Research Article
Factors Influencing Exclusive Breastfeeding Up To Six Months of Age in a Rural Community of North 24 Parganas, India
Basu P1*, Chakrabartty A2, Dasgupta U1, Bhattacharyya K1, Ali KM3 and Sarkar AK4
1Department of Community Medicine, Medical College, India
2Health Vision & Research, India
3Department of Nutrition, M.U.C. Women’s College, India
4Department of Health & Family Welfare, Government of West Bengal, India
Corresponding author: Basu P, Department of Community Medicine, Medical College, Kolkata 700073, India, Tel no: +91-9051353396; E-mail: arup.publication@gmail.com
Citation: Basu P, Chakrabartty A, Dasgupta U, Bhattacharyya K, Ali KM, et al. Factors Influencing Exclusive Breastfeeding Up To Six Months of Age in a Rural Community of North 24 Parganas, India. Indian J Nutri. 2018;5(1): 181.
Copyright © 2018 Basu P, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 5, Issue: 1
Submission: 09-02-2018; Accepted: 01-03-2018; Published: 05/03/2018
Abstract
Background: Exclusive Breastfeeding (EBF) means providing only breast milk to an infant. However, oral rehydration solution or medicine can be accepted if prescribed by a qualified doctor. In India, several initiatives were taken to promote EBF among the infants up to six months without getting much promising result. In West Bengal, the rate of EBF up to six months was lower than the national average. It was poorly explained before. Therefore, the study was conducted to estimate the prevalence of EBF in a rural area in West Bengal, India. The study also explored the influencers of EBF practices in the said area.
Methods: It was a community based cross-sectional study conducted in 2016. From the birth register available at the sub-centre, 96 mothers were interviewed face to face. We analyzed data in IBM SPSS 23.0 version. Association between socio-demographic factors and EBF was calculated through Chisquare test and Multivariate logistic regression.
Results: Prevalence of EBF at six months of age was 34.5%. Three factors were found significantly associated with EBF practices at 95% confidence interval. They were - age (p = 0.01), type of family (p = 0.01) and gender of the child (p = 0.05). Important predictors of EBF were age group [p = 0.01; OR: 5.98 (1.78-20.03)] and the type of family [p = 0.02; OR: 0.25 (0.078-0.80)]. Barriers of EBF were caesarean section delivery (37.1%), perception of having insufficient milk (29.0%), ignorance about the importance of EBF (12.9%) and conception during lactation (4.8%).
Conclusion: Factors found to influence EBF in the study can be considered in Infant and Young Child Feeding (IYCF) program in the state.
Keywords:
EBF; Barriers; Prevalence; Socio-demographic characters
Introduction
The World Health Organization (WHO) highly recommended Exclusive Breastfeeding (EBF) of infants up to six months. EBF means feeding only breast milk and nothing else, except for oral rehydration solution or medicine, if prescribed by a qualified doctor. Continuing EBF up to six months is a very simple and cost-effective way to combat malnutrition and to reduce Infant Mortality Rate (IMR) [1-3]. EBF is important for good health and well-being of infants and mothers as well [4]. Children who were not exclusively breastfed for the entire period of six months were prone to suffer from diarrhoea, pneumonia and other morbidities leading to increased mortality [5-7]. Evidence established that non-exclusively breastfed children had more risk of developing atopic eczema [6,8], allergy, asthma, type II diabetes [9], leukaemia and obesity in later part of the life than infants who were exclusively breastfed [4,10].
