Research Article
The Effect of Positive Deviance Hearth Approach on Wasting Among Children Aged 6-24 Months in Chinkozya Community, Kazungula District, Southern Province Zambia
Chipili G1*,Chinyemba U2 and Ajayi K3
1Department of Nutritional Sciences, School of Applied Sciences and Technology, Zambia
2Catholic Relief Services, Plot 377A Ibex, Lusaka, Zambia
3Department of Human Nutrition and Dietetics, ,AfeBabalola University, Ado-Ekit, Nigeria
*Corresponding author: Chipili G, Department of Nutritional Sciences, School of Applied Sciences and Technology, Mukuba
University,Itimpi, off Chingola Road, Kitwe- 50100, Zambia; chipiligiven@yahoo.com
Article Information: Submission: 17/05/2021; Accepted: 19/06/2021; Published: 22/06/2021
Copyright: © 2021 Chipili G, et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: Malnutrition is one of the major causes of childhood morbidity and mortality in Zambia. Positive deviant hearth (PH/hearth) has been
recommended as one way of overcoming the high morbidity and mortality rates among under-five children. The current study aimed at assessing the effect
the positive deviance hearth approach (PD/Hearth) had on underweight among children in Chinkozya community of Kazungula district in Southern Province
Zambia.
Method: An intervention study was 44 children aged 6 – 24 months were admitted to the hearth for a period of 3 months. The intervention was conducted
through experimental learning. Mothers/caregivers and community volunteers met at a local point where knowledge on practices from mothers with wellnourished
children were shared with mothers with acute malnourished children. Questionnaires were administered to the head of the households of the 44
children who were admitted into the hearts and socio-demographic information was obtained. We conducted anthropometric measurements at baseline (day
1)and at the end of the three months intervention. Data analysis was conducted using STATA version 16 and WHO Anthro software version 3.2.2.
Results: The baseline prevalence of stunting was 40.9%, underweight 25% and wasting 4.5%. At the end of the intervention underweight among children
was 6.8%. PD/heath reduced underweight by 18.2% (from 25% - 6.8) in Chinkozya community. Based on the paired t-test, the mean WAZ difference reduced
by 0.27 (95%CI:-0.67, 0.13) between baseline and endline. However, this effect was not significant. (P-value = 0.1806).
Conclusion: PD/hearth reduced the prevalence of underweight in Chinkozya community, Kazungula district.
Keywords
Positive deviance; Hearth; Acute malnutrition; Children; Zambia
Introduction
Underweight is one of the major causes of morbidity and mortality
among children below the age of five [1]. In 2010, over 104 million
children in the world were underweight. Most of these children live
in sub-Saharan Africa. Globally underweight accounts for 1 million
death [2] and the prevalence of underweight in sub-Saharan Africa is
38%.1 Under-nutrition
Apart from causing morbidity and mortality in children,
malnutrition which manifests itself as underweight, stunting, and
wasting can also affect physical growth and motor development,
lower intellectual quotient (IQ), lack of social skills which may have
an impact in adulthood [3].
In Zambia, the most recent data shows that among children
less than five years of age, 35% are stunted, 12% are underweight and 4% are wasted [4]. Literature shows that community-based
interventions to combat malnutrition have shown a reduction in
severe malnourished children in Zambia from 51% in 2009 to 35% in
2013 [5]. The Zambian government and its partners have used among
many other interventions the PD/hearth approach to reduce the
levels of underweight in the country.
Positive Deviance (PD) is a strength-based or asset-based
approach based on the belief that in every community there are
certain individuals (“Positive Deviants”) who’s special, or uncommon
practices and behaviours enable them to find better ways to prevent
malnutrition than their neighbours who share the same resources and
face the same risk [6-8]. The positive deviance intervention is designed
to contribute to the reduction of the high levels of malnutrition by
rehabilitating the malnourished children, affordably and sustainably
in a culturally acceptable manner, enabling families to sustain the
rehabilitation of these children at home on their own and prevent
malnutrition among the community’s other children, current and
future [9].
The Positive Deviance approach has been in literature since 1967
with the aim of fighting malnutrition, although field research has
been recent [10]. Most African and Asian countries have adopted the
PD/hearth approach to help reduce malnutrition [9] In Malawi, study
that used the PD/hearth approach to examined the impacts of training
on nutrition, hygiene and food safety designed by the Nutrition
Working Group, Child Survival Collaborations and Resources Group
(CORE) showed a progressive effects in ameliorating children’s
under nutrition and improve dietary and hygiene practice among
mothers [11]. A Kenyan study also found an improvement in weight
gain among children who were followed up for six months after
graduating from the hearth in Migori County [12]. The study further
found that feeding frequency was the main contribution to weight
gain compared to other care practices [12].
