Research Article
Food Security and Food Safety during Lockdown 2.0 in East Delhi-India
Suri S1*, Choudhary SR2 and Rohatgi S3
1Department of Food Technology, Vivekananda College, University of Delhi, Delhi, India
2NSS In-charge, Vivekananda College, University of Delhi, Delhi, India
3Department of Home Science (Foods and Nutrition), University of Delhi, India
*Corresponding author: Suri S, Assistant Professor and Convenor, Research and Innovation Club, Vivekananda College (University of Delhi), Delhi, India, Email: sukhneets@yahoo.co.in
Article Information: Submission: 05/04/2021; Accepted: 08/05/2021; Published: 11/05/2021
Copyright: © 2021 Suri S, et al. This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Context: COVID 19 has brought with it the wrath of disrupted production, processing and distribution of food along with economic fall outs. This has
increased the risk of food insecurity especially among the vulnerable. Data is required at national and community level to chalk out plan of action to curb the
ill-effects of this pandemic.
Aims: To assess the impact of COVID 19 during lockdown 2.0 on the food security and safety (practices) as well as community preparedness.
Settings and Design: The e-survey was carried out during April-May 2020 with the help of volunteers from National Service Scheme by using a
questionnaire developed, designed and pre-tested for the study.
Methods and Material: Out of 746 responses, 363 were sifted and analysed on the basis of inclusion exclusion criteria.
Statistical analysis used: Spreadsheet program (Microsoft Excel) was used for quantitative analysis of data.
Results: 49.6% worried about enough food at household level and an equal number were uncertain about food availability. 53.7% had curtailed diet
diversity. 34.2% and 10.1% experienced mild and moderate food insecurity. Only 59.2% were able to maintain social distancing though 86.2% wore mask.
Mean score of WASH and food safety practices was 0.70+0.39.
Conclusions: Food insecurity was prevalent among households of East Delhi. Data indicates moderate community preparedness. Lack of awareness
and infrastructure could be reason for several respondents not being able to maintain social (physical) distancing..
Keywords: Food Security; Food Safety; lockdown; Covid-19
Key Messages: 44.3% were experiencing mild/moderate food insecurity. Mandatory precautionary measures such as washing hands and wearing mask
were being practiced by majority. Social distancing got compromised during essential activities outside home. Greater awareness generation of masses is
necessary. Hand holding of families experiencing mild/moderate food insecurity is need of the hour.
Introduction
Food security and food safety have witnessed several challenges
since the evolution of mankind. Nearly 2 billion people across the
globe still do not have access to safe, nutritious and sufficient amount
of food [1]. While the world was tirelessly working towards achieving
the sustainable development goals including the zero hunger
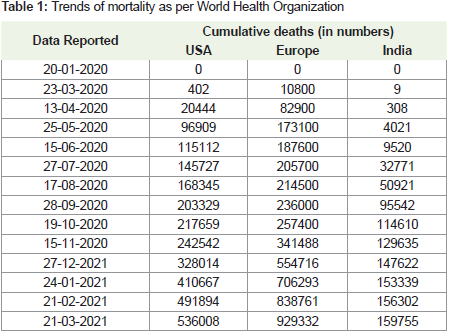
challenge it was slammed with a deadly biological hazard in the name of novel corona virus (2019-nCoV) in 2019 [2]. Data indicates that the
mortality rate in India has so far remained proportionately lower as
compared to that in other regions of the world such as United States
and Europe. Trends as per WHO situation report are summarized in
Table 1 [3-7]. It is expected that the number of people suffering from
acute hunger would nearly double to reach 265 million in the world
due to COVID 19 [8-9].
In conformity to the Disaster Management Act [10] and strategic
preparedness, the country had to go for nationwide lockdown viz.,
1.0, 2.0, 3.0 and 4.0. This decision was taken in view of the fact that
the respiratory disease spreads through saliva and nasal discharge of
active patients; nearly 78-85% of the transmission is at household
level or in clusters and nearly 80% cases are asymptomatic [11,12].
India having the second largest population, and nearly 29.4% living in
slums [13], with compromised health system, decision of nationwide
lockdown was inevitable to curb community spread [14-18].
Subsequent to the lockdown, the food system of India faced
several challenges. With a population of 1.3 billion people, Global
Hunger Index (GHI) rank of 94 and GHI score of 27.2; 190.7 million
already malnourished and 30.3% hungry [19-21]; feeding the masses
and maintaining their nutritional status was a mammoth task during
lockdown. This period coincided with the peak harvest time of
several crops such as wheat, rice, barley, fruits and vegetables. Mass
reverse migration, shortage of labour, transportation problems led to
disruption in the harvest/post-harvest/food processing activities [22].