The government of India developed the Infant and Young Child Feeding (IYCF) guideline in 2004. The guideline emphasized on the promotion of exclusive breastfeeding up to six months [11]. The Government of India’s two flagship programs, the Integrated Child Development Services (ICDS) and the National Rural HealthMission (NRHM) had put in place several interventions. These programs promoted exclusive breastfeeding by preparing the health workforce, mass media campaign, behaviour change communication and sensitizing the community [12]. One of the important desirable outcomes of these two programs was to promote EBF for the children up to six months for the reduction of malnutrition and IMR. Despite several measures, the rates of EBF in India continued to be low [12]. In India, prevalence of EBF was 46.4% in 2005-06 and 54.9% in 2015-2016. The prevalence was 56.0 % in rural and 52.1% in urban area [13]. In spite of many initiatives taken by the Government of India, the rate of EBF was very poor. It was a matter of concern to the policy makers. Any nutrition program like the promotion of EBF; would succeed if we could identify modifiable factors and design a program addressing them. Such program must target individuals, families and resistant communities to achieve optimum breastfeeding behaviors [14].
In West Bengal, the rate if EBF among infants up to six months came down from 58.6 % in 2005-06 to 52.3 % in 2015-16. Compared to the prevalence of EBF in 2005-06, the EBF practices came down by 6.3% in 2015-16 [13,15]. In the District Level Household Survey (DLHS) during 2012-2013, the overall rate of EBF was 48.7% compared to 47.6% in rural areas of North 24 Parganas. This interpreted to the lower rate of EBF in rural area than the urban area [16]. In the National Family Health Survey 4 (NFHS 4) during 2015-2016, the prevalence of EBF was 52.1% in urban compared to 56.0% in rural India. Whereas, in West Bengal, the prevalence of EBF was 61.1% in urban compared to 49.6% in the rural area [13].
Our study area was within the district of North 24 Parganas in West Bengal, India. North 24 Parganas had around 10 million populations in 2011 [13]. North 24 Parganas had very close similarity to the overall picture of the state of West Bengal in 2011 with respect to certain demographic characteristics like the level of literacy, sex ratio, per capita income and scheduled caste/tribe population. Compared to India, causes of higher urban and rural difference (rural much lower than urban) remained under-researched in West Bengal. The present community based study was conducted in a rural area in North 24 Parganas to estimate the prevalence of EBF practices among the infants up to six months. The study also explored the influencers of EBF practices in the said area.
Materials and Methods
Design and setting of the study
This was a community-based cross-sectional study conducted in the catchment area under the Banspool public health sub-centre of North 24 Parganas. All three villages under this sub-centre (Banspool, Iswarigacha and Birpur) were covered under this study. In India, one sub-centre (the lowermost public health institution) usually covers a population of 5,000. However, the sub-centre under this study had a population of 6,120 in 2011.
Study period and sampling
The study period was from 1st April to 30th June 2016. Eligible respondents were all mothers having their children born within the period from 1st October 2014 to 30th September 2015. Therefore, the age of the children was between 6 months to 21 months. Based on the existing prevalence of EBF (64.1%) in North 24 Parganas; required sample size was 96 (with 15% relative error). During the period, there were 111 births under the sub-centre as found out from the birth register available at the sub centre. From the list of these 111 mothers, the interview was conducted from the beginning of the birth register. We continued till we reached a sample size of 96.
Data collection
A trained doctor interviewed 96 mothers at the household level having a child of 6 to 21 months. The interviewer used a predesigned, pretested and semi-structured questionnaire. The accompanying health worker provided a good introduction for rapport building. The interviewer first explained to the respondent, the purpose of the study and then read out the consent form. Thereafter, the interviewer took written consent. There were two married women below 18 years. For these two respondents, husbands also provided written consents.
Exclusive breastfeeding (operational definition under the study)
In our study, EBF meant providing only breast milk, not even water. However, medicine or oral rehydration solution was accepted, if it was prescribed by a qualified doctor. The interviewer retrospectively collected information about EBF among children of 6 to 21 months and its duration in months.
Measures
From the mothers, information about breastfeeding was collected using different questions. First, a mother was asked if the child was ever breastfed. Mother, who responded “no”, was coded as “Nonbreastfed”. Mother, who reported “yes”, was coded as “Breastfed”. Mothers, who had reported breastfeeding their children, they were asked for how many months they depended only on breast milk. They were probed if the child was provided other food supplements or even sips of water during breastfeeding till six months (except for medicine or oral rehydration solution if prescribed by a qualified doctor). Among them, who reported that they only depended on breast milk (exclusively) and nothing else, such breastfeeding was coded as “EBF”.
