Research Article
Operational Experience of Community-based Provision of Ready-to-use-food (RUTF) to Young Children with Severe Wasting in Urban Informal Settlements of Mumbai, India
Jayaraman A*, Chanani S, More NS, Waingankar A, Fernandez A and Pantvaidya S
Society for Nutrition, Education & Health Action, Mumbai, Maharashtra, India
*Corresponding author: Anuja Jayaraman, Director- Research, SNEHA, Behind Bldg. No. 11, BMC Colony, Shastri Nagar, Santa
Cruz (W), Mumbai- 400 054, India, Tel: (+91 22) 26614488 / 26606295 /24040045; Email: anuja@snehamumbai.org
Article Information: Submission: 19/06/2019; Accepted: 06/08/2019; Published: 08/08/2019
Copyright: © 2019 Jayaraman A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Background: In India, approximately 7.5 percent of children under five experience severe wasting (low weight-for-height), a measure of severe acute
malnutrition (SAM). The WHO and UNICEF recommended the provision of ready-to-use therapeutic foods (RUTF) in community-based programs to treat
uncomplicated severe acute malnutrition. In our first objective, we assess the process outcomes of community-based screening for severe wasting and
provision of RUTF through community health workers. Second, we compare recovery outcomes of severely wasted children who reportedly consumed MNT
with those who reported consuming none to insubstantial quantities of MNT.
Methods: The study follows a case series without a control methodology similar to other program reviews. To compare characteristics of children across
treatment groups, we use Pearson’s chi-squared tests and to examine recovery outcomes, 8-week anthropometric status is calculated.
Results: Among the 543 children followed up, out of the 338 (62%) who went to a health camp or the NRRC, 174 were confirmed as severely wasted by
a doctor, passed an appetite test for MNT, and given a prescription for MNT. Among those who consumed MNT, nearly forty percent of the < 28 cups children
remained severely wasted at the time of their anthropometric measurement closest to the 8-week mark as compared with 19% of the 28+ cups children. While
a similar percentage of children (about one-quarter) across both groups had fully recovered to no longer being wasted, more children in the 28+ consumption
group had shown improvement to moderate wasting (53 percent moderately wasted as compared to 36 percent in the < 28 cups group).
Conclusion: Implementation strategies to improve diagnosis of severe wasting, provision of RUTF, and compliance with RUTF dosages are required.
However, the costs and efforts involved in effective coverage of MNT in large-scale community-based programs may not justify the potentially small
improvements in recovery.
Keywords
Child Health, Ready-to-use therapeutic foods, Urban Health, Community-based nutrition program, Acute Malnutrition, Medical Nutrition Therapy, India
Abbreviations
SAM: severe acute malnutrition; RUTF: ready-to-use therapeutic foods; IAP: Indian Academy of Pediatrics; SNEHA: Society for Nutrition, Education and Health Action; ICDS: Integrated Child Development Services; MCGM: Municipal Corporation of Greater Mumbai; MNT: Medical Nutrition Therapy; NRRC: Nutritional Rehabilitation and Research Centre; LTMGH: Lokmanya Tilak Municipal General Hospital; WHZ: weight-for-height; HAZ: height-for-age; WAZ: Weight-for-age; ENA: Emergency Nutrition Assessment; CHWs: community health workers; SD: standard
deviations; PPI: Progress out of Poverty Index; PPP: Purchasing Power Parity; TEM: technical error of measurement; CMAM: Community-based Management of Acute Malnutrition
Background
In India, approximately 7.5 percent of children under five
experience severe wasting (low weight-for-height) [1], a measure of severe acute malnutrition (SAM) strongly associated with mortality,
morbidity, and impaired cognitive development [2]. The WHO and
UNICEF recommended the provision of ready-to-use therapeutic
foods (RUTF) in community-based programs to treat uncomplicated
severe acute malnutrition. RUTF are energy-dense lipid pastes
enhanced with micronutrients that do not require refrigeration or
any close medical supervision to consume [3,4].