According to the Centre for Monitoring Indian Economy [23], the
unemployment rate witnessed a sharp rise from 8.4% in mid-march to
23.5% in April 2020; being 30.9% in urban India as on 5th April 2020.
Thus, ignorance, poverty, lack of resources and large population were
a challenge to the food security and food safety of the masses [24,25].
Lockdown touched the lives of every individual physically,
socially, emotionally and spiritually. Since, the masses were unaware
of the future lockdowns, food insecurity may have trickled at
household level. Thus, an attempt was made to:
- understand the impact of lockdown on the availability,
accessibility and affordability of food
- know the psychological and social interactions of the
community with regard to food during lockdown 2.0
- know the food safety practices adopted at household level in
view of COVID-19 pandemic
- identify key areas of concern for supporting the community
Materials and Methods
Selection and Description of Participants:
a. Selection of the participants
The participants for the study were randomly enrolled through
e-platforms such as email and social media. The locus of the
diverse spectrum of respondents included families of students and
community members associated with the volunteers of the National
Service Scheme Committee of the college.
b. Eligibility criteria
Families residing in East Delhi, informed e-consent and
accessibility through phone, responses received before 14th April
2020 and after 03rd May 2020
c. Exclusion criteria
Families residing outside East Delhi, not having phone, no
informed consent.
d. Description of the source population:
Head of the family/family member managing day-to-day
household expenses/ care-giver looking after the food related needs
of the family/ adults living alone and taking care of their food needs.
Technical information:
Methods:
It was a cross-sectional study. The study was carried out in ten
steps (Figure 1).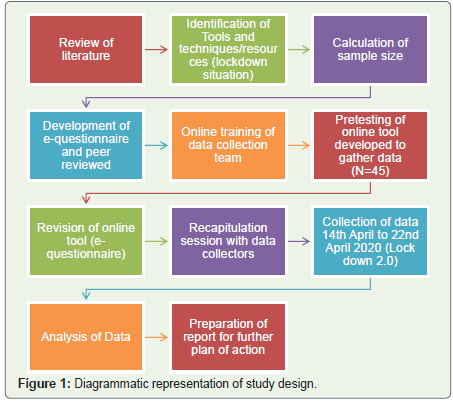
Step-1: The study was planned on the basis of extensive review
of literature. In addition to the review of literature, recent changes
in the policies and programmes especially in context to Disaster
Management Act and food supply chain at National and International
level were studied in depth. The challenges associated with biological
disasters at different levels; household/family level as well as at the
National/International levels were studied.
Step-2: The tools, techniques and availability of various resources
that could be utilized to undertake a study during lock down situation
were carefully identified.
Step-3: Sample size for pre-test and for the survey was computed.
The sample size for pre-test was 45 so as to achieve a power of 90%
for detection of errors/problems; prevalence of problem 0.05 [26].
Sample size for the survey was computed by using the Fischer’s
formula and random sampling technique, at 90% confidence level. A
minimum of 271 responses were required to be obtained.
Step 4: A structured questionnaire was developed and designed.
The questionnaire was divided into three parts. The first part aimed
to gather information on the socio-demographic profile, the second
part on the food security issues (availability, accessibility, eating
pattern, psychological and economic aspects) and the third part
was related to the food safety practices adopted at household level.
The questionnaire was subjected to peer-review and converted to a
suitable dynamic e-form that could be easily circulated and used by
respondents to enter the responses.
Step 5: The data collection team was formed and trained. It
comprised of ten students; three from the Research and Innovation
Club and seven from the NSS team of college belonging to various
disciplines of study such as foods and nutrition, political science,
history, sanskrit. Three students had also successfully completed the
course “COVID 19: Operational Planning Guidelines and COVID-19
Partners Platform to Support Country Preparedness and Response”.
They were provided online training to assist them to collect data over
non-android phones from subjects not having access to android
phone and circulation of forms over social media platforms.
Step 6: Based on the results of the pre-test (64), minor changes
were made in the online form developed and designed to gather data.
It was subjected to peer-review once again.
Step 7: Online recapitulation session was organized with the
data collection team. The finalized online form (questionnaire) was
discussed in detail. Hand-holding was done by investigators of the
study.