Duration of EBF was indicated in months. The proportion of mother continuing such EBF was calculated to estimate the prevalence of EBF for one month, two months and so on, up to the period of six months and more.
The interviewer asked mothers who did not provide EBF up to the age of six months. They also asked what were the most important reasons for non-EBF. The respondent picked up the most important reason suitable for her from the list of reasons stated in the questionnaire.
Data analysis
In the study, the independent variables were socio-demographic characteristics of the mother like age, religion, literacy, occupation, the income of the family, type of the family, sex of the child and number of children.
We measured socio-demographic characteristics of mothers. For this, we considered some basic demographic characters. They were age in completed years, religion - Hindu/Muslim or other and literacy - illiterate (cannot read and write) or literate. We also considered economic factors like employment status - employed or housewife and monthly income of the family in INR (Rs). Some factors were related to the family characters like the type of the family - joint (two families shared the common source of food) or nuclear, sex of child under the survey- male or female and number of children of the respondent mother.
For the age, monthly income and number of children; questions were open-ended and for rest of the items, questions were closedended. Age was categorized into two groups - up to 24 years (age group up to youth) and above 24 years. Monthly income was classified into two groups - up to INR 3046/month (BG Prasad Scale Class IV, December 2016 and above it (>INR 3016 per month). The number of children was grouped as - single child or more.
The dependent variable was exclusive breastfeeding up to six months of the infant (EBF or non-EBF). Duration of EBF was categorized in to one month, two months and so on up to the age of six months and more.
In the results section of the manuscript, we have provided key findings in row percentages for better understanding of the distribution of EBF for different factors. However, in the tables, we have provided column percentages.
We used multivariate logistic regression model to identify the most important predictor of EBF at the confidence interval of 95%. Hsieh estimated the required sample size for Multivariate logistic regression. Considering the estimated prevalence of EBF as 34.5%, expected Odds Ratio 3.0 and multiple correlation coefficient 0.7; required sample size for Multivariate logistic regression was 82 [17]. Our sample size was 96.
We used SPSS 23.0 version to analyze the dataset of 96 respondents. We performed bivariate analysis using Chi-square test at the confidence interval of 95%. P values of =< 0. 05 were considered to be significant.
Limitation of the study
The NFHS 4 in West Bengal during 2015-2016 measured the rate of EBF for last six months using 24 hour recall method [13,18]. Based on the population of the sub-centre area and the birth rate, the estimated child up to the age of six months would be around 55 in a certain point of time. We had a sample size requirement of 96. Therefore, we decided to select only the mothers who delivered during the period from 1st October 2014 to 30th September 2015. Our study retrospectively collected EBF information of the children of 6 to 21 months from their mothers. During the period of the interview, none of the children was less than six months. So, we did not follow 24 hour recall method like many other studies. Following the definition of EBF as per WHO, we estimated the rate of EBF for different duration of months like one month, two months and so on up to six months or more. We had a known limitation of recall bias. Our study was also limited to a single sub-centre area and therefore, could not capture wider socio-demographic variations.
