Research Article
Eating Behavior and Nutritional Status of Adolescents in Peri-Urban Delhi
Upasna Seth*
Department of Home Science, Aditi Mahavidyalaya, University of Delhi, Delhi, India
*Corresponding author: Upasna Seth, Department of Home Science, Aditi Mahavidyalaya, University of Delhi, Delhi, India; E-mail: upasnaseth01@yahoo.co.in
Article Information: Submission: 01/03/2021; Accepted: 08/04/2021; Published: 12/04/2021
Copyright: This is an open access article distributed under the Creative Commons Attribution License, which
permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background:
The nutritional and life style transition in urban as well as rural areas of countries has resulted in rapid changes in eating behavior. The
replacement of traditional home-cooked meals with ready-to-eat processed foods has contributed to malnutrition among adolescents.Objective:
The present study is with objective to investigate the eating behavior and prevalence of malnutrition among adolescents in peri-urban Delhi.Method:
This cross-sectional study was conducted with 491 children in the age group of 12 to 14 years in government peri-urban schools. The data
collection was done through administering questionnaires and conducting anthropometric measurements. It was observed that adolescents have erratic eating
behavior.Results:
The average percent adequacy intake of food groups for cereals was 63.5%, pulses 71%, vegetables 54%, fruits 60%, milk and milk products
69%, sugar 187% and visible fat/oils 196%. The average percent adequacy intake of nutrient for energy was 87%, protein 74%, iron 69.5%, calcium 59% and
vitamin A 80%. The energy intake from fat was 35%, which is high. It was observed that as per BMI for age 5 to 19 years (z-scores) classification by WHO 17%
adolescents were overweight, 42% were underweight and 41% were with normal BMI. 5. Conclusion: Thus the study concluded that malnutrition is prevalent
among the adolescents and there is need to encourage healthier lifestyle habits among students through various strategies to improve dietary pattern and
nutrition status.Keywords
Adolescents; Eating behaviour; Nutritional status; Malnutrition
Introduction
The rapid changes in the structure of the Indian diet due to
globalization, proliferation of multinational fast food companies
in the Indian food market have replaced traditional home cooked
meals with ready-to-eat, processed foods. The replacement of
traditional home-cooked meals with ready-to-eat, processed foods
has contributed to an increased risk of chronic diseases. This has also
bought nutritional and life style transition in urban as well as rural
areas of countries resulting in high fat intakes, low intakes of fruits
and vegetables, increased consumption of refined foods, erratic eating
behavior coupled with low physical activity, thus placing individuals
at risk of chronic diseases such as obesity, diabetes, hyper tension,
cardio vascular disease, osteoporosis, etc towards development of
disease in adulthood [1].
Adolescence is one of the most dynamic and complex transitions in the life span, representing a transitional period between childhood
and adulthood. During adolescence there is rapid enlargement of
organs and tissues which needs to be supported by nutrients. Under
nutrition in adolescents may lead to slowed growth rates and have
lasting consequences on an adolescent’s cognitive development.
Macronutrient deficiencies may have negative impact on bone
mineralization [2]. Over nutrition puts an adolescent at risk of
coronary heart diseases as they grow up [3] Adolescence is a crucial
period in a woman’s life. Health and nutritional status during this
phase is critical for the physical maturity, which in turn influences
the health of the offspring. The physical developmental and social
and emotional changes to occur during adolescence this bring
changes in lifestyle and formation of new eating behaviors which
are continued into adulthood. Thus good nutrition and dietary
behavior are important to achieve full growth potential, appropriate
body composition and to promote overall health and well-being [4]. Research on trends in food consumption and nutritional status
also show that serious concerns over childhood and adolescence
malnutrition.