Step 8: The online or dynamic e-form link was circulated by email
and social media platforms. Data/responses were collected during the
period when lockdown 2.0 was imposed in Delhi. Case studies were
also noted by NSS volunteers in case of some respondents who were
contacted telephonically (non-android phone users).
Step 9: Data were automatically entered in excel sheet. The data
were suitable analysed.
Step 10: The analysed data and case studies were used for preparing
the research paper and would be used for academic purposes during
teaching the students.
Results
A total of 746 responses were recorded during this online survey.
On the basis of pin-codes and name of colony as provided by the
Postal Department of India the responses obtained from East Delhi
were sieved for further analysis. Thus, a total of 363 responses were
received from East Delhi. 10% of the recorded responses (selected
randomly) were verified to ensure authenticity of the data.
Part I: Socio demographic profile:
The modified Kuppuswamy classification of socio economic
status based on three parameters of education, occupation and total
monthly per capita family income was used to compute the socioeconomic
score [27]. 1/3rd (33.1%) of the respondents belonged to
low economic status (32.0% upper lower group and 1.1% lower) while
25.1% were from lower middle, 30.6% from upper middle class and
11.3% belonged to upper class. Majority (44.9%) of households were
having family size of 4-6 members. 33.1%households had less than
four family members while 22.0% had large families (more than 6
members). 17.6% of the households had pets/ live stocks.Part II: Anxiety towards the lockdown 2.0:
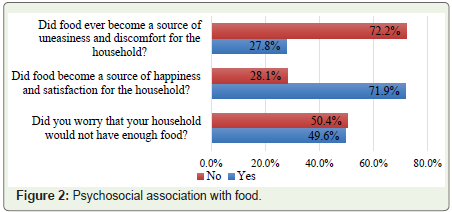
About 49.6% of participants were worried about not having
enough food during the lockdown 2.0 period.Figure 2 indicates the psychosocial/emotional association of
respondents with food. Since food is a primary necessity for life and also
due to social distancing, limited transportation/communications and
work from home, food became the pivotal point of several emotions
during the lockdown period. According to 27.8% respondents, food
became a source of uneasiness and discomfort. A few telephonic
conversations indicated that the primary reason of discomfort was
lack of availability of resources; monetary or food itself. Food was
used by 71.9% households to enjoy, relax and share happy moments
with each other during the stressful period of pandemic.
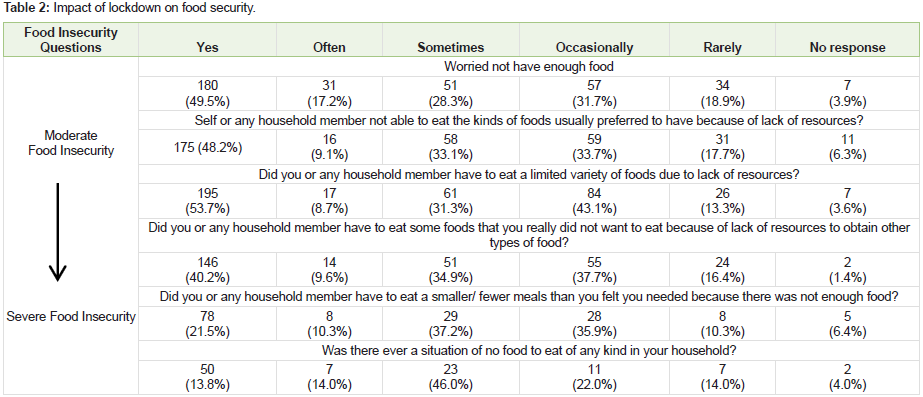
Part III: Food Insecurity: The survey tried to assess the constraints (if any) experienced by
individuals/households in having access to adequate amount of food.
The data are given in Table 2. 49.5% of the respondents were uncertain
about the availability of food for themselves and their families due to
the lockdown. Dietary diversity got curtailed in 53.7% cases as there
was reduced variety of foods at their disposal. Food choices changed
as 40.2%respondents reported to have consumed foods usually not
liked/preferred by them. Such modifications in food consumption
pattern can contribute to emotional changes/stress related behaviour
and also alter the amount of food consumed thereby resulting in
changes in the nutritional status.21.5% respondents informed that
they and their family members ate fewer or smaller meals due to
non-availability of food while 13.8% of the households reported
that there were situations when there was no food to eat. Thus, these
families were suffering from severe food insecurity. Thus, based on
the classification of food insecurity given by FAO/WHO, 70.7% (257)
households were experiencing moderate food insecurity while 13.8% (50) were suffering from severe food insecurity. Nearly 84.0% of the
households experiencing severe food insecurity had more than four
family members. 62% (31/50) of the households suffering from severe
food insecurity belonged to lower/upper-lower income group.
