal sinus mucoceles[1,2]. It usually results from long standing
sinusitis and closure of the sinus ostia. The expanding mucocele leads
to osteoclastic absorption of the surrounding bony architecture and
pressure effect on the adjacent neurovascular structures. Presentation
of sphenoid sinus mucocele is variable depending upon the
neurovascular structures involved. The optic neuropathy developing
from these mucoceles has been termed rhinogenic optic neuropathy
and once the patient develops visual disturbances, it should be treated
as an emergency. The visual prognosis depends upon the visual acuity
at presentation, size and location mucocele, and the duration between
presentation and surgery[3-5]. Prognosis is poorer in cases where
there is profound visual impairment at the time of presentation and delay in surgery. We here with report a rare case of rhinogenic optic neuropathy who presented with unilateral no light perception vision,
was operated after 23 days from the commencement of vision loss
and showed significant improvement in vision to finger counting at
three meter at the last follow up. To the best of our knowledge there
are limited case reports of rhinogenic optic neuropathy presenting
with complete loss of vision showing partial visual recovery even
after delayed surgery. We have also discussed the optical coherence
tomography findings which have not been reported in the literature
for these cases.
Case Report
A 48 years old female presented with complains of right eye
gradually progressive painful loss of vision for the past 2 weeks. The
visual disturbance was preceded by episode of headache, nausea and vomiting. Patient had history of recurrent upper respiratory tract
infection and was a known case of diabetes mellitus, hypertension
and hypothyroidism.
On examination right eye had no perception of light while it was
20/20 in the left eye. The right eye had a relative afferent papillary defect
(RAPD) with mild temporal tenderness. Extra-ocular movements
were full. Rest of the anterior and posterior segment examination
was within normal limits. Left eye was otherwise normal. MRI of
brain and orbits showed features suggestive of large expansile cystic
lesion in the sphenoid sinus. The lesion was hyperintense on T1 and
T2 weighted sequences and exhibited rim enhancement (Figure 1A).
It was compressing over the intra-canalicular part of the right optic
nerve with abnormal contrast enhancement in this segment (Figure 1B). The findings were suggestive of sphenoid sinus mucocele with
right sided rhinohenic optic neuropathy.
The patient was immediately referred to an ENT surgeon,
however he underwent functional endoscopic sinus surgery (FESS)
and drainage of the mucocele after 8 days causing a total delay of 23
days between onset of visual loss and sugery. The patient reported
back to us after a week of surgery and the vision noted was counting
finger at one meter. Patient was given a trial of oral steroids for a
month to take care of any residual inflammation from the disease
process.
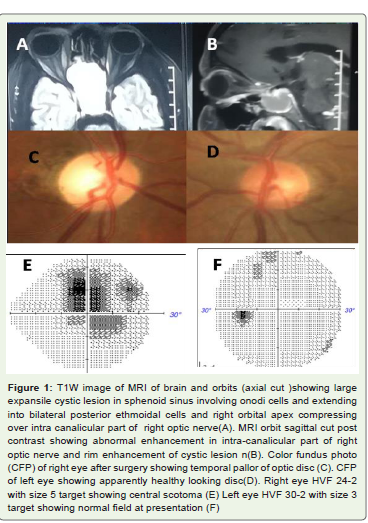
After three months the vision improved to counting fingers at
three meters. Temporal pallor of the optic disc had settled in by this
time (Figure 1C), optic disc of the other eye was however normal
(Figure 1D). The patient was able to perform perimetry with large
target which showed fixation scotoma (Figure 1E). Humphrey visual
field of the left eye was however normal both at the presentation and
at the final visit (Figure 1F).
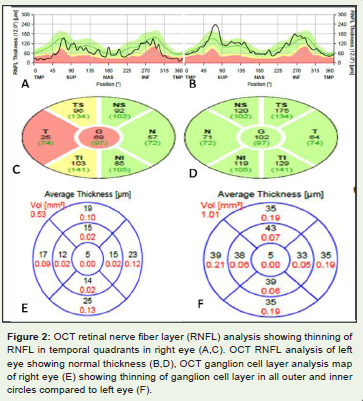
Right eye optical coherence tomography(OCT) (Spectralis OCT
platform, Heidelberg engineering, Heidelberg Germany) for analysis
of retinal nerve fiber layer (RNFL) and ganglion cell layer (GCL) was
performed at this visit which showed significant RNFL thinning in
temporal quadrants and GCL thinning in all quadrants in the right
eye as compared to left (Figure 2).
Discussion
Rhinogenic optic neuropathy is a rare differential diagnosis of optic
neuritis. Mucoceles are cystic, respiratory epithelium lined structures
which have ability to cause bone destruction within paranasal sinuses.
Sphenoidal mucocele is very rare accounting for around 1% of all
paranasal sinus mucoceles [1,2]. The spheno-ethmoidal cells are
in close relation with the sphenoid sinus, optic nerve and internal
carotid artery. Because of this close proximity, the optic nerve may
get involved in several ways. Direct spread of the sinus infection is
the most common mode; causing an infective optic neuritis (3). The
cytokines released during the infective process stimulate fibroblasts
to release prostaglandins and collagens which in turn stimulate bone
destructions causing further expansion of the mucocele. This silent
expansion of the mucocele may ultimately lead to compression of
the optic nerve [7].The released cytokines can also cause secondary
inflammatory occlusive vasculitis and optic neuritis [8].
