Research Article
Does Hypovitaminosis A in Mothers Cause Congenital Malformation of the Eye?
Shah S, Shah M*, Chandarana B, Rajoria R and Vador R
Drashti Netralaya, Nr. GIDC, Chakalia Road, Dahod-389151, Gujarat, India
*Corresponding author: Shah M, Drashti Netralaya, Nr. GIDC, Chakalia Road, Dahod-389151, Gujarat, India; Mobile: 00-91-2673-
238700; E-mail: omtrustdahod@gmail.com
Article Information: Submission: 10/09/2022; Accepted: 28/10/2022; Published: 04/11/2022
Copyright: © 2022 Shah S, et al. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction: Congenital malformation is an important cause of childhood blindness. Hence, we attempted to study the factors responsible for it.
Methods: This was a retrospective cohort study. We collected data from our hospital EMR for the period 2008-2019.We retrieved the total number of
paediatric outdoor and children with congenitally malformed eyes. We also explored the history of night blindness in mothers during pregnancy, exported the
data to excel sheets, and calculated the type of anomalies using descriptive analyses with SPSS 22.
Results: Our cohort included 1435 children out of the total 100946 (1.42%) outdoor of paediatric ophthalmology. We found various anomalies in our
analyses. We discerned that 423(29.47%) cases had a history of night blindness to mother during pregnancy, suggesting vitamin A deficiency.
Conclusion: Based on our clinical observation, it could be concluded that hypovitaminosis A in mother results in maldevelopment and congenital
anomalies of the eye in children.
Keywords
Vitamin A deficiency; Congenital malformation of eye; Hypovitaminosis A in mothers
Introduction
Blindness in children causes a deep impact on the psychological,
emotional, and socioeconomic growth of the family. It has been
observed that unlike adult blindness, which is 80% avoidable (either
preventable or treatable), only less than 50% of the causes are
preventable in children. The prevalence globally has been reported
to be as high as 1.5 per 1000 children in contrast to the high income
countries where the figure is only 0.3 per 1000 [1,2].
As the prevalence of blindness in children is relatively lower than
that in adults, a large sample size is required to provide accurate data
on the occurrence and causes of childhood blindness. The current rate
is known to be 0.8/1000 [3,4]. The studies from India have shown
that there has been an overall increase in congenital globe anomalies
over the past two decades, and recent investigations have asserted that
the condition contributes to nearly 40% of all causes of Childhood
blindness [1-4]. To tackle the current causes of ocular morbidity
attributed to whole globe and retinal abnormalities, a careful genetic
counseling of parents before childbirth is necessary.
In India, 3,20,000 children (<16 years) are blind, which constitutes
1/5th of the world’s blind children [4]. As reported by Dandona et al.
[3], the prevalence of blindness is 0.17% in Andhra Pradesh, which
corresponds to 6,80,000 children (after extrapolation) (Vision 20202).
The prevalence of childhood blindness was found to be 0.17%
(95% confidence interval 0.09-0.30). Treatable refractive error caused
33.3% of the blindness, followed by 16.6% resulting from preventable
causes (8.3% each due to vitamin A deficiency and amblyopia after
cataract surgery). The other major causes included congenital eye
anomalies (16.7%) and retinal degeneration (16.7%) [3].
Upon examining the etiological causes, childhood
disorders(mainly corneal infections) as a cause of blindness have
declined in the Southern part of the country but are still prevalent
in the north and northeastern parts (especially in the rural pockets)
[1,2]. Data also indicate that congenital anomalies and retinal causes
are increasing in certain regions of the country [1,2].
However, the etiology is still not known for a majority of the
causes (Khanna).
Methods
After obtaining approval from the Hospital Ethical Committee,
We retrieved data from the Electronic Medical Records pertaining to
the period 2008-2019.All children with congenital malformation were
enlisted, and all information regarding the type of anomalies, family
history, maternal history, and birth history of the child were acquired.
Specifically, details regarding night blindness in mothers during the
last trimester of pregnancy were collected. We documented the total
number of fresh outdoor cases, number of children having congenital
malformation of the eye, and mothers experiencing night blindness
during the last trimester.After obtaining approval from the Hospital Ethical Committee,
We retrieved data from the Electronic Medical Records pertaining to
the period 2008-2019.All children with congenital malformation were
enlisted, and all information regarding the type of anomalies, family
history, maternal history, and birth history of the child were acquired.
Specifically, details regarding night blindness in mothers during the
last trimester of pregnancy were collected. We documented the total
number of fresh outdoor cases, number of children having congenital
malformation of the eye, and mothers experiencing night blindness
during the last trimester.