The expansion of large cities has meant increasing and more
complex interactions with surrounding rural areas, transforming
them into peri-urban areas. Thus peri-urban is an area immediately
adjacent to a city or urban area. They are characterized by dynamic
flows of commodities, capital, natural resources, people and pollution
and a range of processes leading to the intensification of urban-rural
linkages [5]. In India, peri-urban areas are too often neglected. They
are fraught with institutional ambiguity, unplanned growth, poor
infrastructure and environmental degradation. In India, 57 per cent
of the urban population lives in the expanding city peripheries, thus
policy and planning must support rural-urban transformations
in relation to changes in food production, access, consumption,
nutritional quality and safety [6]. To improve health and nutrition, a
more holistic, food security-based perspective is needed in peri-urban
agriculture while protecting the environmental services on which
they depend. To date, little is known about the food intakes of Indian
adolescents. Neither the National Family Health Survey-3, 2007 nor
the National Sample Survey Office, 2012 have examined the dietary
habits of urban Indian adolescents [7,8]. This lack of evidence about
the food consumption patterns of Indian adolescents is a significant
barrier to the development of effective nutrition promotion and
disease prevention measures. Therefore, the present study was
undertaken to examine the dietary intake and nutritional status of
school going adolescents in peri-urban Delhi. The area under study
has observed a shift from agriculture to industrilization and is likely to
result in under nutrition amongst adolescents. Mostly interventions
to curb malnutrition are targeting children and mothers leaving out
adolescents, whereas the adolescents may be vulnerable.
Methodology
The present study with early adolescents was conducted in the
year 2015 in a peri-urban schools situated in North West Delhi. This
cross-sectional study was conducted with 491 children in the age
group of 12 to 14 years in 7 Delhi government peri-urban schools.
To conduct the study permission was obtained from Directorate of
Education. Principals of these schools were contacted and necessary
permission to collect the information was obtained. Due to the
limitations of the sample size, the principal of the respective schools
were asked to assign one section from either VII or VIII class for the
study. Written informed consent from the teachers of the respective
class and assent from children to participate in the study was taken.
Data from school children was collected during regular class period
of 40 minutes. Information was collected regarding the eating habits
and nutrition status of early adolescents.
Dietary intake in terms of food groups, calorie, protein, vitamin
A, iron, and calcium were assessed using 24 hours dietary recall for
three consecutive days including one weekend day. A sub sample of
50 students was done to calculated nutrients and food group’s intake
using standardized recipes in Meal Planner software designed by the
researcher [9]. The interactive menu planner is designed to guide
daily food and meal choices based on one day’s calorie allowance. The mean percent adequacy of different food groups for 12 to 14 years
old adolescent boys and girls were compared with the corresponding
Recommended Dietary Allowances (RDAs) recommended by the
Indian Council of Medical Research [10]
Nutritional status of the adolescents was assessed through body
mass index (BMI), according to the World Health Organization
(WHO) Asian criteria [11]. The measurement of height and body
weight of each student was recorded by following the standard
techniques and body mass index calculated. The subjects were
classified as underweight or overweight by the following classification.
< 5th percentile- Underweight ; 5th - 85th percentile- Normal
>85th percentile- Overweight ; > 95th percentile- Obese
The responses obtained from questionnaire were suitably coded
converted into means, frequency charts, mean percent adequacy
intakes of various food groups and nutrients were assessed.
Results and Discussion
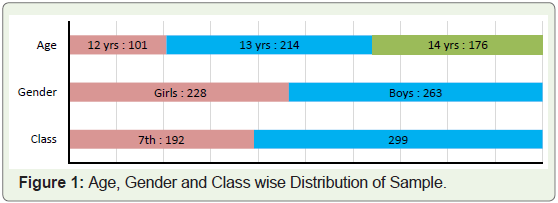
The study was undertaken at seven government schools in periurban
Delhi from early adolescents. The sample comprised of 491
students aged between 12-14 years from seven government schools
in peri-urban Delhi. The sample comprised of 101 (20.6%) 12 years,
214 (43.6%) 13 years and 176 (35.8%) 14 years old adolescents. Out
of total sample of 491 students 228 (49%) were girls and 263 (51%)
were boys. 192 (39.1%) students were from class VII and 299 (60.9%)
students were from class VIII. Figure 1 depicts the age, gender and
class wise distribution of the sample.