Patients usually present with visual loss with or without motility
disturbances. Afferent pupillary defect with visual field loss is usually
seen. The classic radiological sign is appearance of large distorted
sinus with bone defect and compression of the optic nerve.
Rhinogenic optic neuropathy should always be considered as an
ophthalmic/rhinological emergency. Visual prognosis is extremely
guarded and entirely depends upon the pre-operative vision and
duration of the disease [4-6]. Prognosis is very poor in cases where
visual loss is profound (hand movement, perception of light, no
perception of light). It has been reported that visual prognosis is
poorer if surgery is delayed for more than 6-10 days after vision loss
and if optic atrophy has settled in [5]. McCarthy and Frenkel reported
diminution in final visual acuity of 64% of their study subjects with
sphenoid sinus mucocele [9]. They stated that the cause was pressure
effect on optic nerve and/or central retinal artery and no improvement
could be achieved in more than 50% of the cases, even after surgical
intervention. The role of pre or post operative steroid treatment in
cases of rhinogenic optic neuropathy is a matter of debate, however
we gave a one month course of post operative oral steroid to our
patient [4,10,11].
In the present case there was a delay of 23 days between
commencement of diminution of vision and surgery. However the
vision improved from no light perception to 20/400 at 18 months of
follow up period.
Fujimoto et al [12] in their study on optic nerve blindness due to
paranasal diseases included 7 patients with no light perception vision.
All underwent endonasal surgery within 4 days of onset of decreased
vision. Five of the 7 patients had an increase in their final vision to
20/200 or better, however 2 patients didn’t show any improvement in
vision even after early surgery.
The study done by Nakaya et al [10] included 2 patients (out
of total 38 patients) of rhinogenic optic neuropathy with no light
perception vision with surgical delay of 4 and 16 days respectively.
Both the patients failed to show any improvement.
Selvakumar and colleague [13] reported a case of rhinogenic optic
neuropathy, wherein patient had a 2 weeks history of vision loss in
both the eyes. The delay between vision loss and FESS surgery was
16 days and there was no improvement in vision in one of the eyes
even after surgery. Siritho et al [11] reported a case where the patient
was misdiagnosed as optic neuropathy and there was a delay of one
and a half month between visual loss and surgery. There was no
improvement in the vision after surgery.
Otsuka et al [4]reported a similar case as ours, where the patient
had sphenoid sinus mucocele with no perception of light. There was
no delay between visual loss and surgery and the patient’s vision
improved to 0.3 Log Mar units in the post operative period. They
concluded that preoperative visual acuity should be considered as
the most important predictive factor for postoperative visual acuity
improvement. However, an improvement in visual acuity could be
expected even in cases without light perception.
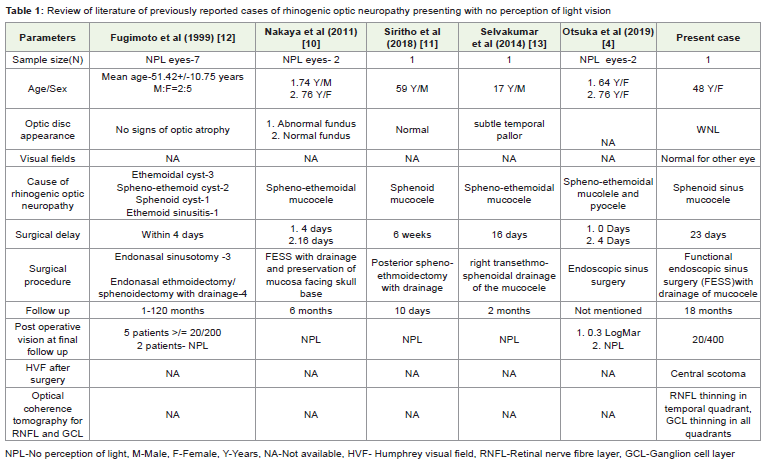
Detailed comparative review of literature has been provided in
(Table 1). To the best of our knowledge there are no reports on OCT findings
in cases of rhinogenic optic neuropathy. Though we have missed the
preoperative OCT examination, we strongly feel that preoperative
OCT RNFL and GCL analysis could predict visual prognosis after
surgery
Conclusion
Rhinogenic optic neuropathy is an important differential
diagnosis of optic neuritis. Delay in diagnosis and management can
lead to permanent vision loss. Although timely management can
prevent irreversible loss of vision and salvage useful vision to some
extent; delayed surgery too in rare circumstances can expect visual
recovery.
References
Citation
Priya S, Guha S, Biswas T, Ghaisas S, Alam MS. Partial Visual Recovery after Delayed Surgery in a Case of Rhinogenic Optic Neuropathy:
03 Report of a Case and Review of Literature. Indian J Neurol. 2021;2(1): 102