We further analysed the data of respondents suffering from
moderate food insecurity. Since several respondents answered ‘yes’
for more than one question related to non-availability/accessibility
of food we gave a score of “1” for each “Yes” for first six questions/
parameters mentioned in Table 2. The analysis indicated that 17.1% of
the respondents scored only ‘one out of six’ score and an equal number
received score of ‘two out of six’. Such families can be considered
to be suffering from mild food insecurity. Nearly 10.1% of the
respondents suffering from moderate food insecurity received score
of ‘six out of six’. Among the respondents suffering from moderate
food insecurity, 38.6% belonged to lower/upper lower income group.
These households could be at a high risk of experiencing severe food
insecurity in future if the lockdown/ pandemic continues for a longer
period. Details of the score are given in Table 3.

Food is primarily cooked by using piped natural gas or liquefied
petroleum gas in India especially Delhi (India being the second largest
consumer of LPG in the world). LPG (in cylinders) is used by majority
of lower income households [28]. It was therefore important to know
whether the supply of fuel for cooking food got affected during the
lock down. Data of our survey indicated that majority; 90.8% (327)
had access to fuel for cooking food.
Part IV Diet Diversity:
As discussed above (part III) 53.7% households ate limited variety
of foods during the lock down 2.0. Data were gathered regarding the
non-availability (if any) of food items (food groups) by using an open ended question. 354 responses were obtained. All foods usually
consumed in daily diets were available in 68.3% (247) households.
29.5%(107) of the respondents reported that all food items which
they usually consumed in daily diets were not currently available in
their households. Majority (57.0%, 61) of these households belonged
to lower income group. These 107 responses were further analysed
by using the eight food group classification. The results indicated
that staple cereals which are the primary source of energy in Indian
diets were missing in 30.8% (33) households of which 30.3% (10)
and 66.6% (22) belonged to households experiencing severe and
moderate food insecurity respectively. Pulses were not available in
27.1% (29) households of which 41.3% (12)and 55.1% (16) belonged
to households experiencing severe and moderate food insecurity
respectively. Fats/oils were not available in 7.5% (8) households
(Table 4).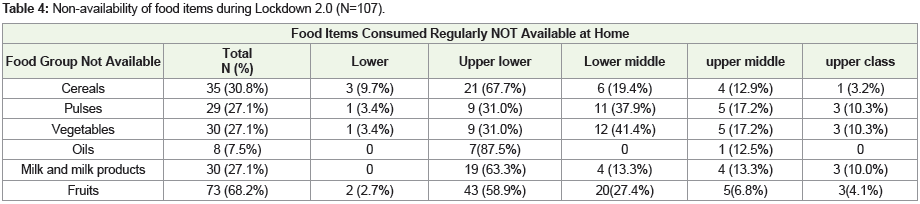
Part V: Precautionary measures - WASH Practices and Behaviour modification:
Several studies are indicating that SARS-CoV-2 RNA is found
in waste water contaminated with upper gastro intestinal and upper
respiratory system several days before the detection of COVID 19
through clinical surveillance [29]. India being a developing country
has compromised environmental and social sanitation, in resource
stricken segments of the population [30]. Compromised social and
environment sanitation by food handlers could increase the risk of
transmitting Covid-19 virus. Data were therefore gathered regarding
the precautionary measures being taken by the community regarding
WASH practices. This would help in knowing the level of community
preparedness.Data indicates that 82.6% of the participants had access to tap/
supply water as a source of drinking water and 76.6% of the participants
were purifying the water. As a precautionary measure, 15.7% of the
participants had modified (improved) the method of purifying water
and 7.7% reported that the source of water had been changed.78.2%
of participants used tap/ supply water to wash vegetables/ fruits as their usual practice while 15.7% used water purified by using reverse
osmosis system. Only 3% used hand pump and 3.3% did not wash
fruits and vegetables. 44.9 % of them had changed their practices
of washing vegetables/fruits during this pandemic period as result
during the lockdown 2.0, 75.2% of all was them always, 17.6% washed
them occasionally and remaining did not wash fruits and vegetables.
Data were also gathered regarding the practices adopted by the
community regarding storing of fresh/raw produce. 62.5% washed
vegetables/ fruits before storing them in refrigerator. Compromised
practice such as storing unwashed raw food was practiced by 37.5%
respondents. Data indicated that 75.2% participants always washed
cartons/ packets purchased, 17.6% washed them occasionally while
remaining participant did not wash.