Evidence on the effectiveness of RUTF in community-based
programs is primarily from African settings with a few examples from
South Asia, which has the greatest burden of child wasting [5-7]. A
2013 Cochrane review concluded that based on the limited evidence,
definitive conclusions on the effectiveness of RUTF in comparison
to standard diets or other RUTF formulations could not be reached
[8]. In one large Indian randomized multi-center trial, locally
produced RUTF performed better in recovery and weight gain than
augmented home-prepared foods in community-based treatment of
uncomplicated severe wasting. However, RUTF was insufficient to
bring about recovery for over 40% of the severely wasted children,
and among the recovered children, relapse rates were high [9]. The
Indian Academy of Paediatrics (IAP) has recognized the potential
benefits of RUTF in India, but has noted the urgent need for research
on operationalization in diverse settings [10].
Given the immense challenge of child malnutrition in India,
comprehensive and multi-sectoral approaches are required to
prevent, treat, and sustain the recovery of children with acute
malnutrition. From December 2011 through March 2016, the Society
for Nutrition, Education and Health Action (SNEHA) implemented
a community-based child nutrition program to prevent and treat
wasting in urban informal settlements of Dharavi, Mumbai. The
program was implemented in collaboration with the largest national
child welfare program, the Integrated Child Development Services
(ICDS) and with the Municipal Corporation of Greater Mumbai
(MCGM). The intervention covered the service areas of 300 ICDS
Anganwadis (child care centers), a population of approximately
300,000. Through screening, referral to public health facilities for
immunization, deworming, treatment of complications, OPD care in
medical camps, growth monitoring and home-based counseling, the
program achieved a reduction of 19% in wasting levels in intervention
areas [11].
As part of the program activities, eligible severely wasted children
could access RUTF, as a supplement to their regular diets, called
Medical Nutrition Therapy (MNT), produced by the Nutritional
Rehabilitation and Research Centre (NRRC) at Lokmanya Tilak
Municipal General Hospital (LTMGH). The Indian Institute of
Technology Bombay and Toddler Food Partners (USA) formulated
the MNT paste. An MNT cup (100 gram/540 kcal) consisted of milk
powder, sugar, vegetable oil, peanut butter, vitamins, and minerals
[12]. The objectives of this study are two-fold. Given the lack of
operational evidence on multi-sectoral approaches to providing
RUTF to severely wasted children at the community-level in urban
informal settlements of India, we assess the process outcomes of
community-based screening for severe wasting and provision of
RUTF through community health workers. Secondly, we compare
recovery outcomes of severely wasted children who reportedly consumed MNT (and other services) with severely wasted children
who reported consuming none to insubstantial quantities of MNT
(but also received other services).
Methods
Provision of MNT in the child nutrition program:
Figure 1 provides an overview of the treatment and followup
activities for children screened as wasted in the child nutrition
program. Children that SNEHA CHWs and ICDS Anganwadi
workers screened as wasted (severe or moderate) were referred
to SNEHA community-based health camps. At the camp, a
pediatrician confirmed the child’s severe wasting status and then
provided an appetite test for MNT to children over six months of
age. Alternatively, children screened for severe wasting could go to
the NRRC for a similar medical screening and MNT prescription.
Most children (> 75 percent) utilized the SNEHA community-based
health camps due to the nearer proximity to their homes as compared
with the NRRC. MNT prescriptions provided by both the NRRC and
SNEHA doctors were typically 1-2 cups daily over an 8-week period.
SNEHA provided the MNT supplements free of cost to mothers and
SNEHA community health workers (CHWs) ensured delivery of the
cups to the homes of children and supervised mothers to feed MNT
to the children who had received MNT prescriptions.While all children were monitored for growth every month
at ICDS Anganwadis, SNEHA CHWs took anthropometric
measurements of severely wasted children more frequently, aiming
for at least once a week. More detailed descriptions of activities are
available in the program evaluation paper [11].
