Research Article
Thiamine Deficiency in Alcoholics with Normal Body Mass Index
Shanmugiah A*
Department of Psychiatry, Coimbatore Medical College Hospital, India
*Corresponding author: Shanmugiah A, Department of Psychiatry, Coimbatore Medical College Hospital, Coimbatore-641018,
Dr. MGR Medical University, Chennai, India, E-mail: shanmugiah_dr@hotmail.com
Article Information: Submission: 17/05/2019; Accepted: 02/07/2019; Published: 05/07/2019
Copyright: © 2019 Shanmugiah A. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Ethanol consumption leads to nutritional deficiency due to various causes. Well known theoretical as well as literature supports the hypothesis on dietary
factors, metabolic derangement and alcohol per se produces empty calories. In this study completed in 2000 go hand in hand with the earlier observations
and the available literature after 2000. Nutritional deficiency in turn leads to Alcoholic brain damage which is reversible if identified early. Among the nutritional
deficiency Thiamine deficiency (Vitamin B6) appears as the most common findings across the studies. In this study also, thiamine deficiency was considered
based upon the increased serum Pyrophosphate level an indirect indicator of thiamine deficiency. In this study all the 40 samples were moderate drinkers,
diagnosed as Alcohol dependence syndrome according to ICD-10 DCR. No indicators of overt nutritional deficiency on clinical assessment by ICMR Scale,
Biochemical assessment and anthropometric assessment. Though very preliminary and cross sectional analysis, thiamine supplementation of all the drinkers
irrespective of the clinical and biochemical nutritional deficiency will prevent at large both acute and chronic alcoholic brain damage.
Background
Ethanol is a rich source of nutritional calories. So, that heavy
drinking is often complicated by malnutrition and vitamin deficiency
[1]. Malnutrition has been a well recognized accompaniment of
alcoholism [2]. The low concentration of nutrients in alcoholic
beverages cannot compensate for the reduced nutritional intake
of patients, whereas the alcohol may provide two third of the daily
caloric requirement, thereby producing nutritional imbalance.
Nutritional and vitamin deficiency is suggested by analogy with
Wernicke’s Korsakoff’s encephalopathy. Dietary inadequacy are
often exaggerated by malabsorption of Thiamine secondary to the
effect of circulating ethanol [3,4]. The chemical, biochemical and
pathological observations which have been made in Wernicke’s
Korsakoff’s syndrome strongly favor the contention that it represents
the human counterpart of experimentally induced thiamine
deficiency in animals [5]. Genetically determined abnormalities
in the thiamine dependent enzyme transketolase may explain why
only a subgroup of malnourished alcoholics have the Wernicke’s
Korsakoff’s syndrome [6]. Current research suggests that ethanol
related neurological disorders may be caused by a combination of
neurotoxic effects of ethanol or its metabolites, nutritional factors and genetic predisposition. Therefore it would be important to study
the relationship between alcohol consumption and nutritional status.
Ethanol intake appears to affect the thiamine status in three main
ways [7]. First, the diet of alcoholics are frequently low in thiamine
because the daily energy intake largely displaced by nutrient deficient
alcoholic beverages. Secondly, the metabolic demand for thiamine
is increased by the consumption of a diet rich in carbohydrate as
primary source of energy. Thirdly, alcohol can inhibit the intestinal
ATPase involved in the entire absorption of Thiamine. In young
healthy non alcoholic individuals, subjective symptoms appear after
2-3 weeks of deficient diet [8].
This study has been done in 2000 at De-addiction centre,
NIMHANS, Bangalore. There are very few studies actually focusing
on vitamins and alcoholic brain damage in developing as well as
developed countries. Hence we have retrospectively analyzed the
relevance of this study with similar studies in the past and present.
This study examined the relationship between nutritional parameters
in a group of alcohol dependent individuals without any clinically
manifest nutritional deficiency. The mechanism behind the nutritional
deficiencies in alcoholics include inadequate dietary intake, vomiting, diarrhoea, steatorrhoea, reduced absorption of vitamins and minerals,
increased metabolic demands and impaired utilization. Ethanol
consumption in a bomb calorimeter indicates a caloric value of
7.1kcal/g. But, there are empty calories, since the alcoholic beverages
are almost devoid of other nutrients like vitamins and trace elements.