Underweight is caused by so many factors. The main cause of
underweight is inadequate dietary intake [13].Other factors include
diseases that may be cause by food insecurity in the household,
poor maternal and child care practices, poor sanitation, and living
environment and no access to basic health services [13]. These
factors can be attained easily if the community is involved in the
implementation of the intervention. The current study used positive
deviance hearth approach because of its developmental approach to
the community already exists within the community. This approach
differs from traditional “community need based” approaches in that
it does not focus primarily on Identification of needs and the external
inputs necessary to meet these needs [10]. PD/heath seeks to Identify
and optimize existing and available resources and solutions within
the community to solve community nutrition underweight among
children. The primary objective of this study was to assess the effect of
the PD/hearth approach [7]. In the reduction of underweight among
under-five children aged 6-24 months.
Materials and Methods
Study area:
We conducted an intervention study using the PD/hearth
approach at Chinkozya rural community health post of Kazungula district in Southern Province, Zambia. Chinkozya community is
located 35km from the Simango Health Centre under which it
operates. The Simango Rural Health Centre is located in Kazangula
District, approximately 60km from Livingstone the tourist capital of
Zambia. Based on the nutrition assessment conducted for the whole
catchment areas prior to the study, Chinkozya has one of the highest
rates of under-five children disease presentation of all the villages in
the catchment area, due to its high population.Study population:
The study population included children aged 6-24 months who
were enrolled into the PD hearth in Chinkozya community.Measurements
Socio demographic information:
Socio-demographic information was collected from the mother
of infants at baseline (day 1). The data collected included the age and
sex of the head of house, marital status, level of education, occupation.PD/hearth intervention:
We implemented PD/heath approach using community
volunteers. We used practices of mothers with well-nourished children
to transfer them to mothers with underweight (acute malnourished)
children. The practices included feeding practices with the emphasis
on introducing solid foods at 6 months and feeding children with
complementary foods three times a day. Water and sanitation in
which mothers were told to draw water from a protected water source
such as a borehole, treating water either by boiling or using chlorine
and washing of hands before and after handling food and after using
the toilet or following changing the child’s nappy. Hygiene regarding
bathing the child and cleaning cooking utensils after use, cleaning,
caring, and health seeking behaviour were emphasized.These were done through experimental learning which included
cooking demonstration of some foods and feeding of children with the
same foods. The PD/hear approach was also localised by participants
who called it “chiko” meaning a cooking place or fireplace. Care givers
and community volunteers met at a local point where knowledge on
practices from mothers with well-nourished children was shared with
mothers with acute malnourished children.
Anthropometric measurements:
Weight of children in the intervention was taken on day 1, 12, 30
and 3 months after the start of the hearth to assess their nutritional
status. The purpose of taking weight 12 days after enrollment was
to monitor children who were not gaining weight so that they can
be referred to the rural health centre for further medical attention.
Height of infant was taken at baseline only. However, for the purpose
of this study only weight and height taken on day one (baseline) and
weight taken at three months endpoint will be reported.Length/Height Board of the United Nations Children’s Funds
(UNICEF) were used by community volunteers who underwent
training on how to conduct height and weight measurements.
The reading from the height boards were recorded to the nearest
centimetre. Portable (Seca Model 881) scales were used for measuring
weight of children dressed in light clothing. The scales were checked for accuracy and calibrated using standard known weights before
use. Weights were recorded to the nearest 0.1 kg. Children who
could not stand on the scale were weighed with the respondent,
then the respondent was weighed alone, and the difference was
used for obtaining weight of the child. The children were dressed
in light clothing and the scales were calibrated to zero each day of
measurement to avoid measurement errors. The reading of the child’s
weight was recorded to the nearest 0.1kg.
Statistical analysis:
We used world health organisation (WHO) reference medians to
calculate anthropometric indices. Weight-for-height s-score (WHZ).
Height -for -age (HAZ) and weight-for-age (WAZ) below negative
two (<-2) defined wasting, stunting and underweight, respectively.
