Research Article
Facility Based Management of Children with Severe Acute Malnutrition (SAM): Experience of Child Malnutrition Treatment Centres in Gujarat, India
Rana R*, Vaze G and Maitrak T
Indian Institute of Public Health Gandhinagar (IIPHG), India
Corresponding author: Rana R, Assistant Professor, Indian Institute of Public Health Gandhinagar (IIPHG), Gandhinagar, Gujarat-382042, India, Tel no: +91 7966740713; E-mail: rrana@iiphg.org
Citation: Rana R, Vaze G, Maitrak T. Facility Based Management of Children with Severe Acute Malnutrition (SAM): Experience of Child Malnutrition Treatment Centres in Gujarat, India. Indian J Nutri. 2019;6(1): 197.
Copyright © 2019 Rana R, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 6, Issue: 1
Submission: 22/03/2019; Accepted: 24/04/2019; Published: 29/04/2019
Abstract
Background: In response to high prevalence of severe acute malnutrition, Government of Gujarat in 2012 launched Gujarat State Nutrition Mission; where in a network of nutrition rehabilitation centres across state were established (district and sub-district level). The objective of present analysis is to assess the effect of sub-district level facility based management of children with severe acute malnutrition.
Methods: Retrospective data of 1042 admitted children (April-2014 to March-2015) was retrieved from 12 selected nutrition rehabilitation centres in Gujarat (10% of total nutrition rehabilitation centres, stratified on the basis of sub-district category; normal, priority and high priority). Outcomes studied were average weight gain, survival, defaulter, and recovery rates.
Results: Out of 1042 admitted children, 54% were girls, 56% were infants, 86% belonged to disadvantaged group and 70% were below poverty line. Of the 1042 exits, proportion of children who survived was 100% (acceptable level of care, > 90%) and proportion who defaulted was 4% (acceptable level of care, < 15%). These two are highly positive aspects of the program. Among 96% (1000) discharged children, only 5% recovered (gained ≥ 15% weight gain of initial weight, acceptable level of care, > 75%) with average weight gain of 8.25 (0.7) g/kg body weight/day (acceptable level of care, ≥ 8g/kg body weight/day). Average weight gain among all discharged children was only 3.44 (2.3) g/kg body weight/day which is much less than acceptable level of 8 g/kg body weight/day.
Conclusion: Nutrition rehabilitation centres are effective in providing treatment to children with severe acute malnutrition as demonstrated by acceptable survival and defaulter rates. However, there is need to improve recovery rates and average weight gain.
Keywords:
Child; Severe acute malnutrition; Severe wasting; Management
Abbreviations
SAM: Severe Acute Malnutrition; NFHS: National Family Health Survey; GoG: Government of Gujarat, GSNM: Gujarat State Nutrition Mission; NRC: Nutritional Rehabilitation Centre; CMTC: Child Malnutrition Treatment Centres; INCC: Intensive Nutrition Care Centres; GoI: Government of India; WHO: World Health Organisation; MUAC: Mid-Upper Arm Circumference; IMNCI: Integrated Management of Neonatal and Childhood Illness; EPD: Energy Protein Dense; AWW: Anganwadi Worker; ICDS: Integrated Child Development Scheme; FHW: Female Health Worker; HFW: Health and Family Welfare; CHC: Community Health Centres.
Introduction
Severe Acute Malnutrition (SAM) or severe wasting is widespread in India and children with SAM on an average are 11 times more likely to die than their healthy counterparts [1,2]. Latest National Family Health Survey (NFHS-4) data shows an overall increase in the prevalence of severe wasting from previous survey (NFHS-4: 7.5%, NFHS-3: 6.4%) [3]. In response to high burden, some states initiated high level nutrition mission- such as Gujarat, Jharkhand, Karnataka, Madhya Pradesh, Maharashtra and Uttar Pradesh [1]. In 2012, Government of Gujarat (GoG) launched Gujarat State Nutrition Mission (GSNM) [4], wherein a network of rehabilitation centres across state was established to provide therapeutic treatment to severely wasted children. Despite this, recent data suggests that Gujarat state still has one of the highest (9.5%) incidences of severe wasting [5].