Alcohol induced gastritis, Pancreatitis and liver disease leads to
malabsorption of major nutrients. Most of the alcoholic admitted for
the management of medical problems are found to have evidence of
malnutrition. Anthropometric measurements like Body Mass Index,
Triceps Skin-fold thickness Creatinine/height index are found to be
low in alcoholics. Individuals consuming more than 30 percentage of
total calories as alcohol, significant decreases in protein and fat intake
occurs, and their intake of Vitamin A,C and thiamine is below the
recommended daily allowances. Periods of altered sensorium, Poor
appetite and hangover during intoxication also leads to a reduction
in the amount of food consumed. Various studies have demonstrated
the high incidence of Vitamin deficiency [9].
Thiamine is the vitamin commonly deficient in alcoholics.
This is due to reduced intake as well as reduced absorption of
thiamine. Thiamine deficiency leads to complications like Beriberi
and Wernicke’s Korsakoff’s syndrome. Literature reports that most
consistent reduction was in thiamine followed by folate. Early
symptoms of thiamine deficiency include anorexia, weakness,
itching, burning sensations in hand and feet, indigestion, irritability
and depression [10]. A deficiency in the essential nutrient thiamine
resulting from chronic alcohol consumption is one factor underlying
alcohol induced brain damage. Studies found consistently low total
vitamin B6 in chronic alcoholics. Riboflavin and nicotinic acid were
the next most frequently reduced blood vitamins. Pantothenic acid
and folate were least frequently affected. There were no significant
reduction in folate level of the CSF [11]. Chronic alcohol intake
increases the metabolism of vitamin A and leads to deficiency
features like night blindness. Poor food intake, fat Malabsorption
due to hepatic and pancreatic disease as well as lack of exposure to
sunlight leads to Vitamin D deficiency in alcoholics.
Alcohol induced hepatic dysfunction leads to a reduction in the
production of Vitamin K dependent clotting factors II, VII, IX and
X leading to raised Prothrombine time and bleeding manifestations.
Vitamin E is also found to be low in alcoholics with fat metabolism. Zinc
deficiency found in alcoholics said to be the cause for night blindness
and hypogonadism in alcoholics. Reduction in the concentration of
zinc have been found in liver, Red blood cells and plasma following
chronic ingestion of alcohol [12]. Patients with cirrhosis show that a
greater proportion of zinc was bound to the alpha 2 Macroglobulin
which is metabolically more inert and exaggerate zinc deficiency
[13]. Iron deficiency anaemia often accompany the anaemia of liver
disease [14]. It may be due to poor dietary intake or chronic Gastro
intestinal blood loss either from peptic ulcer or from esophageal or
gastric varices. Alcoholics also prone for Iron deficiency anaemia due
to blood loss resulting from oesophagitis, gastritis, duodenitis and
bleeding esophageal varices [15]. Many studies have documented low
circulating magnesium concentration and a few studies have been
demonstrating reduced tissue levels [16]. Magnesium deficiency may
have pathogenic role in the symptomatology of delirium tremens,
possibly resulting from cell cation bump failure in which magnesium
deficiency plays a integral role [17].
Poorly nourished spirit drinkers are more liable to suffer to folate
dependent megaloblastomas than beer drinkers, since the latter
beverage contains fairly large quantities of folate [18]. The reduction
in alcohol consumption and the restoration of normal diet has been
shown to produce a reticulocytosis and the reversion of the marrow
to normoplastic state.
Stomatocytosis may occur in isolated cases of alcoholics [19].
The stages of anaemia development in alcoholics includes, dietetic
phase, megaloplastic and sideroblastic change [20]. Neutropenia in
alcoholics usually transient. Cell count becomes normal within 24
hours of admission to hospital. A subsequent rebound leukocytosis
has also been noted [21]. The total Granulocyte may be decreased
and this was attributed to folate deficiency. A transient neutropenia,
often with thrombocytopenia reported in non infected alcoholic
patients with only mild hepatic disease [22]. Both lymphocyte
function and macrophage activity are reduced in alcoholics [23].