Data Collection:
In August 2014, SNEHA began implementing a new tracking
system for the MNT component of the program through CommCare,
an Android-based mobile application designed for community health
workers. During the screening, each child received a unique ID in the
CommCare system, and along with their anthropometric information
(weight and height), SNEHA CHWs collected some basic socioeconomic
information. The use of electronic data collection improved
the monitoring of prescription, pick-up, delivery, and consumption
of MNT for each child.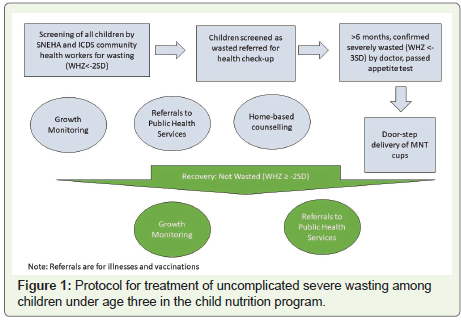
SNEHA CHWs collected and updated anthropometric data
in CommCare each time the child was measured. Children were
categorized as severely wasted, moderately wasted, or not wasted
based on WHO 2006 simplified weight-for-height/length field tables
[13]. SNEHA CHWs were repeatedly trained in anthropometry with
cross-checking of measurements by supervisors. After a child was
screened as severely wasted, the SNEHA CHW entered details of
whether the child went to a health camp or the NRRC, and if an MNT
prescription had been given. Each time the SNEHA CHW delivered
MNT cups to the child, she entered information on how many cups
of MNT had been consumed since her last visit.
The protocol, questionnaires, and informed consent forms for the
evaluation were reviewed and approved by the Institutional Ethics
Committee of the Bandra Holy Family Medical Research Society,
Mumbai.
Study Design:
The study follows a case series without a control methodology
similar to program reviews in Malawi [14,15], Myanmar [16], and
tribal regions of central-eastern India [17]. The Malawi studies
examined 8-week recovery outcomes of malnourished (moderate,
severe, or oedematous) children enrolled in operational homebased
therapy with RUTF, measuring both clinical status (defined
as recovered, failed, died or dropped out) and weight gain. The
Myanmar study similarly examined the effectiveness of a low-dose
RUTF program by assessing clinical recovery and weight gain for
children with uncomplicated SAM. The cohort study in tribal India
examined program effectiveness of community-based treatment of
severe acute malnutrition by assessing recovery to non-wasting status
as well as average change in WHZ score.Outcomes for children in this study are analyzed for the period
between August 2014 and March 2016, when the monitoring system
for MNT distribution was deployed on the Android phones. Children
included in the study are all children aged 6-36 months and screened
as severely wasted between August 2014 and January 2016 (to allow
for 8-week follow-up).
While CHWs used the WHO field tables for identification of
wasting, the analysis in this study utilizes anthropometric Z scores-
WHZ (weight-for-height), HAZ (height-for-age), WAZ (weightfor-
age)- calculated using Emergency Nutrition Assessment (ENA)
software. The criteria for moderate wasting used in the study are
children with weight-for-height/length z-scores (WHZ) lower than
two standard deviations (SD) below the median WHO growth
standards and equal to or above three SD below the median; severely
wasted children have WHZ scores lower than three SD below the
median WHO growth standards.
Excluded children were either: marked as an “incorrect” screening
by the SNEHA CHW; residing in an unidentifiable Anganwadi
location; screened with a WHZ score that was not approximately
<-3 SD after calculating ENA z-scores; screened with a WHO outlier
WHZ score; and marked as failing to pass the MNT appetite test.