The objective of this study is to assess the effect of sub-district level facility based management of children with SAM in Gujarat state. To manage severely wasted children, Gujarat has a 3-tier system of nutrition rehabilitation centres (district, Nutrition Rehabilitation Centres-NRCs; sub-district, Child Malnutrition Treatment Centres-CMTCs; and village, Intensive Nutrition Care Centres-INCCs) [4]. SAM children with medical complication are first admitted to either district or sub-district level rehabilitative centres (NRCs/CMTCs), after attaining desirable weight gain they are transferred to INCCs, whereas SAM children without medical complication are directly managed at INCCs. Guidelines for SAM management developed by GoG are in line with Government of India (GoI) and World Health Organisation (WHO) guidelines [6-8]. However, there are a few modifications done as per local need; unlike other states where children are discharged from facility-based centres in 14 days, in Gujarat it is 21 days.
Methods
Sample site selection
Rehabilitation centres in Gujarat are being scaled up using need based approach for management of children with SAM, hence planning for centres is done at sub-district level (not so far from villages) and not at district level (quite far from villages). Based on various geographical locations, sub-districts in Gujarat are categorized as normal-plain area, priority-deserted area and high priority-hilly area (N-53, P-118 and HP-77 = 248 total). Total 116 rehabilitation centres are set up across these sub-districts (30-N, 39-P and 47-HP). Among these, 24 out of 116 sub-districts are district headquarters and hence, centres in these 24 sub-districts are treated as district level centres-NRCs and are attached with government medical colleges. For present study from normal, priority and high priority sub-districts, we included 10% (N = 3/30, P = 4/39 and HP = 5/47 = 12 total) sub-district level centres-CMTCs that are usually attached to Community Health Centres (CHCs) as sample sites and excluded 24 district level centres-NRCs (to be studied in next phase).
For this analysis, we retrieved facility based retrospective data of all children (n = 1042) with SAM admitted from 1 April, 2014 to 31, March 2015 to 12 sub-district level centres-CMTC in three different geographical regions (normal, priority and high priority) of Gujarat.
Intervention
Identification and facility based treatment of severe acute malnutrition using locally adapted protocols. The details of treatment protocol are presented in the following sub-section.
Admission: Underweight children referred from community are first admitted to rehabilitation centres on provisional basis by the nutrition assistant. After recording age, weight, length/height, Mid Upper Arm Circumference (MUAC) and presence/absence of oedema and referring admission protocol, identified SAM children are admitted in the rehabilitation centres.
Treatment: At rehabilitation centres, the in-charge medical doctor examines the provisionally admitted children for presence/absence of any medical complications (poor appetite, lethargy, high fever, diarrhoea/severe dehydration, any respiratory distress, and/or severe palmar pallor) using the criteria for the Integrated Management of Neonatal and Childhood Illness (IMNCI) [9]. Finally, children with severe wasting (weight-for-height/length z-scores <- 3SD), and/or MUAC < 115mm, and/or poor appetite, and/or bilateral pitting oedema, and medical complications are admitted for 21 days facility based treatment. These admitted children are fed with locally prepared F-75 therapeutic formula as a substitute of WHO F-75 formulation along with micronutrients and other required medicines as per need. Initial 2 days during stabilization phase, children are fed locally prepared F-75 (starter diet) therapeutic formula every 2 hourly (including night feeds) to correct physiological and metabolic imbalances. Thereafter during rehabilitation phase (2-7 days), these children are given locally prepared F-100 (catch-up diet) therapeutic formula as a substitute for WHO F-100 formulation every four hourly for rapid catch-up growth. After completing 7 days at the centres, children are fed F-100 (catch-up diet) and semi solid (Energy Protein Dense-EPD diet) food alternatively every eight hourly for rapid catch-up growth till day 21.
Discharge: Children are discharged from the rehabilitation centres when they meet the following discharge criteria: (i) target weight gain is achieved (15% weight gain from weight on admission), (ii) no signs of bilateral pitting oedema, and (iii) no medical complication.
Follow up: Before discharge, the nutrition assistant is supposed to share the list/names of children to be discharged with their area specific Anganwadi Worker (AWW) from Integrated Child Development Scheme (ICDS) department and Female Health Worker (FHW) from Health and Family Welfare (HFW) department. Once discharged from the rehabilitation centres, children are to be followed in the community by the ICDS or HFW front-line workers. These frontline workers need to ensure, (i) discharged children are enrolled in the INCCs and are beneficiaries of supplementary nutrition program of ICDS, and (ii) mother is taking the child for regular follow-up visits to rehabilitation centres every 15 days during the 60 days following discharge (i.e. four follow-up visits).