Acute thrombocytopenia may follow excessive alcohol ingestion
[24]. Thrombocytopenia appears to be due to a direct toxic effect
of ethanol on the magakaryocytes. Thrombocytopenia appears to
alleviate within a week of alcohol withdrawal [25]. In this study we
retrospectively reviewed the studies related to nutritional deficiencies
particularly thiamine deficiency in alcohol dependence syndrome.
Methods and Materials
Forty males aged 20 to 40 years attending the De-addiction
services at National Institute of Mental health and Neuro-sciences,
Bangalore were taken up for this study in the year 2000. In an Average
2-3 patients were recruited every week from the out-patient Screening
Block. All the sample were males who were diagnosed to have Alcohol
Dependence syndrome according to International Classification of
Diseases tenth version Diagnostic Criteria for Research [26].
Subjects having independent medical disorders, independent
psychiatric disorders, other substance use disorders except nicotine
use, malnutrition and subjects having alcohol related psychiatric
disorders were excluded from the study.
All the study subjects were administered a semi-structured
interview proforma including demographic data. Diet history was
assessed by 24 hour recall method. Average daily intake of calories,
protein, fat, carbohydrates, minerals and vitamins were calculated
from the collected diet history. A detailed physical examination was
done by administering Indian Council of Medical Research Score
card. All the subjects were subjected to anthropometric measurements
including weight, height, Mid-Arm Circumference (MAC), Triceps
Skin-fold thickness (TKFT) and Body Mass index (BMI). All the
subjects were subjected to the following Biochemical investigations
before vitamin supplementation;
(a) Hematological parameters
(b) Bio-chemical parameters including fasting blood Sugar,
Serum Bilirubin, Total Protein, Serum Albumin, Serum Glutamte
Oxaloacetae (SGOT), Serum Glutamate Pyruvate Transaminase
(SGPT), Serum Alkaline Phosphatase, Serum Gamma Glutamate
Transferase (GGT), blood Urea, Serum Creatinine.
(c) Fasting Lipidogram
(d) Serum Calcium, Phosphorous, Magnesium, Zinc and Iron
(e) Serum Sodium and Serum Pottasium
All the data were analyzed by using descriptive statistics,
Pearson Correlation Co-efficient, Student’s-t test and multiple linear
regression.
Results
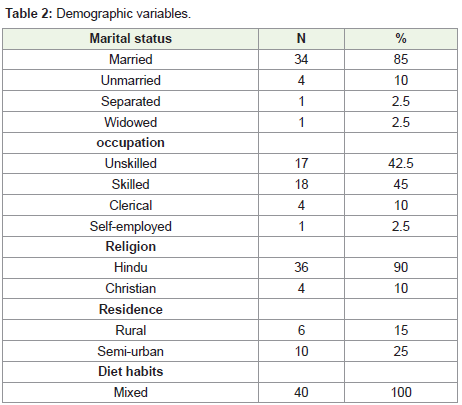
Demographic variables:
All the study sample were men with mean age of 33 years+4.59.
The mean number of education was 7 years and their monthly
income ranged from 600 INR to 6000 INR. Eighty five percentage of
the sample were married. Among the study sample skilled workers
were 45 percentage, unskilled workers were 42.5 percentage. Ninety
percentage of the subjects belong to Hindu religion. Sixty percentage
from the Urban Background. All the sample were 100 percent Non-
Vegetarien (Table 1 and 2).Drinking variables:
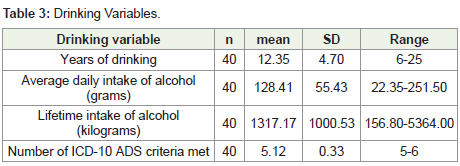
The mean duration of drinking was 12+4.70 years. The mean
daily consumption of alcohol was 128 grams of alcohol. Mean lifetime
consumption of alcohol was calculated as 1317 Kilogram of ethanol.
