Research Article
India Lockdown: Relationship between Disordered Eating and Mental Health Concerns
Bhatia IN*, Kishnani R2*
1The Nutrition Project, India
2Mind Heal(th), India
*Address for Correspondence: Bhatia IN, The Nutrition Project, 7, Embassy Center, Ground Floor, Nariman Point, Mumbai - 400 021,
India Tel:+918657991198; E-mail: ishitaa.bhatia@gmail.com
Article Information: Submission: 18/02/2021;
Accepted: 10/03/2021;
Published: 13/03/2021
Copyright: © 2021 Bhatia IN, et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
The purpose of the study was to investigate whether there was a significant positive correlation between disordered eating behaviours and mental health
concerns (depression, anxiety and stress).
A master survey was electronically circulated to young males and females (age 15-30 years) residing in the city of Mumbai, India during the national
lockdown in the month of May 2020. The survey included the DASS-21 questionnaire (depression, anxiety and stress score) and the EDE-Q (Eating Disorder
Examination Questionnaire). Subscale and global scores were processed. One-tailed Pearson’s correlation was conducted to investigate the relation between
EDE-Q global score and DASS-21 subscale scores. One hundred and eighteen (n=118) respondents took the survey. The mean scores for the depression,
anxiety and stress subscales were 15.25 (moderate), 9.94 (moderate) and 16.28 (mild) respectively. Out of the four EDE-Q subscales, the mean score of
shape concern appeared to be the highest (2.39 ± 1.6), followed by weight concern (1.96 ± 1.59), restriction (1.31 ± 1.37) and eating concerns (0.92 ± 1.19).
The mean global EDE-Q score was 1.65 ± 1.22. A positive correlation was found between EDE-Q global scores and DASS-21 subscale scores i.e. depression
(r=0.49; p<0.01) anxiety (r=0.31; p<0.01) and stress (r=0.41; p<0.01). The present study gives insight into mental health conditions and eating behaviours
present within an Indian sample during the national lockdown. It opens avenues for discussion for the need of multidisciplinary healthcare teams to provide
holistic eating disorder care.
Keywords
Survey; Depression; Anxiety; Stress; Disordered eating; Lockdown; Correlation; Eating behaviour; Mental health; Pandemic
Introduction
The widespread COVID-19 outbreak in December of 2019
in China identified that the Chinese public was at a high risk of
displaying a myriad of psychological distress and mental health issues.
The overall prevalence of mental health conditions - Generalized
Anxiety Disorder (GAD) and depressive symptoms were significantly
high and the Chinese population indicated higher risk for poorer
sleep quality [1]. Current literature suggests that self-reported
stress, depression and anxiety symptoms are common psychological
responses to the pandemic [2]. In addition, the restricted outdoor
mobility and disruptions in daily routines have indicated changes
in eating behaviours in individuals as observed by a preliminary
health survey [3]. The changes include snacking frequency, eating
out of control frequency and hunger/satiety perception, sweet intake
frequency etc. [3].
Eating disorders are psychological disorders characterised
by abnormal or disturbed eating behaviours with or without
compensatory behaviours as diagnosed by DSM-5 [4]. Behaviours
include binge-eating, purging, laxative usage, food restrictions and
excessive exercise. Disordered eating is a condition described by
similar characteristics of a lower level of severity and frequency as
that of an eating disorder [4]. Indicators of low self-esteem such as
body shape, weight, perception and preoccupation/anxiety towards
certain food groups are also found to be related to disturbed eating
patterns. It is essential to highlight that populations with depressive
symptoms also often experience increased body image dissatisfaction,
binge eating and disordered eating behaviors [5]. Conversely,
low self esteem, poor body image issues and lack of social support
systems are also indicative as potential risk factors for depression
[6]. The bidirectional influential nature of these constructs along with the observed high levels of comorbidity between depressive and
disordered eating symptomatology warrants a further investigation
to explore the relationship between the two.