Results
Socio-demographic characteristics
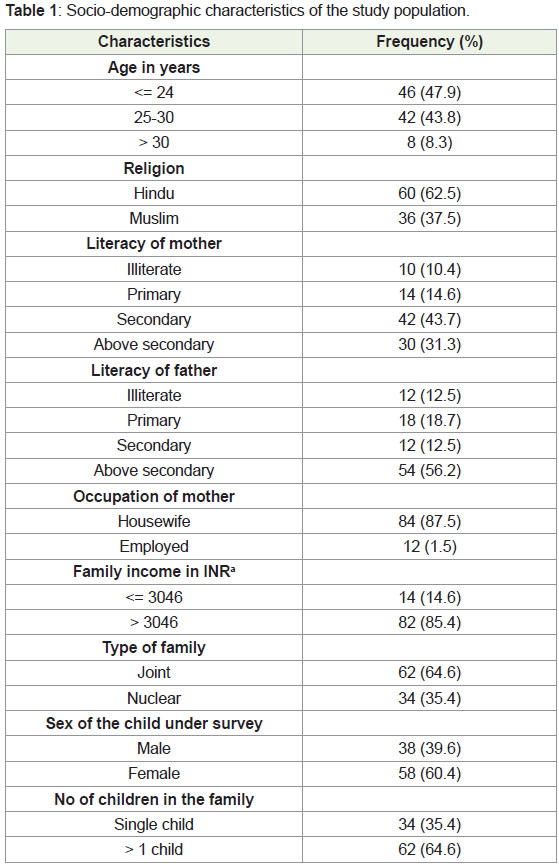
In the study, 96 mothers participated. Mean age of the mothers was 24.9 years (24.9 ± standard deviation, 3.6). Among 96 mothers, a majority of the mothers belonged to the age group below 24 years (47.9%). The next major age group belonged to 25-30 years (43.8%). Among the respondents, 62.5% mothers were Hindus and 37.5% were Muslims. Around 10.4% mothers were illiterate. Mothers below the BG Prasad socio-economic scale (= < INR 3046 per month) counted 14.6%. The average income of the family per month was INR 5656.2 (5656.2 ± standard deviation, 3294.3). Further details are provided in the Table 1.
Prevalence of Exclusive Breastfeeding (EBF)
In the study, 34 (35.4%) mothers had exclusively breastfed their children at least for six months. Mean duration of EBF with only breast milk was around 95 days (95 ± 11. 8, standard deviation; Range: 7-189 days). Around 62 mothers (64.6%) did not complete EBF for the said duration. Among these 62 mothers, only 19.8% mothers continued EBF for at least one month and thereafter they discontinued. Our study could find out the proportion of mothers who continued EBF for one month, two months and so on up to the age of six months and more (Figure 1).

aEBF (Exclusive Breastfeeding): EBF means feeding only breast milk, nothing else, not even water, except for medicine and or oral rehydration solution, if prescribed by a registered doctor.
• The above figure shows the proportion of mother continuing EBF for one month, two months and so on up to the age of six months and more.
Factors influencing exclusive breastfeeding
Factors like age, religion, literacy, occupation, the income of the family, type of the family, sex of the child and number of children were explored in this study. Among 46 women of younger age group (<= 24 years), 64.7% provided EBF up to the age of six months. Whereas, among mothers of higher age group (>= 25 years), the rate was 24.0%. Among Hindus, 36.6% and among Muslims, 33.3% mothers provided EBF. Mothers with lower literacy level (up to the primary) had lower EBF rate (25.0%) than mothers with higher literacy rates (38.8%). Compliance of EBF was 14.3% among the lower income group compared to 39.0% among the higher income group. Women from nuclear families practised EBF in 47.1% cases compared to 29.0% in joint families. Among 38 male children, 36.8% children were put on EBF and whereas, among 58 female children, 34.5% were put on EBF. Mothers with a single child provided EBF in 70.6% cases compared to 16.1% among mothers with more than one child (Table 2).