Outcomes
Survival rate, defaulter rate and recovery rate were transcribed from the register of the centre.
Data collection and analysis
We extracted retrospective data maintained in record registers of CMTCs for selected variables. Data was collected in a form and then entered in Microsoft excel 2014. Data cleaning and recoding were done as per need using SPSS version 19. Appropriate statistical tests were used to test the differences in average weight gain. Results are presented as frequencies, percentages and mean (SD). Further, Pearson’s chi-square test was used to measure the association between independent (age, gender, caste, MUAC at admission, socioeconomic status-BPL/APL) and dependent variables (weight gain and recovery rate).
Ethical approval
Ethical approval was obtained from the Institutional Ethics Committee, Indian Institute of Public Health Gandhinagar.
Results
Over a period of one year, 1104 children aged 6-59 months were referred to the selected 12 CMTCs, of which 62 children did not meet the admission criteria (weight for height/length >- 3SD). Out of 1042 admitted SAM children, 564 (54%) were girls and more than half (56%) of the admitted children were infants. Regarding social identity and socio economic status, 896 children (86%) were from scheduled tribes-ST (247), scheduled caste-SC (222), and other backward caste-OBC (427), whereas 731 (70%) children belonged to below poverty line families. Most of the children (83%) were referred by front-line workers of ICDS and HFW department (Table 1). As per the records, none of the admitted children had any medical complications.
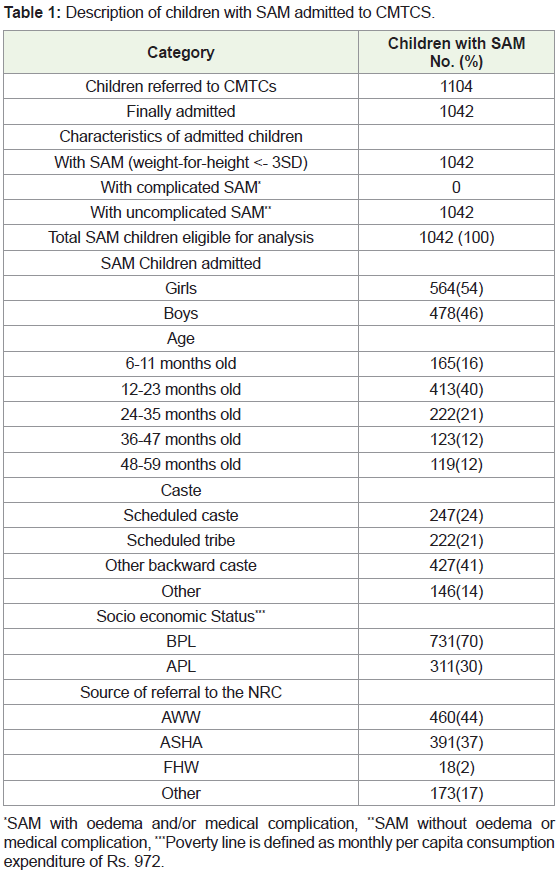
*SAM with oedema and/or medical complication, **SAM without oedema or medical complication, ***Poverty line is defined as monthly per capita consumption expenditure of Rs. 972.
Out of 1042 admitted children, 1000 children were discharged after completion of 21 days therapeutic treatment and 42 children stayed in the CMTCs only till 7th day (defaulted). The following outcomes were recorded among the 1042 children admitted to CMTCs, i) Transfers and deaths: None of the admitted children were transferred to another facility. Also, there were no deaths reported, ii) Defaulters: 42 (4%) children defaulted from the treatment as they left the CMTCs against the advice of staff and iii) Discharged: 1000 (96%) children were discharged from the centres after they completed the facility based treatment at CMTCs for 21 days.
The findings revealed statistically significant association between age of children and weight gain (p = 0.005), age of children and recovery rate (p = 0.002), caste of children and weight gain (p = 0.000), and caste of children and recovery rate (p = 0.000). Further, a multivariable logistic regression analysis indicated that those at higher risk of non-recovery were children belonging to SC/ST/OBC category (adjusted OR: 3.35; 95% CI: 1.8-6.1; p = 0.006) and those with higher weight gain were younger children, 6-23 months old (adjusted OR: 2.77; 95% CI: 1.3-5.6; p = 0.001).