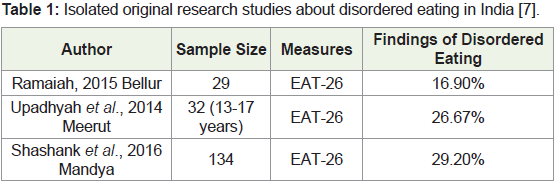
Furthermore, it is essential to highlight that there is a paucity of
research in India to determine the prevalence of eating disorders and
disordered eating behaviors due to under-reporting concerns [7].
Although, there have been small and isolated studies in the recent
past that indicate the prevalence of disordered eating in India between
16.9% to 29.2% (Table 1).
Majority of the studies conducted in India have predominantly
employed the Eating Attitudes Test- 26 item (EAT- 26) measure as the
chosen screening tool [7]. However, the EAT-26 aims to assess eating
attitudes by calculating scores on only three subscales: 1) Dieting, 2)
Bulimia and Food preoccupation and 3) Oral Control. Alternatively,
the Eating Disorder Examination Questionnaire (EDE-Q) is
considered to be the clinical gold standard screening tool to evaluate
the presence of key behavioural and cognitive features present in
disordered eating, as well as eating disorders [4]. The EDE-Q has
shown to have good internal consistency, high validity and sensitivity
[8]. The Depression Anxiety Stress Score (DASS‐21) questionnaire is
a well‐established instrument for measuring depression, anxiety, and
stress with good reliability and validity reported across cultures [9].
The dearth of Indian research on disordered eating behaviors
coupled with the above stated bidirectional influence calls for
further empirical inquiry. This lends an opportunity to conduct a
study examining the relationship between mental health concerns
and disordered eating in the context of COVID-19. The research
proposes that a significant positive Pearson’s correlation will be
observed between mental health concerns (depression, stress and
anxiety scores) and disordered eating scores during the country-wide
lockdown.
Method
A 60 item master survey was developed by compiling the 33
item EDE-Q and the 21 item DASS-21 questionnaires, in addition
to six demographic questions. Previously validated questionnaires
were chosen as they have been extensively tested in the past and thus
correctly calibrated to their target [10-12]. A voluntary response
sampling method was employed. A web-based survey approach was
selected in light of the national lockdown. Compared to manual
entry, web-based surveys are time and cost effective. Further, they
improve data collection quality and response rate compared with
alternative survey forms [13]. The web-based nature facilitated the
survey to reach various regions of the city of Mumbai, India. The
survey platform employed was Google Forms.
Participants: The 15 minute master survey was electronically distributed to
young males and females (age 15-30) residing in the city of Mumbai,
India during the national lockdown in the month of May 2020.
Survey: The survey was divided into two main parts, DASS-21 questions
and EDE-Q questions. The DASS- depression subscale focuses on
reports of low mood, motivation, and self-esteem. The DASS-anxiety
on physiological arousal, perceived panic, and fear. Lastly, the DASSstress
subscale on tension and irritability [14].
The EDE-Q is a 33 item questionnaire developed by Fairburn
and colleagues addressing cognitive features of eating disorders over
the past 28 days [15]. It includes subscales like Eating Concerns,
Shape concerns, Weight Concerns and Dietary Restraint. The mean
of the subscales was employed to calculate the overall EDE-Q global
score [15]. This global score was then correlated with the DASS-21
subscales.
Statistics: The responses were maintained on Microsoft Office Excel. Subscale
scores and global scores of the respective validated questionnaires
were calculated in accordance to the questionnaire guides. One-tailed
Pearson’s correlation was conducted using the Statistical Package for
the Social Science (SPSS) Statistics software [16,17].
Results
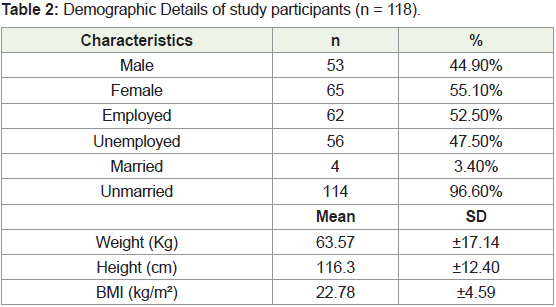
One hundred and eighteen (n=118) complete responses of youth
aged 15-30 years from Mumbai, India- were received electronically.