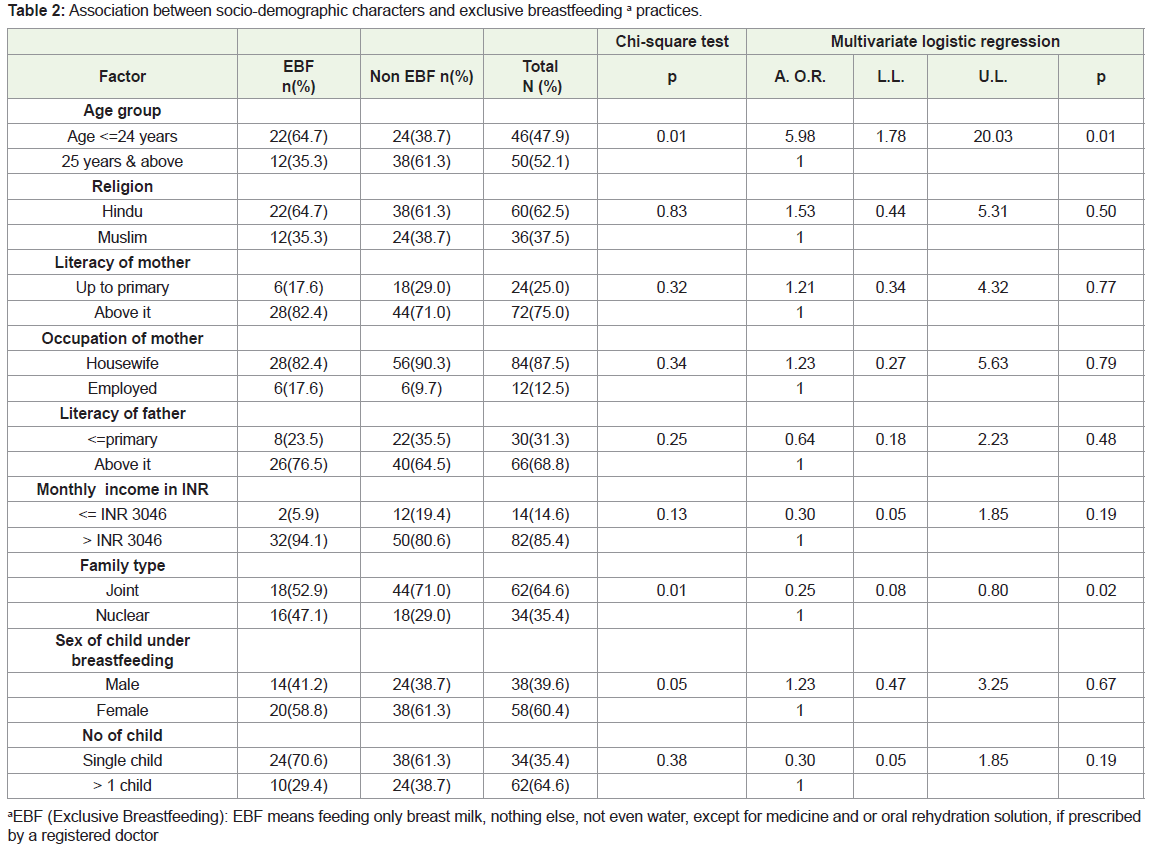
The study explored important barriers among 62 mothers (64.6%) who had not provided EBF to their children up to six months of their age. Among these barriers, most important was caesarean section delivery (37.1%). The next important barrier was the perception of having insufficient milk secretion (29.0%). Out of these 62 mothers, 12.9% mothers had ignorance about the importance of EBF. Around 4.8% conceived during lactation.
Using the Chi - square test, three factors were found significantly associated with the EBF. They were age of the mother (p = 0.01), type of the family (p = 0.01) and sex of the child (p = 0.05). The multivariate logistic regression analysis identified two important predictors of EBF. They were age group [p = 0.004; OR: 5.979 (1.785-20.031)] and the type of family [p = 0.020; OR: 0.251 (0.079-0.803)] (Table 2).