Refrigerator was available in majority i.e. 91.1% households out of
which 69.7% households had cleaned it in the past 15 days. Majority
(48.3%) used soap and water for cleaning, while 20.0%, 13.5%, 4.8%
and 3.0% used some readymade solutions, disinfectant, soda and
water, sanitizers respectively. 24.2% of participants reported to have
made changes in the choice of utensils for preparation and serving.
81.3% used stainless steel utensil for preparation and eating, 10.5%
used disposables while few of them used melamine/glass.
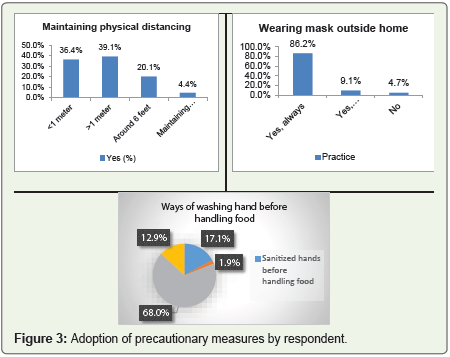
In accordance to the WHO recommendations on precautionary
measures for maintaining social distancing, 59.2% reported to have
been able to maintain social distance and 86.2% participants wore
mask while moving out from house (Figure 3). Data indicated that
22.0% wore mask while preparing and or serving food at home also.
While 97.2% participants washed hands after coming back home,
66.7% washed their foot wares also. Maximum (68%) number of the
participants washed hands with soap and water before handling food.
27.5% participants reportedly discarded the shopping bags after every
use, 28.9% kept the bag aside for few hours, 32.0% washed bags after
single/every use while remaining 11.6% had compromised practices. 82.6% made cash payments, 3.9% credit/ debit cards, 11.8% online
while only 1.7% purchased groceries on credit.
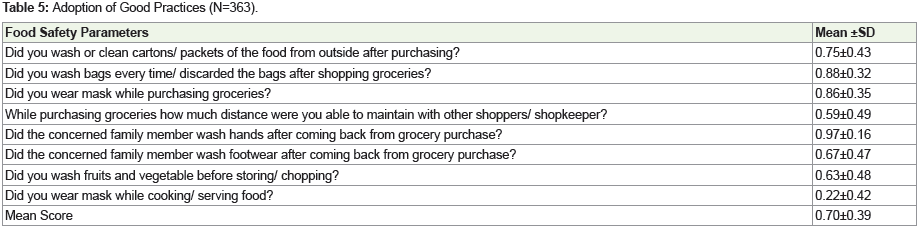
We gave a score of one for each good practice adopted by each
respondent. The results are summarized in Table 5. The mean score
indicates that community preparedness was fairly good to protect
themselves from Covid-19 virus.
Part VI: Community Support:
During natural disasters/pandemics both government and
community are stakeholders to social responsibility. Hand holding by
the community was observed during the study as nearly 49.9% of the
households reportedly provided monetary/food related support to
the resource stricken community members (Figure 4). In the lower/
upper-lower income group, 47.5% and in the upper-middle income
group, 26.3% of the respondents informed that they had received
some kind of monetary/food related support from the community/
government.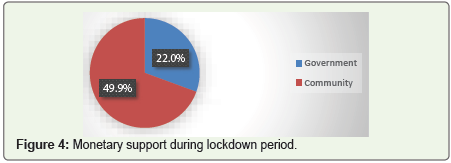
Discussion and Conclusion
India has witnessed 11,787,534 confirmed cases and 160,692
deaths as on 24th March 2021; the numbers being lowest in
December 2020 peaked in September 2020 and are once again rising
in March 2021 after a hiatus. While the country has administered
more than five crore vaccine doses, its health sector has to race
against time. According to the estimate of the United Nations World
Food programme (2020), 265 million people could face acute food
insecurity by the end of 2020; up from 135 million people before the
crisis. According to this study, the social protection programmes and
the community hand-holding have been able to face the challenges
of food insecurity which arose as an outcome of covid-19 pandemic
during the emergent and sudden lockdown. However, surveillance
on the status of food security should be done on a continuous basis
especially during the unlock phases (when the economic meltdown
would be most vivid) to avoid another pandemic, the pandemic of
under nutrition in times to come.
References
Citation
Suri S, Choudhary SR, Rohatgi S. Food Security and Food Safety during Lockdown 2.0 in East Delhi-India. Indian J Nutri. 2021;8(2): 228.