Process Outcomes Assessed:
To examine the operational outcomes of the program the study includes: 1) the number of children who accessed a SNEHA health
camp or the NRRC after being screened for severe wasting; 2) among
those who followed through with the above referral, the number
of children who subsequently were confirmed as severely wasted
and given an MNT prescription. The study also evaluates effective
coverage by examining the outcome of the number of children who
consumed at least 28 cups of MNT within eight weeks of receiving
their MNT prescription.Recovery Outcomes Assessed:
The study evaluates recovery to non-wasted and improvement
to moderate wasting status during the 8-week MNT treatment phase
(WHZ ≥-2 SD). Additionally, the study measures mean weight gain
per kilogram body weight per day (g kg-1 day-1) and mean change in
WHZ score during the 8-week treatment period.Statistical Analysis:
To compare characteristics of children across treatment groups,
we use Pearson’s chi-squared tests (and Fisher’s exact for counts less
than 5) to compare the distribution of categorical variables and t-tests
to compare means for continuous variables. To examine recovery
outcomes, 8-week anthropometric status was calculated using the
most recent height and weight measurements available closest to
the exact date, eight weeks after the child was screened as severely
wasted by the CHW. Weight gain (g kg-1 day-1) was calculated as
the difference between the 8-week weight and screening weight, in
grams, divided by the screening weight, in kilograms, divided by the
number of days between measurements. For all 8-week follow-up
measurements, children with WHO outlier z-scores (WHZ, WAZ,
HAZ) were dropped from the analysis. We used the Progress out
of Poverty Index (PPI) to measure poverty levels. It estimates the
likelihood that a household is living below the international poverty
line of $2.16 per day Purchasing Power Parity (PPP). Designed to
measure poverty in India, the 2008 PPI includes ten questions about
household characteristics including occupation, number of children,
and large and small assets.Results
Between August 2014 and January 2016, 663 children aged 6-36
months were screened as severely wasted by SNEHA CHWs and
ICDS Anganwadi workers. Exclusions from this group included
55 children with screening WHZ scores inconsistent with a severe
wasting nutritional status; 50 children marked as outliers according
to WHO standards (WHZ, WAZ, and HAZ); and four children who
failed the appetite test.
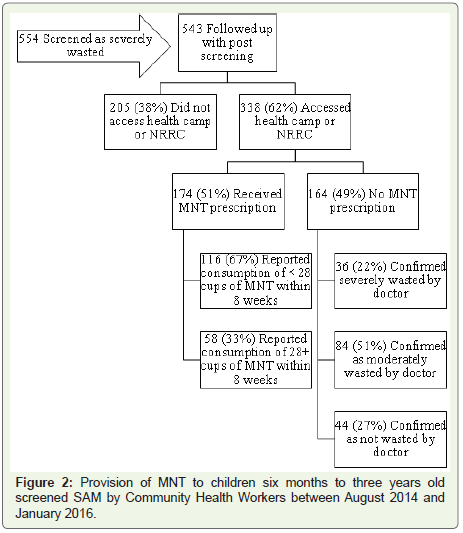
Process Outcomes:
The final analysis included 554 children screened as severely
wasted. CHWs were not able to follow up with eleven (2%) children
after they were screened. Figure 2 depicts the process flow of children
from screening through the provision of MNT.205 (38%) of 543 children screened as severely wasted did not
access either the SNEHA Health Camp or the NRRC. Without this
further medical assessment, the child did not have the opportunity
to get an MNT prescription through the child nutrition program. Among the 338 children (62%) who went to a health camp or the
NRRC, 174 were confirmed as severely wasted by a doctor, passed an
appetite test for MNT, and given a prescription for MNT.
The doctor did not give 164 of the 338 children who accessed the
health camp or NRRC an MNT prescription. Most of these children
were not given prescriptions because they were no longer severely
wasted by the time they reached the doctor; by the time they attended
the health camp, 84 children were measured as moderately wasted
(MAM) and 44 were measured as not wasted at all. The mean number
of days that passed between screening to accessing the health camp or
NRRC was 22 days for the 174 children that got MNT prescriptions;
for the 164 children that did not get a prescription, the mean number
of days that passed was 60 days. There were 36 children confirmed
as severely wasted that did not receive an MNT prescription. The
reasons for this could not be determined from the data.
Consumption of MNT:
Since dosages were typically between 1-2 cups per day, we assessed
consumption by grouping children based on whether they consumed
at least half (28 cups) of a minimum 8-week dose (56 cups) within
eight weeks from the date of prescription. Reported compliance with
consumption of prescribed MNT varied considerably across children
who received MNT prescriptions. 116 (67%) of the children who got
MNT prescriptions reported total consumption of fewer than 28 cups
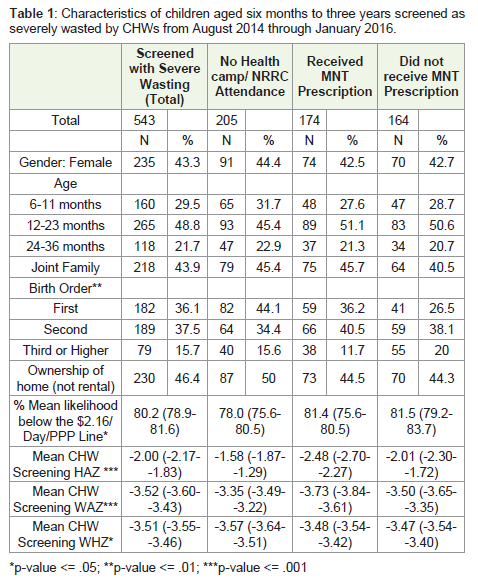
(Figure 2).Among the children screened as severely wasted by CHWs, Table 1 compares the characteristics of children across the groups of
children according to process outcomes (No Health Check-up, MNT,
No-MNT). No Health Check-up children were more likely to be firstborns-44 percent as compared with 36 (MNT) and 27 (No-MNT)
percent. This group was also less likely (78 percent as compared to 81
(MNT) and 82 (No-MNT) percent) to be living below the $2.16/day/
PPP poverty line.