Discussion
In our study, the rate of exclusive breastfeeding up to six months was 34.5%, whereas it was 47.6% in the rural areas of the same district during 2012-2013 [16]. In a community based study in 2008, conducted in Bankura, West Bengal, the prevalence of EBF was 57.1% [19]. Another study in South India reported 27% EBF in 2015 [20]. In Bangladesh, situated nearby North 24 Parganas, the rate of EBF in Mirzapur was 36% in 2011. The rate was lower than the national average of 64% in Bangladesh [21]. The prevalence of EBF in our study conducted in 2016 was 13.1% less compared to the district average during 2012-2013 [16]. The rate was also 7.8% less than the state average of 52.3% during 2015-2016 [13]. In India, using the NFHS 4 questionnaire, women were asked several questions about the duration of any breastfeeding, and infant feeding in the previous 24 hours [18]. At the age of six months, NFHS 4 measured rate of the EBF using 24 hour recall method. This was not out of limitation [13]. Agampodi, et al. showed that actual exclusive breastfeeding rates were lower than those derived from the 24 hour recall method [22]. We strictly adhered to the definition of EBF as per the WHO guidelines and retrospectively estimated the rate of EBF for one month, two months and so on up to six months and more, with a known limitation of recall bias [1,2]. However, the findings were very close to some other findings of studies conducted surrounding the geographical areas of our study during similar periods. Our finding was quite lower than the NFHS 4 report conducted during the same period. So, it raised a question on the accuracy of the information collected through NFHS or DLHS using 24 hour recall method. In the 24 hour recall method used in NFHS 4, there was a possibility of a higher rate of reporting. The 24 hour recall method was a proxy indicator towards the actual estimation of EBF. Only correct information could properly help for planning a program, for example, IYCF or Reproductive and Child Health (RCH) program of the state. We, therefore, needed more accurate information on EBF. The most accurate way to estimate the actual exclusive breastfeeding rate is to through a prospective cohort study of newborn babies for up to 6 months of age. Our study, therefore, gives a justification to go for a prospective cohort study to measure the accurate rate of EBF among the newborns till their age of six months.
We identified three important influencers of EBF. They were sex of the child (male or female), type of family (joint and nuclear) and age group (younger age group <= 24 years and elder group >= 24 years). Out of these three, multivariate logistic regression analysis identified two factors (age and type of the family) to be important predictors of EBF.
First, we have discussed about the role of the gender. The gender discrimination still prevailed in the study area. Among 38 male children, 36.8% were put on EBF. Among 58 female children, 34.5% were put on EBF. Gender as a social issue influenced adherence to initiation of EBF and its continuation in a study in Haryana in India [23]. In Chandigarh, male gender was found as a risk factor for pre-lacteal feeding and delayed initiation (beyond the first hour) of breastfeeding [24]. If the newborn was a girl, the mother either refused to feed the baby immediately or reacted reluctantly. Gender preference affected not only the female baby, but also the male baby. Because of son preference, the family followed all rituals in case of a boy baby that ultimately delayed the timely start of breastfeeding [25]. Exclusive breastfeeding was practised among overall 52.5% children, and whereas, 41.5% among boys and 27.1% among girls up to six months. The gender difference was statistically significant [26]. The Child Disparity Index in India with respect to the breastfeeding was 0.040, 0.041, 0.042 in NFHS 1, NFHS 2, NFHS 3 respectively [27]. Any effective healthcare program for mother and child had to focus on preparing their health workforce so that gender disparity did not prevail. Birth preparedness by the health workers and community health volunteers showed the positive impact of the breastfeeding practices [27,28]. Even though the gender difference was not high in our study, it was indicative that the difference prevails. If the study area could have been wider, more concrete conclusions could have been made. In West Bengal, the present study findings recommend for sensitization of health workforce so that promotional activities are carried out among mothers and family members are sensitized about the importance of EBF for both male and female children.
In our study, mothers from nuclear family (47.1%) were more likely to give EBF to children than the mothers from the joint family (29.0%). In a study in Lyon and in the Paris in 2015, it was found that the family environment, especially the husband, appeared to have the greatest influence on the EBF decision [29]. The nuclear family had a higher rate of EBF than the joint family in our study and being revealed out as an important predictor [p = 0.02; OR: 0.25 (0.08-0.80)]. The encouragement from other family members was also associated with higher breastfeeding initiation rates [29]. In our study in a joint family, the rate of EBF was lower. In other words, the influence of family members was negative to EBF. Support from fathers in supporting the initiation and continuation of breastfeeding was recognized [30]. From the joint family perspectives, more research was needed to fully understand the matter and even the relationship between the father and mother in connection with the EBF [31,32]. Our study opened an opportunity to further research; why in a joint family rate of EBF was lower.