All the study subjects fulfilled more than five out of six criteria for
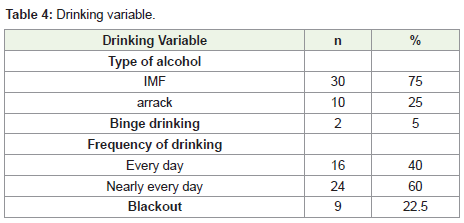
Alcohol dependence syndrome as per ICD-10 DCR. Seventy five
percentage of the subjects have consumed Indian Made Foreign
Liquor (IMFL) like Whisky, Brandy and Rum. The remaining twenty
five percentage of the subjects consumed arrack. The drinking pattern
reveal that 5 percentage of them had binge drinking. Sixty percentage
were smokers.7.5 percentage used Panparag. Thirty percent had a
positive family history of Alcohol Dependence in parents, 15 percent
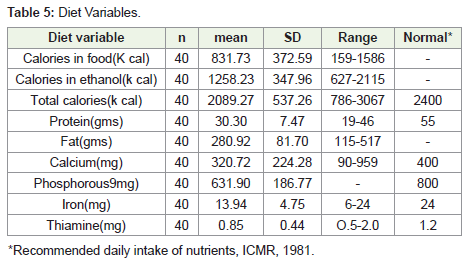
in sibling 2.5 percent in Off-spring (Table 3 and 4).The mean caloric intake was 2089+537.26 which is slightly below
the norms for the average Indian male (2400 Calories). Sixty percent
of the total calories (mean 1258.23+349.960) derived from ethanol.
Only 40 percent from the food intake. Dietary intake also appears
deficient in Protein, Calcium, Iron and Thiamine.
Nutritional variables:
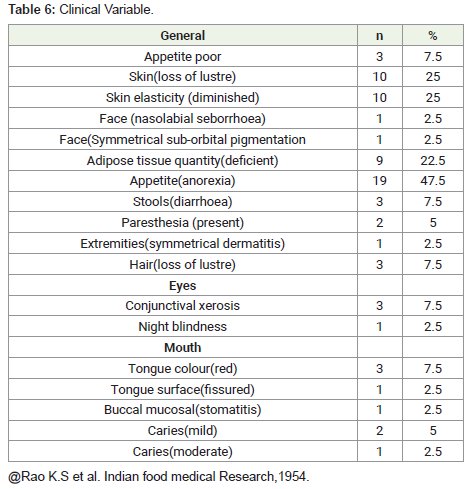
Clinical assessment reveals no evidence of malnutrition in all the
study population. However anorexia was the commonly reported
symptom in 47.5 percent of the study population. The next common
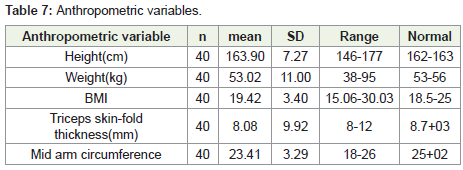
presentation was deficient adipose tissue quantity. The mean Body
Mass Index (BMI) was 19.4 which falls within the normal range of
Indian males (18.5 to 25). The mean anthropometric measures of
Triceps skin fold thickness and mid-arm circumference were within
normal range (Table 5-7).Biochemical variables:
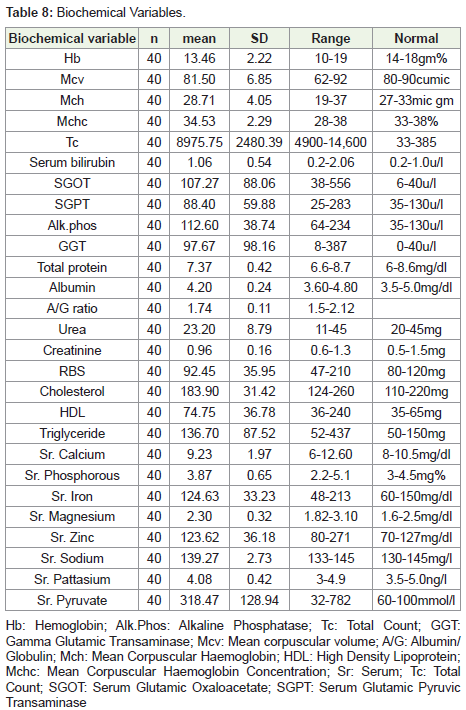
All the study subjects had normal heamogram. Liver function
tests were abnormal as reflected by the elevated liver enzymes.