WHO anthro software was used to do the nutrition status analysis
while STATA version 16 was used to compute percentages, means
and standard deviations of baseline characteristics and to determine
the mean difference between the baseline and endpoint WAZ using
paired t-test.Ethical approval:
Permission to conduct a study in Chinkozya community was
granted by the Kanzungula district office and the village head person.
Informed consent was given by the mothers/caregiver to have their
children included in the study.Results
The socio-demographic characteristics of participating children
are presented in Table 1.The number of children enrolled in the study
was 44. Of the 44, 28 (63.6%) were females while 16 (36.4%) were
males, and their age ranged from 6-24 months. The mean WAZ was
-0.89 ± 1.27, ranging from -2.71 to 1.87.The number of mothers who
enrolled their children into the hearth was 37 (84.1), while 7 (15.9)
were caregivers.
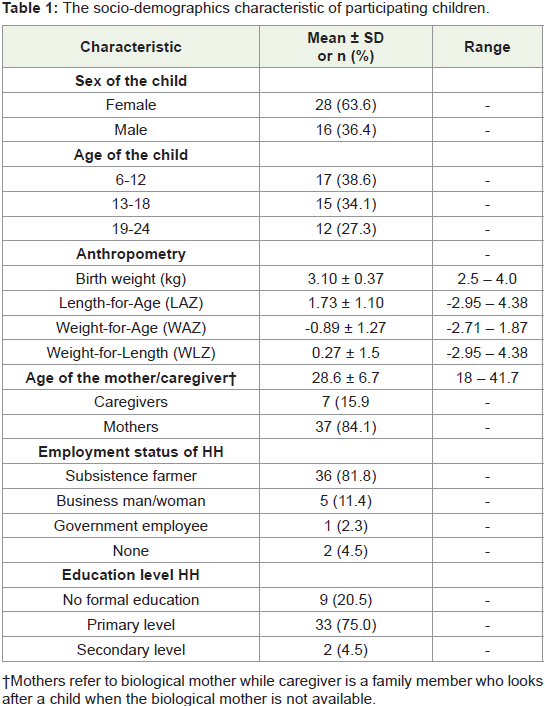
†Mothers refer to biological mother while caregiver is a family
member who looks after a child when the biological mother is not
available.
Maternal care practices of children enrolled in the hearth are
shown in Table 2. There was an improvement in all the care practices
that were assessed in the study (Table 3). Meal frequency improved
from 51.2% to 82.3%. Participation of mothers in the hearth also
improves from 76.4% to 98.1.
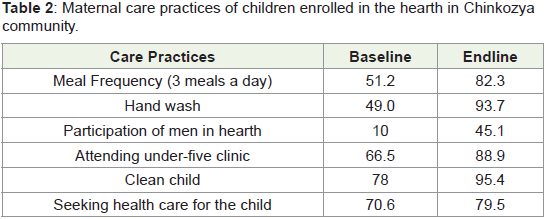
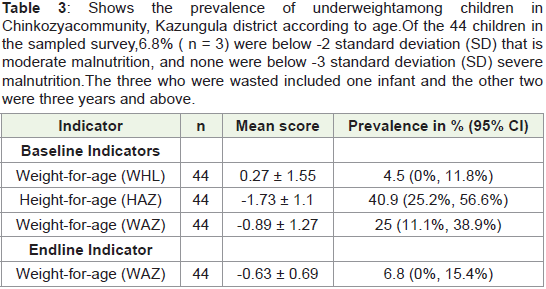
Figure 1 shows the mean difference between baseline and endline
WAZ in Chinkozya community. The median WAZ at baseline
is slightly before the -1SD while at baseline it’s above -1SD.This
indicates an improvement in WAZ between baseline and end line.
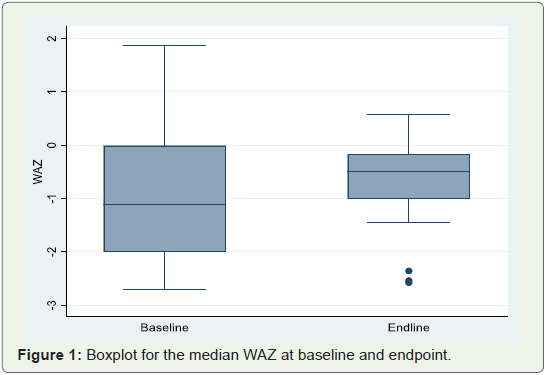
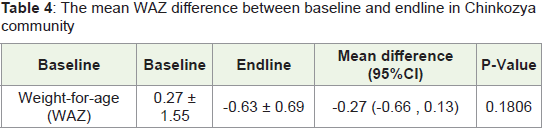
The mean WAZ difference between baseline and endline is shown
in Table 4.The mean at baseline was -0.89 and the mean at endline
was-0.63. The mean difference between the two time points was
-0.27 (95%CI:-0.67 , 0.13). However, this mean was not statistically
different P-value = 0.1806.