In our study, the age of the mother was an important predictor of EBF. Younger mothers up to 24 years were more likely (64.7%) to complete EBF till six months than the elder mothers (29.0%) [p = 0.01; OR: 5.98 (1.78-20.03)]. Zielinska in his study in 2017 found that non-exclusive breastfeeding was associated with maternal age under 20 years. Maternal age from 26 to 30 years had a very high chance of compliance with EBF [33]. In our study, we got similar observations. For younger mothers, they might have less exposure to health promotion activities and had poor knowledge as well. Poor knowledge about the benefit of EBF had detrimental effects on the compliance to EBF [33]. Our study, therefore, recommends adequate promotional activities among mothers of all age groups with focus on the younger age group.
Apart from the above three influencers of the EBF, we have discussed above, in our study, we identified important barriers of EBF those were mentioned by the lactating mothers from their own experiences. Two most important barriers were caesarean section delivery (37.1%) and the perception of having insufficient milk secretion (29.0%). In a tertiary care hospital in Haryana, major barriers to the initiation of breastfeeding were obstetric complications leading to caesarean section and neonatal complications [23]. In another study in Chandigarh in India, caesarean section was found to be a leading barrier of EBF [24]. Unlike other studies, one important barrier that could not be identified in our study was neonatal complications. However, our study identified a new barrier, the perception of having insufficient milk secretion. This finding could contribute to the planning of health education among the mothers and training of health workers.
Conclusion
The prevalence of exclusive breastfeeding up to the age of six months in our study area was 34.5%. Important factors to influence EBF were age, type of family (joint or nuclear) and gender of the child. Important barriers of EBF were caesarean section delivery and perception of having insufficient milk secretion. Some of these factors can be incorporated into IYCF program of the health department to increase the rate of exclusive breastfeeding. A cohort study may be conducted among the mothers to estimate the actual prevalence of EBF. The same study can also explore the barriers of EBF to avoid limitations of 24 hour recall method or the retrospective method we adopted in this study.
Acknowledgement
This study is part of an academic work under MD (Community Medicine) of Medical College, Kolkata; West Bengal University of Health Sciences. We wholeheartedly thank all faculties of Medical College, Kolkata for their support. We sincerely extend thanks to all mothers who participated in the study.
References
- WHO (2007) Indicators for assessing infant and young child feeding practices part 1 definition. Dept of Child and Adolescent Health and Development pp: 1-19.
- WHO (2015) Up to what age can a baby stay well nourished by just being breastfed?
- WHO (2009) Infant and young child feeding: model chapter for textbooks for medical students and allied health professionals. Geneva: World Health Organization.
- Kramer MS (2010) “Breast is best”: the evidence. Early Hum Dev 86: 729-732.
- Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS, et al. (2003) How many child deaths can we prevent this year? Lancet 362: 65-71.
- Ip S, Chung M, Raman G, Trikalinos TA, Lau J (2009) A summary of the agency for healthcare research and quality’s evidence report on breastfeeding in developed countries. Breastfeed Med 4: S17-S30.
- Kramer MS, Guo T, Platt RW, Sevkovskaya Z, Dzikovich I, et al. (2003) Infant growth and health outcomes associated with 3 compared with 6 months of exclusive breastfeeding. Am J Clin Nutr 78: 291-295.
- Kramer MS, Chalmers B, Hodnett ED, Sevkovskaya Z, Dzikovich I, et al. (2001) Promotion of breastfeeding intervention trial (PROBIT): a randomized trial in the republic of Belarus. JAMA 285: 413-420.
- Pettitt DJ, Forman MR, Hanson RL, Knowler WC, Bennett PH (1997) Breastfeeding and incidence of non-insulin-dependent diabetes mellitus in pima Indians. Lancet 350:166-168.
- Jones ME, Swerdlow AJ, Gill LE, Goldacre MJ (1998) Pre-natal and early life risk factors for childhood onset diabetes mellitus: a record linkage study. Int J Epidemiol 27: 444-449.