Eating Behaviour of Early Adolescents:
Data collected from 491 peri-urban government school students
of 12-14 years old revealed that 251 subjects (51%) were vegetarians,
94 subjects (19%) were vegetarians and 146 (30%) non-vegetarian
(Figure 2). Most of the adolescents 85% were regularly snacking and
their favorite snacks were chips, biscuits and kurkure. Almost all
children liked package food. The meal pattern of the subjects varied from 2 to 4 meals per day viz mid-day meal, packed tiffin, lunch and
dinner. It was observed that 74% (n=364) of the subjects consumed 3
meals per day and 11% (n=52) reported to consume 4 meals a day and
remaining 15% (n=75) of the subjects consumed 2 meals a day, which
was undesirable. Almost all children 91% carried tiffin to school
and most common tiffin item was paranthas (layered, unleavened
flatbread, a popular Indian cuisine made with flour, salt, fat and
water) and vegetable. 47% students reported that the quality of midday
meal (MDM) received at school was good and 22% rated the meal
received as very good and 14% also rated the MDM as excellent. The
students also reported that the mid-day meal provided had variety.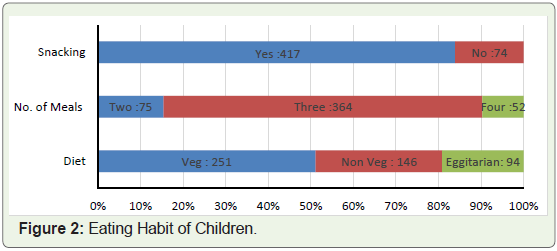
Dietary Pattern:
Food Group Intake: Food group intake was calculated using
standardized recipes in using standardized recipes in Meal Planner
software designed by the researcher (Seth 2008). The interactive menu
planner is designed to guide daily food and meal choices based on one
day’s calorie allowance. The average intake of various food groups by
50 subjects was calculated and compared to suggested intakes [10]
Mean intake of different food groups by 12-14 years old adolescent
boys and girls are reported in the following Table 1.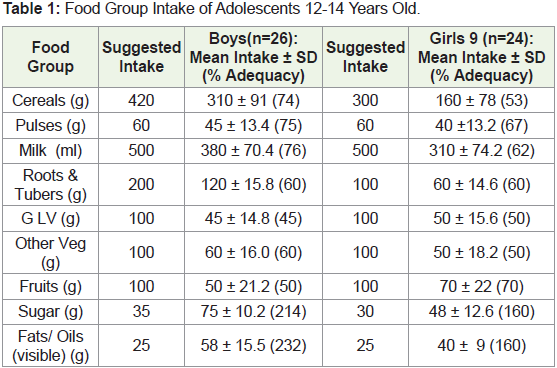
Percent adequacy of different food groups intake was also
calculated. Intake of cereals, pulses, milk and milk products,
vegetables, fruits was less than suggested intake whereas, intake of
sugar, fat/oils were very high, almost double as compared to suggested
intakes [10]. The average percent adequacy intake of food groups for
cereals was 63.5%, pulses 71%, vegetables 54%, fruits 60%, milk and
milk products 69%, sugar 187% and visible fat/oils 196%. The dietary
pattern of peri-urban adolescents show that snacking calorie dense
food was high and intake of fruits and vegetables was low coupled with
erratic meal pattern. The diet of school going children was deficient in
all the food groups except fat and sugar, ultimately resulted in the low
intake of nutrients and micronutrients. Review of literature reports
that Mid Day Meal (MDM) is an important instrument for combating
class room hunger and promoting better learning. It has catered to
the nutritional needs of school children in both rural and urban areas.
MDM is effective in improving physical and psycho-social health for
disadvantaged school children in lower income and higher income
countries. It is the largest school lunch programme in the nation and
has contributed to increase in the school attendance of children [12].
Nutrient Intake: Nutrient intake was calculated using meal planner software. The average daily intake of selected nutrients:
energy, protein, carbohydrates, total fat, iron, calcium, vitamin A was
calculated and compared with Recommended Dietary Allowances
RDA [13]. Nutrient adequacy is the level of intake of an essential
nutrient in relation to the nutrient requirement for adequate health,
which is expressed as the percentage of recommended dietary
allowance. Percent adequacy of different nutrient for 12-14 years old
adolescent boys and girls was also calculated. Table 2 represents mean
and percent adequacy intake of various nutrients by 12-14 years old
adolescents boys and girls respectively.