Discussion
The main aim of the study was to assess the effect of the PD/hearth approach in the reduction of underweight among under-five children
aged 6-36 months. In Chinkozya community. Result from the study
indicates that PD/Hearth reduced the levels of underweight by 18.2%
(from 25% - 6.8%) in the three months intervention period. The 6.8%
had a reduction from moderate underweight to mild underweight. Our
findings are similar to the a PD/hearth impact evaluation conducted
in Kenya that found a reduction in underweight from 18.9% to 3.8%
of those who were moderate underweight and from 43.4% to 34.0%
of those who were mild under nutrition [12]. The reduction in the
current study is evidenced by the successful graduations that took
place in Chinkozya community. Children gained weight of 400g and
above. Thus, changing their nutrition status from severe, moderate or
mild to normal.
However, when paired t-test was used to determine the difference
in mean WAZ between the baseline and endline, we recorded a
mean difference of -0.27 (95%CI:-0.67, 0.13), yet this mean was not
statistically different (P-value = 0.1806). Our finding differ with
what was found in similar studies that were conducted in Ecuador
and Kenya [12,14]. A community-based Positive Deviance/Hearth
infant and young child nutrition intervention that was conducted
in Ecuador found that PD/hearth improved diet and reduced
underweight among participating children, odds ratio. 0.36; 95%
(95%CI, 0.13-0.96) [14]. In Kenya a study that determine the level to
which PD/hearth enables families to sustain rehabilitation at home
on their own and to identify the practices which influence PD/hearth
outcomes found a mean difference of 0.36, (95% CI: 0.57 to 0.14) [12].
The findings in the current study could be because our intervention
was only conducted for three months compared to the Ecuador and
Kenya studies that were conducted for six months. Secondly, our
study compared means between the baseline and endpoint and not
with the control group unlike the Ecuador and Kenyan studies that
had control groups to compare their results with.
The current study also showed an improvement in the care
practices among the mother and caregivers. Mothers increase their
care practice of meal frequency from 51.2% to 82.3%. Those who
were giving children meals twice a day increased the frequency to
three times a day. Increased meal frequency showed an improvement
in weight gain than other care practices in Kenya [12]. This is an
indication that the increased meal frequency in our study might have contributed to the weight gain experienced by children in our
study. Other care practices among mothers such as breastfeeding
more than 7 times a day, clean and clad child, mothers interest to
learn new things has shown positive correlates of child growth [15]
The improvement of cleaning the child by the mother/caregivers in
our study from 78.0% to 95.4% is similar to what was found in India
where care practices of a clean and clad children contributed to the
improved the nutrition status of children [15]. Furthermore, our study
shows that the PD/Hearth approach encouraged male involvement
in child care. There was an increase of male participation from 10%
at baseline to 49.1% at endline. Male involvement in PD/hearth has
been encouraged because it can help the mothers/caregiver to practice
good care behaviours [15].
Conclusions
The PD/heath approach reduced underweight among children
in Chinkozya community. If well implemented by the community
through involvement of men, it can help reduce levels of underweight
in rural communities
Limitation and strength of the study:
We did not have a control group to which we could compare
our findings with. However, the study has contributed to the
existing knowledge that the PD/Hearth approach has helped reduce
underweight level among infants aged 6- 36 months. The strength
of the study was that it involved men who also contributed foods
to rehabilitate the children. Their involvement was a motivation
to mothers to participate in PD/hearth meetings since men are the
decision makers in most homes in Chinkozya community.Acknowledgement
The authors would like to thank all the participants and
community volunteers from Chinkozya rural community and the
ministry of health Kazungula district.
References
Citation
Chinyemba U, Ajayi K. The Effect of Positive Deviance Hearth Approach on Wasting Among Children Aged 6-24 Months in Chinkozya Community, Kazungula District, Southern Province Zambia. Indian J Nutri. 2021;8(3): 235.