- (2006) Ministry of Women and Child Development, Government of India. National Guidelines on Infant and Young Child Feeding (IYCF).
- Dadhich JP, Agarwal RK (2009) Mainstreaming early and exclusive breastfeeding for improving child survival. Indian Pediatr 46: 11-17.
- (2016) National Family Health Survey (NFHS 4), 2015-2016: India. V. I. Mumbai: International Institute for Population Sciences pp: 4.
- Chandhiok N, Singh KhJ, Sahu D, Singh L, Pandey A (2015) Changes in exclusive breastfeeding practices and its determinants in India, 1992-2006: analysis of national survey data. Int Breastfeed J 10: 34.
- International Institute for Population Sciences (2006) National Family Health Survey (NFHS 3), 2005-06: India 1: 4.
- Mumbai: International Institute for Population Sciences (2016) District Level Household and Facility Survey (DLHS 4), North 24 Parganas, 2015-16: India 1: 5-14.
- Hsieh FY (1989) Sample size table for logistic regression. Stat Med 8: 795-802.
- (2017) International Institute for Population Sciences. National Family Health Survey (NFHS), Women’s Questionnaire, 2015-2016.
- Sinhababu A, Mukhopadhyay DK, Panja TK, Saren AB, Mandal NK, et al. (2010) Infant and young child-feeding practices in Bankura district, West Bengal, India. J Health Popul Nutr 28: 294-299.
- Vijayalakshmi P, Susheela T, Mythili D (2015) Knowledge, attitudes, and breastfeeding practices of postnatal mothers: A cross sectional survey. Int J Health Sci (Qassim) 9: 364-374.
- Joshi PC, Angdembe MR, Das SK, Ahmed S, Faruque ASG, et al. (2014) Prevalence of exclusive breastfeeding and associated factors among mothers in rural Bangladesh: a cross-sectional study. Int Breastfeed J 9: 7.
- Agampodi SB, Agampodi TC, Piyaseeli UK (2007) Breastfeeding practices in a public health field practice area in Sri Lanka: a survival analysis. Int Breastfeed J 2: 13.
- Majra JP, Silan VK (2016) Barriers to early initiation and continuation of breastfeeding in a tertiary care institute of Haryana: A qualitative study in nursing care providers. J Clin Diagn Res 10: LC16-LC20.
- Raghavan V, Bharti B, Kumar P, Mukhopadhyay K, Dhaliwal L (2014) First hour initiation of breastfeeding and exclusive breastfeeding at six weeks: prevalence and predictors in a tertiary care setting. Indian J Pediatr 81: 743-750.
- Angadi MM, Jawaregowda SK (2015) Gender discrimination in relation to breast feeding practices in rural areas of Bijapur district, Karnataka. Int J Contemp Pediatr 2: 340-344.
- Sharma RK, Rani M, Sharma SK (2010) Gender inequality in child care in India: is it narrowing down. Annual Meeting at PAA.
- Ladomenou F, Kafatos A, Galanakis E (2007) Risk factors related to intention to breastfeed, early weaning and suboptimal duration of breastfeeding. Acta Paediatr 96: 1441-1444.
- Laroia N, Sharma D (2006) The religious and cultural bases for breastfeeding practices among the Hindus. Breastfeed Med 1: 94-98.
- Otmani C, Ibanez G, Chastang J, Hommey N, Cadwallader JS, et al. (2015) Role of the mother's family environment in the initiation of breastfeeding. Sante Publique 27: 785-795.
- Rempel LA, Rempel JK (2011) The breastfeeding team: the role of involved fathers in the breastfeeding family. J Hum Lact 27: 115-121.
- Cox MJ, Paley B (1997) Families as systems. Annu Rev Psychol 48: 243-267.
- Waletzky LR (1979) Husbands' problems with breast-feeding. Am J Orthopsychiatry 49: 349-352.
- Zielinska MA, Hamulka J (2017) Reasons of non-exclusive breast-feeding to infants within the first 6 months. Pediatr Int.