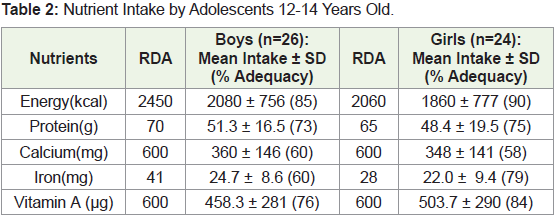
The average percent adequacy intake of nutrient for energy was
87%, protein 74%, iron 69.5%, calcium 59% and vitamin A 80%.
The average percent energy intake from fat is 35%, which is high as
compared to ADA guidelines [14]. According to Gopalan, 1988 total
fat intake can be limited to levels at which fat will provide no more
than 20% of the total energy [15]. Malnutrition is a state of nutrition
in which there is an imbalance of energy, protein, and other nutrients,
it can be both over and under nutrition and has adverse physiological
and clinical effects. It is a serious public-health problem that has been
linked to a substantial increase in the risk of mortality and morbidity.
Malnutrition is poor nutritional status due to dietary intake either
above or below the recommended daily allowances.
Anthropometry Assessment:
The height, weight and BMI of the sample were assessed. Body
mass index is a means of expressing healthy body weight. It is
computed by dividing the body weight in kilograms by the square of
the height in meters. BMI= Weight in Kg / (Height in m)2The ideal ranges of weight for a given height are provided
by WHO, which is useful for categorizing persons as normal,
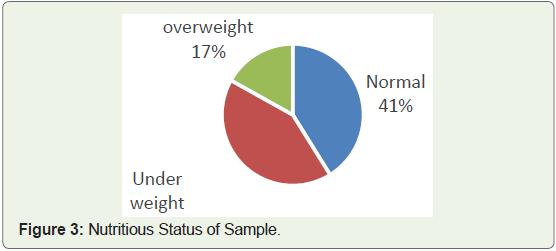
undernourished and overweight or obese. It was observed that as
per BMI for age 5 to 19 years (z-scores) classification by 2007 WHO
Reference, 17% (n=84) adolescents were overweight and 42% (n=206)
adolescents were underweight and 41% (n=201) adolescents were
with normal BMI (Figure 3). The data reveals that malnutrition both under nutrition and over nutrition is as a priority problem in perurban
adolescents and should not be overlooked. A study conducted
by Seth, 2008 with urban public school adolescents also observed 7%
adolescents were overweight and 48% adolescents were underweight
and 45% adolescents were with normal BMI [9]. Gupta and Ahmed
(1990) reported prevalence of obesity as 7.5% in school children [16].
A study conducted by Kapil et al (2002) reported that prevalence of
obesity in school children from a single school of Delhi as 8% for
boys and 6% for girls [17]. Khadilkar and Khadilkar (2004) from
Pune reported 19.9% overweight and 5.75% obesity in boys aged 10-
15 years [18]. Data thus reveals that under nourishment is prevalent
in urban as well as rural families.
Conclusion
Thus it can be concluded that there is need of lifestyle programs
in peri-urban school children to increase the nutrition knowledge,
awareness and assist in one’s behavioural change. Lifestyle programs
can be multi-factorial interventions that are designed for individuals
or groups according to the needs of the subjects to promote healthy
lifestyle habits. The review suggests that effective nutrition intervention
and education strategies based on behavior therapy are needed for
promoting adoption of healthful eating and physically active lifestyle
in adolescents. It is also concluded that schools can prove to be the
good venues to encourage healthier lifestyle habits among students
through various strategies and improve dietary pattern and nutrition
status of adolescents for healthy citizens of a nation.
Acknowledgements
The author would like to thank all the adolescents, teachers and
school principals who took part in the study.
References
Citation
Seth U. Eating Behavior and Nutritional Status of Adolescents in Peri-Urban Delhi. Indian J Nutri. 2021;8(1): 225.