Out of the total number of responses 53 (44.9%) were male and 65
(55.1%) were female. More than half of the participants (76; 64.4%) were
between 21-25 years of age. Most of the participants were unmarried
(114; 96.6%). The mean weight, height and BMI of the participants
were 63.57 kgs, 116.3 cm, 22.78 kg/m2 respectively (Table 2).
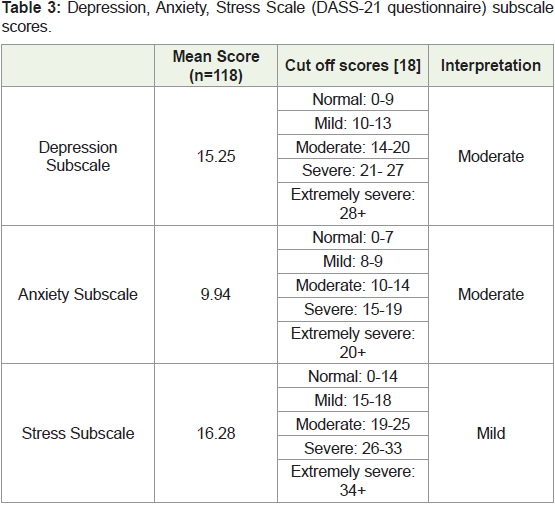
DASS-21 scores: As per the DASS-21 questionnaire, the mean scores during the
national lockdown for the depression and anxiety scales were 15.25
and 9.94 respectively - which is observed as moderate levels of
severity. The mean score for the stress scale was 16.28; indicating mild
levels of stress (Table 3).
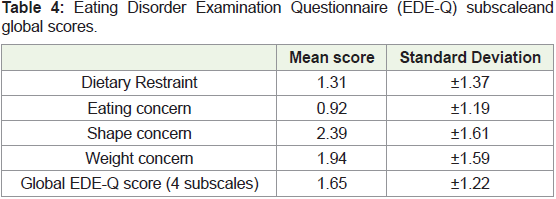
EDE- Q scores: The mean scores of the EDEQ subscales i.e., dietary restraint,
eating concerns, shape concerns and weight concern were computed.
Out of the four subscales, the mean score of shape concern appeared
to be the highest (2.39 ± 1.61), followed by weight concern (1.94 ±
1.59), dietary restraint (1.31 ± 1.37) and eating concerns (0.92 ± 1.19).
The mean global EDE-Q score was 1.65 ± 1.22 (Table 4).
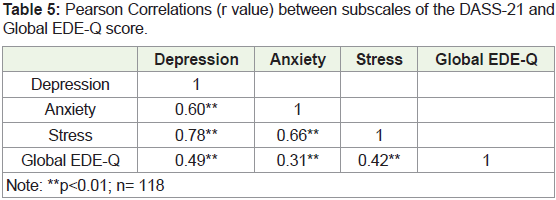
Correlation: DASS-21 depression, anxiety and stress subscales, individually
showed a significant positive correlation with the EDE-Q global
disordered eating scores i.e. r=0.49, p<0.01; r=0.31, p<0.01; r=0.42,
p<0.01 respectively (Table 5).
Discussion
This study is one of the preliminary studies that compares
disordered eating behaviours with depression, anxiety and stress in a South Asian sample population. Validated questionnaires have
been used to assess the said variables. The present study showed that
amongst the DASS-21 subscales - the scores for depression and anxiety
subscales were of moderate severity at 15.25 and 9.94 respectively,
while the mean score for the stress subscale was of mild severity at
16.28. For the EDEQ subscales, the mean score of shape concern
appeared to be the highest (2.39 ± 1.6), followed by weight concern
(1.94 ± 1.59), dietary restraint (1.31 ± 1.37) and eating concerns (0.92
± 1.19). The mean global EDE-Q score was 1.65 ± 1.22. The present
study also showed that there are significant positive correlations
between disordered eating with depression (r=0.49; p<0.01), anxiety
(r=0.31; p<0.01) and stress (r=0.42; p<0.01) respectively.