Overall average weight gain among children who were discharged (1000) was 3.44 (2.3) g/kg body weight/day. Average weight gain in normal, priority and high priority areas was 4.05 (2.4), 2.74 (1.9) and 3.64 (2.3) g/kg body weight/day respectively (Table 2). Statistically significant difference in mean weight gain were found between normal and priority areas (p = 0.000), between priority and high priority (p = 0.010) and between high priority and normal areas (p = 0.030). Out of 1000 discharged children, 56 (6%) were recovered (gained ≥ 15% of their admission weight) with an average weight gain of 8.85 (0.7) g/ kg body weight/day; whereas 944 (94%) were not recovered (gained < 15% of their admission weight), with an average weight gain of 3.12 (1.9) g/kg body weight/day.
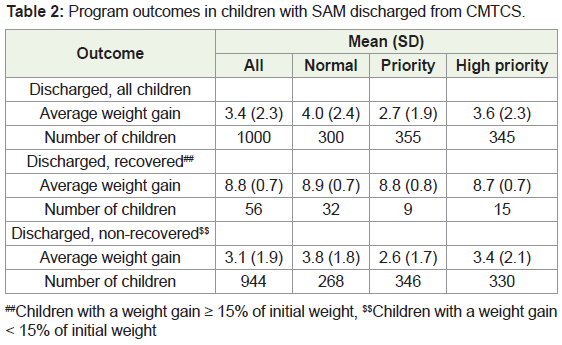
##Children with a weight gain ≥ 15% of initial weight, $$Children with a weight gain < 15% of initial weight
Among the 1000 children who were discharged, 37 children (3.7%) did not gain weight, 749 (74.9%) had poor catch-up growth (< 5 g/kg body weight/day) and only 212 (21.2%) had moderate catch up growth (5-10 g/kg body weight/day). Only 496 (49.6%) of the 1000 discharged children came for all four follow up visits, 772 (77.2%) came back for first three follow up visits, 779 (77.9%) came back for first two follow up visits, 793 (79.3%) came for first follow up visit, whereas 207 (20.7%) did not come for any follow up visit after being discharged. Out of 56 (6%) recovered children, 51 (91.2%) came for first follow up, 49 (87.5%) came for second and third follow up, and only 26 (46.4%) came for fourth follow up.
To sum up, of the total 1042 exits (discharged children), the proportion who survived was 100%, who defaulted was 4% (42), the proportion of children discharged as recovered was 5% (56), whilst the proportion of discharged as non-recovered was 91% (944). Average weight gain after 27 days was 3.44 gm/ per kg body weight/day vs ideal 8 g/ kg body weight/ day.
Discussion
Management of SAM is critical for child survival and subsequent growth. The treatment provided through CMTCs achieved survival outcomes that were comparable with national and international level of care (> 90%). However, overall the average weight gain among discharged children was far below the national and international acceptable level of care (≥ 8 g/kg body weight/day) [6]. In case of recovered children (5%) it was slightly higher than the acceptable national and international level of care. Although, facility based management of SAM is proven to be highly effective in reducing case fatality rates, it is essential for children to complete the treatment. In the selected CMTCs, the proportion of children who defaulted (4%) from the treatment were within international and national acceptable level of care (> 15%) [10]. However, out of total discharged children who completed the treatment (96%), only a minor fraction (5%) were recovered (gained ≥ 15% weight of their admission weight).
Given that this was a record review study, it is unlikely to derive any inferences as to why the recovery rates and average weight gain were below standards despite an acceptable survival and defaulter rate. Possible assumptions for better survival rates could be that as per the records all the admitted children were uncomplicated (without medical complication) SAM and hence they were at relatively lower risk of mortality. Ideally, these children should have been treated in community-based settings or village based rehabilitation centres. The WHO also recommends that uncomplicated SAM children should be treated in the community and facility based centres should be reserved for medically complicated SAM children [11]. However, at present we do not have the facility to provide community based care to SAM children in Gujarat and also, the village based centres are operational in camp based approach. This could be the possible motive for admitting uncomplicated SAM cases to be managed at CMTCs. Similarly, poor recovery and low weight gain together with an acceptable defaulter rate could be due to the reason that many of the admitted children were from nearby catchment areas, they usually go home at night and back in the morning (as reported by CMTC staff), hence skipping the night feeds. As this study could not recognize specific gaps in the locally adopted protocols, further research is needed to study the implementation (such as sincerity of staff, their training in feeding and anthropometry) of facility based SAM management programme, which can provide valuable insights to programme planners.