The MNT group had significantly worse screening nutritional
status for stunting (mean HAZ of -2.48) and underweight (mean
WAZ of -3.73) status, as compared with No Health Check-up and
No-MNT groups. The No Health Check-up group had the highest
mean wasting (-3.57 WHZ) screening status.
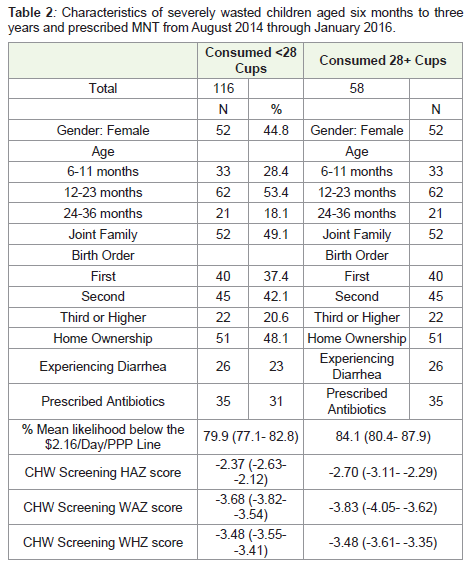
To assess whether children who consumed more MNT had
better recovery outcomes as compared with those who did not
consume substantial quantities of MNT, we narrowed the analysis
to the 174 children who were confirmed as severely wasted by a
doctor and received an MNT prescription. Table 2 compares the
characteristics of the two consumption groups (<28 cups and 28+
cups). Characteristics of both groups were generally similar; none
of the observed differences, such as gender and poverty levels, were
significant.
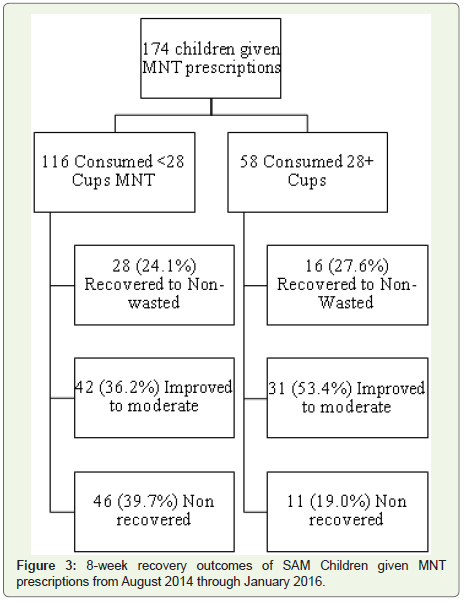
Figure 3 and Table 3 compare the recovery outcomes for the
28+ cups and <28 cups groups. Nutritional recovery status was
significantly different (at p-value <0.02). Nearly forty percent of
the <28 cups children remained severely wasted at the time of
their anthropometric measurement closest to the 8-week mark as
compared with 19 percent of the 28+ cups children. While a similar
percentage of children (about one-quarter) across both groups had
fully recovered to no longer being wasted, more children in the 28+ consumption group had shown improvement to moderate wasting
(53% moderately wasted as compared to 36% in the <28 cups group).