In the past, studies have explored correlations between
disordered eating with mental health concerns [19-21]. Most recently
a correlation between stress and disordered eating in first year college
women was found [22]. Gan and colleagues have also found positive
correlations between stress, anxiety, depression and disordered eating
[21]. The current study was set up to re-examine these variables in a
South Asian sample population in the backdrop of the COVID-19
lockdown. The results show to be in line with the outcome of previous
studies.
Furthermore, examining the observed EDEQ individual subscale
scores could facilitate researchers to explore potential reasons for
weight and shape concerns to be relatively higher than eating concerns
during the national lockdown. This period, marked with isolation and
social distancing, seemed to have left individuals and communities
excessively using mass media as a coping tool. Social media platforms
have seen a 61% increase in consumption as people employ the
platforms to stay connected with family, friends, and colleagues [23].
The excessive usage of platforms such as instagram does serve as a
potential explanatory force to better comprehend why shape concern
is relatively high in the light of lockdown. A recent qualitative study
exploring instagram use and body image suggests how participants
were inclined to adhering to a variety of beauty standards by
responding to beauty ideals such as comparing self with others,
and displaying of self. Participants reported significant appearance
dissatisfaction when trying to achieve these ideals and frequently
compared their photos to the number of likes with others using the
platform [24]. One could also draw light on the nature of the content
displayed on these platforms during the lockdown. A British study
examining the impact on COVID-19 on those with eating disorders
states that there was an increase in posts about physical activity (eg.
sharing daily exercise routines) and “fear of gaining weight” during
the lockdown [25]. There is also some evidence highlighting higher
anxiety being significantly associated with higher weight change
perception during COVID-19 [26]. Thus, the influx of such content
on social media may be a potential contributor to a relatively higher
shape and weight concern in the present study participants.
On the other hand, interestingly-participants scored the lowest
on the eating concern subscale. The speculated reasons for this may
be twofold. Firstly, the lack of availability of a variety of foods, with
access to only staples may have made individuals more open to consuming foods that are available even if it is uncharacteristic of
their regular food choices. Secondly, social influences of eating may
have reduced with the confinement - leading to higher degrees of
food freedom. The effect of social comparison on eating behaviours
has been discussed in the past. Polivy outlines how people tend to
alter not just the amount of food eaten (e.g. women may tend to eat
lesser when they want to make a positive impression on someone) but
also the kind of food eaten (eg. men avoid eating quiche and other
“lady foods,” and choose more hearty meals) in a social setting [27].
It could also be inferred that the uncertainty and lack of control
individuals experience during a lockdown causes significant anxiety
that they wish to diminish by regaining control in other life spheres.
Taking control of their diets, food intake, body shape, size and form
could potentially be a sphere that individuals employ to channelize
their distress and reclaim their control and power. There is adequate
evidence through time, indicating the impact of emotions on eating
behaviours across cultures [28-30]. Similarly, in such trying times,
one can speculate how food can be used as a coping mechanism,
and provide comfort - thus reiterating the influence of mental health
concerns on eating behaviours.
There are certain limitations in the present study. The participating
sample size (young males and females in Mumbai, India) limits
generalizability to other groups and contexts. Moreover, web-surveys
can make it difficult to assess the degree of functionality of the sample
population. It is essential to note that the data collection measures
employed are self-report and are subject to self-report biases. The
limited cultural sensitivity of the screening tools employed is crucial
to highlight, since they have been used on an Indian sample. Lastly,
it is important to highlight that correlation research does not imply
causation and hence there could be several other mediating variables
that could explain the relations observed which cannot be overlooked.
Looking forward, there are significant, widespread and impactful
implications for the findings of the study. It creates awareness about
the relation between depression, anxiety, stress and disordered eating.
Moreover, it also opens avenues for further discussions for creating
an interdisciplinary approach amongst mental health professionals
and dietitians to be able to provide appropriate collaborative care,
as well as early interventions to prevent clinical eating disorders.
The study also contributes to disordered eating and mental health
disorders literature within a South Asian cohort, especially during the
unconventional COVID-19 era. Larger, temporal and causal studies
are required to further investigate and confirm the relation between
disordered eating behaviours with mental health concerns.
References
Citation
Bhatia IN, Kishnani R. India Lockdown: Relationship between Disordered Eating and Mental Health Concerns. Indian J Nutri. 2021;8(1): 224.