Letter to Editor
Pragmatic Covid-19 Nutrition Protocol
Saseedharan S*, Annapurna and Kadam V
Department of Critical Care, S.L. Raheja Hospital- a Fortis Associate, India
*Corresponding author: Saseedharan S, Department of Critical Care, S.L. Raheja Hospital- a Fortis Associate, Mumbai, Maharashta, India, Pin Code: 400016, Tel Num: 00919004479549; E-mail address- docsanjith@rediffmail.com
Article Information: Submission: 12/10/2020; Accepted: 29/10/2020; Published: 03/11/2020
Copyright: © 2020 Saseedharan S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Letter to the Editor
We write to you regarding a pragmatic nutritional protocol that
our tertiary care institute has been following which has helped to
make critical care nutrition safe, scientific and objective with minimal
risk.
Introduction
The clinical spectrum of COVID-19 disease appears wide
encompassing ranging from asymptomatic infection to mild upper
respiratory tract infection, and severe pneumonia with respiratory
failure. Cardiac and renal failure has also been seen. These patients are
known to deteriorate rapidly. Most severe complications and deaths
are reported among older patients with evidence of premorbid illness
such as cardiovascular, liver, kidney disease, or cancer.
C-reactive protein, and serum albumin have been shown to be
independent prognostic markers and serum albumin is a good marker
for the nutritional status as well. Although albumin is not exclusively
dependent on nutritional status, it is part of several nutritional
screening indices and is associated with nutritional conditions.
Interestingly, low prealbumin levels, another marker of malnutrition,
have been demonstrated to predict the progression to respiratory
failure and mechanical ventilation. This evidence strengthens the
concept that nutritional derangements should be systematically and
urgently managed in patients affected by COVID-19, also considering
that the immune response has been shown to be weakened by
inadequate nutrition. The author’s institute has been catering to the
maximum number of Covid-19 patients in the city of Mumbai for the
last 4 months as this is a dedicated Covid hospital. Since knowledge,
experience and practice sharing is so important the authors decided
to write this article.
Covid- 19 Nutritional Challenges
These are the challenges faced in the Indian ICUs
• Staffing is a problem in view of adjustments in various ICUs,
restriction in the number of duty hours and offs given.
• Fear among dieticians to enter the COVID ICUs.
• Food and beverage are generally dependent on these dieticians
for getting their input, which is now not there and thus left in a bad
shape.
• Kitchen feeding becomes problematic as individual feeding is
difficult with low staff and staff in PPEs.
• Food recall is a problem.
• Because of the need of a paperless system, diet charts are a
problem, thus we need software for both nutritional assessment and
diet.
• Diet should be planned in such a way that it is in the same time
as medication, thus decreasing the time of contact of staff with the
patient (clustering of activities).
• Wide availability of three in one (total parenteral nutrition)
bags and powder based nutrition.
The protocol:
Keeping in mind all the above, we have an” India” specific
protocol (using products available in India and Asian countries) that
can be implemented all over the country easily by bed side nurses. It
is simple, nurse managed, has timely doctor feedback and is evidence
based as much as possible. The early nutritional supplementation
protocol that is being followed in our tertiary care center we call as
“dr sanjith’s protocol” is summarized in Figure 1.On admission to the ICU, the height and weight of the patient
is taken, actual weight if the patient can stand and an approximate
weight if the patient cannot stand. Malnutrition screen using
NUTRIC score and NRS 2002 is carried out.
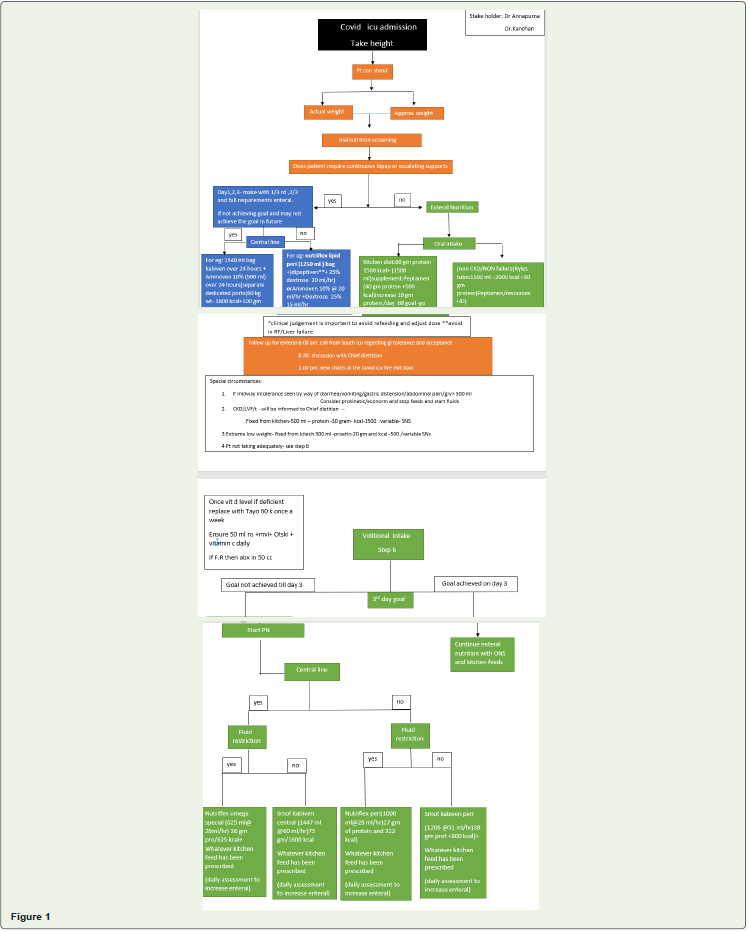
The goal is to achieve target calorie and protein requirements by
day 3 of admission.