Discussion
This study demonstrates the challenges of effective implementation
of RUTF in large-scale community-based programs in urban informal
settlements. Over one-third of children screened as severely wasted
did not seek out health care at the health camp or NRRC. Temporary
and permanent migration of families and children may have played a
role in poor access of the health camp or NRRC. In the intervention
communities, the program experienced high levels of movement
internally within the informal settlement, and externally to other
parts of Mumbai and India. This challenge to service provision has
been observed in other maternal and child health programs working
in urban areas of Bangladesh [18]. A lack of positive health-seeking
behavior by caregivers of children screened as severely wasted reflects
the community-wide perception that malnutrition is not an illness
that requires medical intervention. This challenge, well-documented
in a qualitative study of poor coverage in a CMAM program in Bihar
[19], has been a critical aspect of the intervention design where the
first counseling session (“I am a good mother”) given to the mother
of a wasted child focuses on appreciating the caregiver.
Additionally, in urban informal settlements of Mumbai,
community-level public health services are often underutilized in
favor of the private sector or tertiary hospitals because residents
often perceive public services negatively or as inferior [20]. The
characteristics of children who did not access the health camp
or NRRC suggest they may be better-off and perhaps caregivers
have sought alternative care through private practitioners. The
child nutrition program should further explore the health-seeking
behavior of caregivers whose children have been screened for wasting
and ensure that caregivers are well-informed about the quality of care
provided through public services.
About half of the children who followed-up with SNEHA or
NRRC medical screening were not severely malnourished by the time
they attended. The two possible reasons for the discrepancy between
the SNEHA CHW screening status and confirmation status are 1) the
long time that elapses between screening as severely wasted and the
child’s access of a health check-up for confirmation 2) measurement
error by CHWs during screening.
With respect to the time lag in accessing the health camp or NRRC, the staffing of one single pediatrician was inadequate; for
most households, the health camp was available in a nearby area
approximately only once a month. Thus, the staffing of additional
pediatricians and an increase in the frequency and locations of health
camps could have improved access and more timely confirmation
and treatment of severely wasted children.
Measurement errors in screening are an expected challenge
in community-based screening for wasting by CHWs [21]. Along
with the usual challenges of maintenance of equipment, proper
positioning, and clothing removal, urban informal settlements
have uneven flooring, poor light, crowding and noise that can also
affect the quality of anthropometry taken. CHWs received intensive
training on anthropometry including standardization tests to
calculate the technical error of measurement (TEM). Supervisors
monitored regular calibration of electronic baby weighing scales
(manufactured by Nitiraj Engineers Pvt. Ltd., accuracy of + /- 10
grams) and conducted frequent cross-checks of anthropometry data
collected.
The process outcomes also indicate low levels of reported MNT
consumption once a child had received a prescription. Other studies
in India have similarly found challenges in adherence to RUTF
consumption [22]; in the Indian RUTF trial, peer supporters had
to visit children several times a day to assist in feeding [9]. While
SNEHA CHWs provided regular delivery of MNT cups to the homes
of malnourished children, further research is needed to understand
the obstacles to consumption of RUTF. Anecdotally, CHWs noted
challenges in MNT consumption related to poor palatability and
caregiver concerns about the child’s likelihood of getting diarrhea
from a government-produced supplement.
The 8-week recovery outcomes for children prescribed MNT
indicate that fewer children remained severely malnourished if they
were more compliant with MNT consumption. Compared with
Sphere Minimum Standards for Outpatient Therapeutic Care in
Community-based Management of Acute Malnutrition (CMAM)
[23], if we consider recovery as moving out of severe wasting (into
moderate or not wasted status), then the 28+ cups group meets the
standard for recovery rate (recovery rate >75%). If we consider the
recovery rate as 15% weight gain, often used in traditional CMAM
programs, 24% (28 of 116) of the <28 cups group gained at least
15% of their weight and 38% (22 of 58) of the 28+ children gained
at least 15% (Table 3). Without randomization, causality cannot be
determined, but the results suggest that there may be benefits to MNT
consumption in improving the recovery rates of severely wasted
children. The greater percentage of 28+ children who moved into
moderate wasting status indicates that while MNT (in amounts often
less than the minimum prescribed dosage) may not help the child
into the not wasted status sooner, it may have facilitated children
moving out of the most vulnerable category of severe wasting.