SGOT/SGPT ratio was 1.2.Serum protein and Albumin Globulin
ratio was in the normal range. Lipid profile showed an increase in
HDL cholesterol. Serum Pyruvate was raised to 318.47 mmol/litre,
(Normal range 0.08 to 0.16 mmol/l) indicating Thiamine deficiency.
All other trace elements were within normal range (Table 8).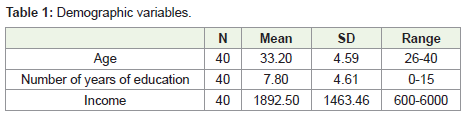
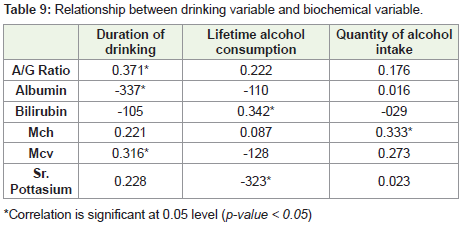
Relationship between drinking variables and biochemical variables:
Duration of drinking is positively correlated with A/G ratio
(P<0.05) and Mean Corpuscular Volume (P<0.05).Life time alcohol
intake is positively correlated with serum bilirubin (P<0.05) (Table 9).Discussion
Chronic alcohol use is known to affect various system in human
body producing Liver function abnormalities, Hematological
abnormalities, Mineral deficiencies and Electrolyte abnormalities. In
this study we aimed to examine the relationship between drinking
variables and nutritional variables in otherwise nutritionally
healthy subjects. Dietary contribution of nutritional deficiency in
alcoholism has been studied. Ethanol is a rich source of Non-nutritive
calories. Heavy drinking is often complicated by malnutrition.
Drinking variables correlated significantly with Liver function tests.
Compromised Liver metabolism could interfere with nutrition,
which in turn may contribute to nutritional deficiency. The mean
total caloric content in this group was below the recommended daily
average intake for an Indian Male. Majority, that is more than sixty
(60%) percent derived from the ethanol, which is essentially known
to produce empty calories. This Observation is comparable with other studies that ethanol may supply more than 50 percent of the dietary
energy [27,28]. The 24 hour dietary intake indicated decreased intake
of other nutrients such as Protein, Phosphorous, Calcium, Iron and
thiamine. Acute alcohol exposure interferes with the absorption
of thiamine from the Gastro intestinal tract at low thiamine
concentration [29]. Biochemical investigations reveal that most of the
nutrients were in normal range except Serum Pyruvate, an indirect
indicator of thiamine deficiency. The Serum Pyruvate this study is
318.47 mmol/L (Normal Value is 0.08 to 0.16mmo/L).Thiamine
is required for the Pyruvate Metabolism. The estimation of Serum Pyruvate level may be of help in suspected Thiamine deficiency. The
symptom of mild thiamine deficiency are vague and can be attributed
to other problems. So the diagnosis of sub clinical thiamine deficiency
is difficult. [30] Mark in 1975 Reported that a useful sign of mild and
moderate thiamine deficiency is Myotactic irritability. Anorexia
is one of the early Symptoms of Sub-clinical thiamine deficiency is
regarded to be a protective phenomenon, since high carbohydrate
diet is a most dangerous in the presence of thiamine deficiency [31].
In this study, anorexia was the most common medical symptom
(47.5%), which correlates with the elevated serum pyruvate level and
indicator of sub-clinical thiamine deficiency.
The most serious complication of thiamine deficiency is damage
to the Central nervous system causing Wernicke’s Korsokoff’s
Syndrome (WKS). That is characterized by the perventricular lesions
including the mamillory bodies, other hypothalamic structures,
periventricular thalamic nuclei and the structures from the floor of
the fourth ventricle [32].
The discrepancy between the 24 hour dietary intake and
biochemical investigation probably suggests that the dietary
deficiencies have not yet resulted in obvious changes in biochemical
measures. This also goes on hand with the observation of normal
clinical assessment of nutrition and anthropometric measurements
in this study sample. Research indicates that the majority of even
the heaviest drinkers have few detectable nutritional deficiencies but
many alcoholics who were hospitalized for medical complications of
alcoholism do experience severe malnutrition [33,34]. This sample is
moderate drinkers with no clinically evident medical complications.