To our knowledge, this is the first observational study from Gujarat that describes the management of SAM children admitted to sub-district level rehabilitation centres. There are limited observational studies from other states in India; which include Uttar Pradesh (2014), Madhya Pradesh (2013) and Jharkhand (2012). On comparing the outcomes, it was found that survival rates and defaulter rates were better in Gujarat (100%, 4%) than in Uttar Pradesh (98.8% and 47%) [12,13], Madhya Pradesh (99.9 %, 19.8%) and Jharkhand (99.4%, 18%) [14,15]. However, recovery rates and average weight gain were lower in Gujarat (5%, 3.44 g/kg body weight/day) than in Jharkhand (32%, 9.6 g/kg body weight/day), Madhya Pradesh (18.4%, 6.8 g/kg body weight/day) and Uttar Pradesh (24%, 12.1 g/kg body weight/day).
Conclusion
Current study concludes that CMTCs in Gujarat provide lifesaving treatment to children with SAM; however, there is an urgent need to address the below standard recovery rates and average weight gain by addressing the gaps in locally adapted therapeutic feeding protocols.
Acknowledgement
Funding: Authors are thankful to Department of Science and Technology, GoI for funding this study under INSPIRE research grant. Support: Authors are also thankful to Department of Health and Family Welfare, and Department of Women and Child Development, Government of Gujarat for their support in data collection.
References
- Raykar N, Majumdar M, Laxminarayan R, Menon P (2015) India Health Report: Nutrition 2015. Public Health Foundation of India.
- WHO (2014) Global nutrition targets 2025: Policy brief series. World Health Organization, Geneva.
- National Institution for Transforming India. Nourishing India: National Nutrition Strategy. Government of India.
- International Institute for Population Sciences (IIPS) and ICF (2017) National Family Health Survey (NFHS-4), 2015-16: India. Mumbai: IIPS.
- Government of Gujarat (2012) Setting up of Gujarat State Nutrition Mission (GSNM) - Integrated and holistic approach to combat malnutrition in the state. Commissionerate of Health, Government of Gujarat, Gandhinagar.
- (2012) Guidelines on facility based management of malnourished children at Bal Sewa Kendra (CMTC). Commissionerate of Health, Government of Gujarat, Gandhinagar.
- (2011) Operational guidelines on facility based management of children with severe acute malnutrition. Ministry of Health and Family Welfare, Government of India, New Delhi.
- (2003) Guidelines for the inpatient treatment of severely malnourished children. World Health Organization (WHO), Geneva.
- (2009) Operational guidelines for facility based integrated management of neonatal and childhood illness (F-IMNCI). Ministry of Health and Family Welfare, Government of India, New Delhi.
- Sphere Association (2018) The Sphere Handbook: Humanitarian Charter and Minimum Standards in Humanitarian Response (4th edn.).
- WHO (2013) Guideline: Updates on the management of severe acute malnutrition in infants and children. World Health Organization, Geneva.
- Singh K, Badgaiyan N, Ranjan A, Dixit HO, Kaushik A, et al. (2014) Management of children with severe acute malnutrition: experience of Nutrition Rehabilitation Centers in Uttar Pradesh, India. Indian Pediatr 51: 21-25.
- Maurya M, Singh DK, Rai R, Mishra PC, Srivastava A (2014) An experience of facility-based management of severe acute malnutrition in children aged between 6-59 months adopting the World Health Organization recommendations. Indian Pediatr 51: 481-483.
- Aguayo VM, Agarwal V, Agnani M, Das Agrawal D, Bhambhal S, et al. (2013) Integrated program achieves good survival but moderate recovery rates among children with severe acute malnutrition in India. Am J Clin Nutr 98: 1335-1342.
- Aguayo VM, Jacob S, Badgaiyan N, Chandra P, Kumar A, et al. (2014) Providing care for children with severe acute malnutrition in India: new evidence from Jharkhand. Public Health Nutr 17: 206-211.