Other Indian studies of community-based treatment of acute
malnutrition have also experienced poor recovery rates as compared
with those achieved by African programs. Small samples observed
in community-based programs in Chandigarh and central-eastern
tribal regions achieved recovery rates (using a 15% weight gain
criteria) of 46% and 58% respectively [17]. The Indian RUTF multicenter trial found that recovery rates (using WHZ ≥−2 SD) for the
two intervention arms using RUTF were 34.8% and 40.7% after eight
weeks [9]. The authors posit that recovery was likely slower among
Indian children as compared with their African counterparts due to
the different nature of acute malnutrition among Indian children
who usually experience Marasmus rather than Kwashiorkor. Our
study supports the experts who advocate that, for Indian children,
the persistent and widespread nature of malnutrition requires a more
sustained and comprehensive approach [7,24,25].
Due to the challenge of compliance and the amount of resources
that would be required to ensure compliance and implement
effectively, SNEHA has discontinued the use of MNT. Additionally,
there was little prospect for longer-term sustainability through
integration with ICDS. ICDS currently provides take-home-rations
to all children, and there is no plan for ICDS to focus specifically on
supplements for acute malnutrition.
Limitations
This study shares the operational experience of a communitybased
program to distribute a locally produced RUTF-one component
among many other activities that were aimed to reduce and prevent
wasting. For comparison of recovery outcomes, children were not
randomly assigned to MNT consumption and non-consumption arms;
children consuming <28 cups are likely to have other characteristics
that affect recovery outcomes other than those identified in the study.
Overall compliance with MNT consumption in this program was low
and thus sample sizes are small, limiting statistical precision and we
could not compare recovery outcomes at further disaggregated levels
of consumption [11]. Due to these limitations, further research would
be required to make conclusions about the efficacy of using RUTF
to treat severe acute wasting as compared with nutrient-rich foods
prepared at home.
Conclusion
The study provides insight into the operational challenges
and successes of community-based provision of RUTF in a largescale
multi-sectoral community-based program in urban informal
settlements of India. Further implementation strategies to improve
diagnosis of severe wasting, provision of RUTF, and compliance with
RUTF dosages are required. This includes tailoring the palatability of
the product to meet children’s needs. However, the costs and efforts
involved in effective coverage of MNT in large-scale communitybased
programs may not justify the potentially small improvements
in recovery.
Acknowledgement
We thank the families and caregivers in Dharavi who made
the study possible through their participation in the CMAM
program. We are thankful to EPIC Foundation and the funders
of the implementation activities. We are thankful to the Aahar
implementation team including Roselin Arul, Ganesh Balgude,
Sandeep Bange, Suchita Bavadekar, Vaijayanti Birwadkar, Anu
Bothra, Vanita Choundhe, Vyoma Dalal, Digambar Gaikwad,
Sushma Gaikwad, Meenakshi Goel, Varsha Kokate, Ganesh Mane,
Shreya Manjarekar, Manashree Mantri, Rohit Misale, Madhuri More,
Bhakti Naik, Anita Patil, Pradeep Pawar, Dr. Bharati Shanbaug, Usha Shinde, and Sarika Yadav. From Integrated Child Development
Services (ICDS) we thank Bapurao Bhavane (CDPO), Vanita Dethe,
Mahendra Gaikwad, Sandhya Pavnikar, Swati Kshemkalyani, Rekha
Sonawane, and Bharati Thakur. From Municipal Corporation of
Greater Mumbai (MCGM) we thank Dr. Prajakata Amberkar, Dr.
Satish Badgire, and Dr. Alka Jadhav. We are thankful to Arja Huestis
for her help in data collection and Pooja Vyas for her research support.
Finally, we are thankful to Vanessa D’Souza, Priya Agrawal, Archana
Bagra, Devika Deshmukh, Wasundhara Joshi, Evelet Sequeira,
members of the SNEHA Research Group, and the SNEHA trustees.
References
Citation
Jayaraman A, Chanani S, More NS, Waingankar A, Fernandez A, et al. Operational Experience of Community-based Provision of Ready06
to-use-food (RUTF) to Young Children with Severe Wasting in Urban Informal Settlements of Mumbai, India. Indian J Nutri. 2019;6(2): 204.