Hence,there is no clinically detectable nutritional deficiencies except
serum pyruvate deficiency. The mean Body Mass Index (BMI) of this
sample is 19.4 which falls within normal range for average Indian
men. Fifty percent of the subjects had anorexia on clinical assessment
which may have contributed for poor dietary intake.
Objective biochemical tests of thiamine status, particularly
measurement of erythrocyte trasketolase activity (ETKA) and the
Thiamine Pyrophosphate Effect (TPPE), provide a sensitive test for
thiamine deficiency where facilities are available [35].
Thiamine is required for Pyruvate metabolism. Increased blood
Pyruvate and Lactate levels can be caused by thiamine deficiency.
The estimation of blood pyruvate can be of help in the diagnosis of
suspected thiamine deficiency. Chronic Wernicke’s Encephalopathy
and korsakoff’s Psychosis may result from episodes of Sub-clinical
thiamine deficiency [36]. The clinician treating for Wernicks
Encephalopathy has a window of opportunity when an adequate
supply of thiamine to the brain can reverse the biochemical lesion
and limit the permanent brain damage [37].
Countries where people normally receive adequate thiamine
from their diet, thiamine deficiency is most commonly caused by
alcoholism. The role of thiamine in the development of Wernicks
korsokoff’s syndrome is supported by reversal of symptoms by giving
thiamine nutrient. Abstinence from alcohol and improved nutrition
have been shown to reverse some of the impairments associated with
thiamine deficiency including improving brain functioning [38]. In
some studies researchers administered thiamine to alcoholic patients and Laboratory animals and found that this treatment reversed some
of the behavioral and metabolic consequences of thiamine deficiency
[39,40]. Researchers also administered different thiamine doses for
two days to a group of alcoholics with no diagnosis of Wernicke’s
korsakoff’s psychosis and tested the participants working memory.
Participants who received highest thiamine dose performed well
on tests of working memory [41]. Some people may exhibit more
subtle neurological symptoms such as abnormalities in a brain region
called cerebellum, inflammation and degeneration of peripheral
nerves as well as changes in behaviour and problems with learning,
memory and decision making. Cerebellum is particularly sensitive to
thiamine deficiency [42]. Accordingly in their countries Wernicke’s
Encephalopathy is primarily found in alcoholics.
The elevated Serum Pyruvate in this study suggests an underlying
Thiamine deficiency. Direct estimation of thiamine would be more
appropriate, since that is more sensitive indicator of Thiamine
deficiency.
Conclusion
This study of Moderate drinkers of Indian male with no clinical
parameters indicating malnutrion reported Reduced Daily intake of
calories than an average that is due to poor diet intake in alcoholics due
to empty calories from ethanol and elevated serum pyruvate which is
an indicator of sub-clinical thiamine deficiency. Also the common
presentation of anorexia in this study, an indicator of sub-clinical
thiamine deficiency improves the validity of sub clinical thiamine
deficiency in this study. Hence, otherwise normal healthy drinkers
both clinically and on routine biochemical evaluation, may have
sub clinical thiamine deficiency. Anorexia also emerged as a clinical
indicator as well as Protector against Wernicke’s Encephalopathy
and Wernicke’s Korsakoff ’s psychosis in this study. Alcohol related
brain damage is reversible if thiamine supplementation is given.
Hence, all the alcohol dependent subjects may benefit from thiamine
supplementation, though they are nutritionally intact to prevent
the precipitation of Wernicke’s Encephalopathy and Wernicke’s
Korsakoff’s Psychosis. Since this observation is cross sectional, more
longitudinal study with direct thiamine estimation will be more
convincing in future. In developing countries all the alcoholics
irrespective of apparent nutritional deficiency may benefit from
thiamine supplementation to prevent alcohol related acute brain
damage.
References
21. Macfarland E, Libre EP (1963) Abnormal leukocyte response in alcoholism.
Ann Intern Med 59: 865-877.
Citation
Shanmugiah A. Thiamine Deficiency in Alcoholics with Normal Body Mass Index. Indian J Nutri. 2019;6(1): 198.