Scenario 1: If the patient is just requiring oxygen support, enteral
nutrition is started which consists of kitchen diet with 60 gm protein
and has 1500 k cal. Oral nutrition Supplement with Peptamen 40 gm
protein and 500 kcal is started. Increase the proteins by 10 gm per day
later to achieve calorie and protein goal.
In case of CKD /Poor cardiac function (EF), the chief dietician is
informed about fluid restriction and feed from kitchen is 500 ml, with
30 gm protein and 1500 k cal.
Scenario 2: If the patient is on escalating support of thus not
capable of taking oral diet, ryles tube feeds need to be started. In
this patient if no fluid restriction, 2000 k Cal with 90 gm protein,
Peptamen /resource HD with 1500 ml fluid should be started. If
the patient is on BiPAP, we still start enteral feeding as described
above. But if the requirement of BiPAP is continuous or requirement
of support is escalating, the patient will not be able to take enteral
nutrition adequately.
If both the above stated scenario patients intake is not adequate,
goal is not achieved by day 3, start parenteral nutrition. If the patient
has a CVP line and has fluid restriction Nutriflex omega special (625
ml@ 26 ml/hr) 36 gm proteins /625 kcal along with whatever kitchen
feed has been prescribed. Access the patient daily to increase enteral
feed.
If there is no fluid restriction and goal is not achieved then,
consider TPN like Smofkabiven central (1447 ml @60 ml/hr) 75
gm/1600 kcal along with the prescribed kitchen diet. Access daily to
increase enteral nutrition.
If this patient has no central line, peripheral parenteral nutrition
should be started to achieve the goal. Nutriflex peri (1000 ml@28 ml/
hr) 27 gm of protein and 322 kcal) along with whatever kitchen feed
has been prescribed. Access daily to increase enteral feed. If the patient has a fluid restriction and has no central line, peripheral parenteral
nutrition Smofkabiven peri (1206 @51 ml/hr) 38 gm protein +800
kcal) along with whatever kitchen feed has been prescribed.
Scenario 3: If the patient is on escalating BiPAP support,
parenteral nutrition needs to be started to achieve nutritional goal.
If patient has a central line- kabiven 1540 ml is given over 24 hrs
along with Aminoven 10 % 500 ml using a dedicated port. This gives
1800 k cal with 100 gm protein. Monitor patient to avoid refeeding.
If the patient does not have a CVP line, peripheral nutrition is
started-like nutriflex lipid peri- 1250 ml bag. This is given along with
dipeptiven (avoid in renal failure and liver failure), 25 % dextrose at
30 ml per hr or aminoven 10 % at 20 ml per hr with dextrose 25 % 15
ml per hr.
If the patient has diarrhoea, vomiting, gastric distention, pain
abdomen or a gastric residual volume of >500 ml, consider prokinetic
agents, econorm, stop feeding and start IV fluids.
In patients with vit D deficiency, ensure supplementation of Vit D
along with Multivitamin and micronutrients like Otski. If all these are
increasing the fluid intake, restrict fluid from antibiotics.
Conclusion
Implementing prompt and adequate nutrition in these patients
with COVID-19 disease is a difficult challenge owing to the current
dramatic emergency circumstances, unknown course and patient
profile. However, all efforts should be made to try to guarantee
adequate nutritional support to hospitalized critically ill patients, as it
may be potentially be beneficial to clinical outcomes and effective in
reducing or preventing the deleterious consequences of malnutrition.
Presently there is three month follow up of patients having gone
through the protocol with respect to their body weight, morbidity
and serum albumin levels and results are awaited and preliminary
results seem encouraging. The above protocol has been used to close
to 200 intensive care patients and has made nutrition delivery in the
intensive care short, simple, scientific, objective and safe.