Results
Our cohort consisted of 1435 cases. We found that 100946
children were totally examined at the Department of Paediatric
Ophthalmology, of which 1435(1.42%) children exhibited congenital
malformation of the eye. Out of the 1423 (29.47%) children having
a history of night blindness in mothers, 1330 (92.7%) were total
globe anomalies and only 105 (7.3%) constituted other anomalies.
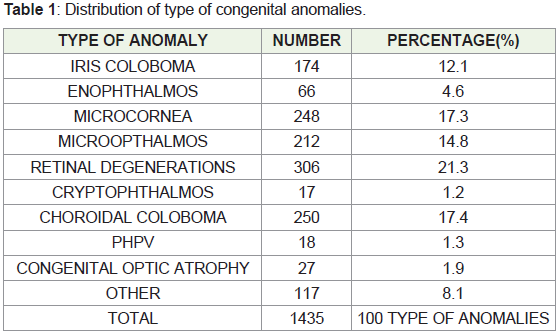
We encountered 250 (17.4%) choroidal colobomas, 174 (12.1%) iris
colobomas, 248 (17.3%) microcornea, 212 (14.8%) microphthalmos,
236 (16.4%) cryptophthalmos, 83 (5.7%) enophthalmos, and
306 (21.3%) retinal degeneration and other anomalies such
ashypertelorism, congenital optic atrophy, andpersistent hyperplastic
primary vitreous (PHPV) (Table 1).
Discussion
Congenital malformation of the eye is an important cause of
childhood blindness. We had 29.47% mothers with a history of night
blindness during pregnancy, which is suggestive of hypovitaminosis
A. Many clinical studies have covered congenital malformation of the
eye and its relationship with hypovitaminosis A. Many experimental
studies have suggested that hypovitaminosis and folic acid deficiencies
in mother leads to congenital malformations of the eye.
Mastereo-de-las et al. have reported that mice exposed to a
folic acid-deficient diet demonstrated numerous macroscopic eye
anomalies, such as anophthalmia and microphthalmia. Microscopically
too, the eye was the most affected organ (43.7% of the
fetuses)[5].
Yomai, et al. have documented that several putative genetic and environmental causes are associated with microphthalmia and
anophthalmia, including vitamin A deficiency [6].
Bhattacharrji, et al. and Millemann, et al. have stated that the major
anatomical causes of visual loss amongst 93 of the 258 patients (36.1%)
were congenital anomalies (anophthalmos andmicrophthalmos) [7].
Horne by asserted the presence of epidemiological and
laboratory evidence supporting a hypothesis of genetic (recessive)
predisposition to the teratogenic effects of mild-to-moderate
maternal vitamin A deficiency during pregnancy. This fact may
explain the high prevalence of congenital eye anomalies in certain
Asian countries where maternal deficiency of the vitamin is common
and consanguineous marriages are popular. Besides, other congenital
malformations commonly found in association with ocular coloboma
(e.g. Esophagealfistulae and heart defects in CHARGE association)
might also be related to the deficiency [8].
The results revealed that 43% of the parents were consanguineous,
19% had a positive family history, and that the frequency of coloboma
was the highest in the second-born children. Eleven (16%) mothers
had a history of night blindness while they were pregnant with the
affected child, 7 (8%) had consumed medication during the first
trimester (abortifacients in two cases), 3% had reported fever in the
first trimester, and11 (13%) had exposure to agricultural chemicals
[8].
According to Ward, et al., during embryogenesis, information
encoded in the genome is translated into cell proliferation,
morphogenesis, and early stages of differentiation. Embryonic pattern
arises from the spatial and temporal regulation and coordination of
these events. The vitamin A (retinol) derivative, retinoic acid (RA), is
essential for normal development. Mammalian embryos are protected
against vitamin A deficiency by maternal retinoid homeostasis until
the stored retinoids fall to very low levels. Retinol binding protein,
which is synthesized in the yolk sac placenta of rodent embryos and
in the syncytiotrophoblast of the human placenta, is imperative for
the embryo to access retinol. Synthesis and metabolism of RA may
involve cytoplasmic binding proteins, but the observation that
mutants lacking these proteins are normal or near-normal suggests
that they are not essential. Severe congenital vitamin A deficiency
results in a spectrum of malformations, including defects of the eyes,
lungs, cardiovascular system, and urogenital system [9].
Many other studies have also reported similar findings either in
clinical or in animal studies [10-16].
Conclusion
Hypovitaminosis in mothers during pregnancy may lead to
congenital malformation of eye.
References
Citation
Shah S, Shah M, Chandarana B, Rajoria R, Vador R. Does Hypovitaminosis A in Mothers Cause Congenital Malformation of the Eye?. Indian J Nutri. 2022;9(3): 269.