Research Article
Retrospective Analysis of Vitamin D Levels in Office Going People in South India
Chetty S* and Ravishankar AC
Department of Medical Affairs, Mylan Pharmaceuticals Private Limited, India
Corresponding author: Chetty S, Department of Medical Affairs, Mylan Pharmaceuticals Private Limited, Bangalore, India, E-mail: Shashikanth.chetty@mylan.com
Citation: Chetty S, Ravishankar AC. Retrospective Analysis of Vitamin D Levels in Office Going People in South India. Indian J Nutri. 2018;5(1): 180.
Copyright © 2018 Chetty S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 5, Issue: 1
Submission: 08/12/2017; Accepted: 09/02/2018; Published: 12/02/2018
Abstract
Background & objectives: Vitamin D is a sunshine vitamin and is one of the fat-soluble vitamins. Vitamin D regulates the absorption of calcium from the small intestine. Though sunshine is abundant in India, there is widespread prevalence of varying degrees (50-90%) of Vitamin D deficiency among Indians. This study was conducted to evaluate the status of the Vitamin D in office going people who get very little opportunity to expose to mid-day sun light.
Methods: This is a retrospective analysis of Vitamin D data, collected from employees of the corporate offices and manufacturing plant in Bangalore. Venous blood samples were collected in the month of August and Vitamin D 2 was measured using Chemiluminescence method.
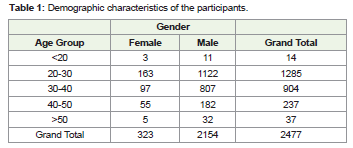
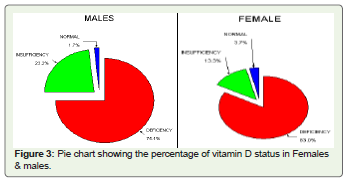
Results: A total of 2477 subjects’ vitamin D data were evaluated. Among them 2154 were men and 323 were women. More than 83% of women and 75% of men were deficient in Vitamin D levels. Only 1.7% of men and 3.7% of women had normal Vitamin D levels and remaining had insufficient levels.
Interpretation & conclusions: Office going people have minimal time to expose themselves to sunlight and hence are more prone for sunshine vitamin deficiency. The study clearly brings forth the importance of exposure to sunlight, periodic Vitamin D screening, strategies for the prevention of Vitamin D deficiency like food fortification with vitamin D and Vitamin D supplements.
Keywords:
Vitamin D; Sunlight; Men; Women; Fortification of foods; India
Introduction
Vitamin D is a sunshine vitamin and is one of the fat-soluble vitamins. Vitamin D regulates the absorption of calcium from the small intestine. It coordinates with parathyroid hormone for bone mineralization and maintains serum calcium levels in the blood stream. Recently, many epidemiologic studies have implicated that vitamin D has a role in inflammation, immune modulation and has effect on cytokine levels [1-3].
The 1,25-dihydroxyvitamin D3 (calcitriol) is the biologically active form of Vitamin D whereas 25-hydroxyvitamin D (25OHD) is the major circulating metabolite. The later one is the most reliable indicator for the Vitamin D status of an individual as its production is not regulated and the serum concentration indicates both absorption from diet as well as cutaneous synthesis [4].
More than 30 ng/ml of 25OHD is normal Vitamin D status, less than 20 ng/ml is considered as Vitamin D deficiency and 25OHD status between 20 and 30 ng/ml is taken as vitamin D insufficiency [5].
The deficiency is associated with osseous changes such as rickets/osteomalacia and the insufficiency is linked with secondary hyperparathyroidism and negative skeletal consequences [6]. In addition to Vitamin D deficiency, lower intake of calcium multiplies the parathyroid response to vitamin D insufficiency. The secondary hyperparathyroidism mobilizes mineral and matrix from the bones leading to increased bone loss and to a high risk of fracture and, low peak bone mass in children [7,8]. Vitamin D is also linked to inflammatory and lifestyle-related chronic disorders like diabetes, cardiovascular diseases, auto-immune disorders, depression, and some cancers [9].
Vitamin D deficiency is endemic and prevalent in all age groups including children, adolescents and adults [10]. About 1 billion people worldwide have Vitamin D deficiency or insufficiency [11]. Though sunshine is abundant in India, there is widespread prevalence of varying degrees (50- 90%) of Vitamin D deficiency among Indians [12,13].
A number of reasons have been attributed for the high prevalence of vitamin D deficiency like limited exposure to sunlight, skin complexion, vegetarian food habits, lack of fortification of staple foods and not aware of Vitamin D supplements and issues with affordability and increasing pollution.
This study was conducted to evaluate the status of the Vitamin D in office going people who get very little opportunity to expose to mid-day sun light. As far as our knowledge goes this is first of kind study in office going people in south India.
Materials and Methods
This is a retrospective analysis of Vitamin D data. The data obtained after the Vitamin D screening program where the employees of the corporate offices and manufacturing plant in Bangalore had participated. The employees included both male and female of age from 20 years to 60 years. Most of the employees were indoor workers. Hardly any staff would be going outside the building premises and expose to sunlight during the working hours i.e., 09:00 AM to 06:00 PM. The dress code of the staff is formal wear.
Venous blood samples of the employees were collected in the month of August during the day time between 11:00 AM and 05:00 PM. The blood samples were collected in the spray-coated lithium heparin tubes. The samples collected were taken to the central lab for the measurement of Vitamin D2. Samples processed in these tubes are used for plasma determinations of Vitamin D2. The method adopted for measuring Vitamin D2 was Chemiluminescence method.
The standard or biological references used were less than 20 ng/ml as deficient, 20 to 30 ng/ml as insufficient, between 30 and 100 ng/ml as sufficient and more than 100 ng/ml as toxicity.
Results
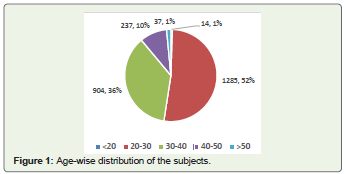
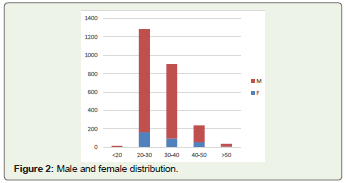
A total of 2477 subjects’ vitamin D data were evaluated for analysis. Among the 2477 participants, 2154 were men and 323 were women (Tables 1,2). Majority of the employees were aged between 20 and 30 years of age (52%), followed by subjects aged between 30 and 40 years (36%), and between 40 and 50 years (Figure 1 ). Distribution of males and females are depicted in (Figure 2).
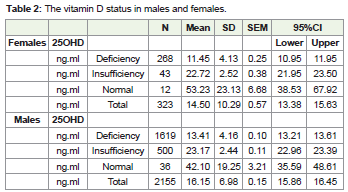
Out of 323 females, 268 (83%) were deficient and 43 women were insufficient and only 3.7 % were sufficient. A higher percentage of women (83%) were deficient in Vitamin D levels compared to men (75.1%). However, more number of men (23.2%) were insufficient for Vitamin D than the women (13.3%) (Figure 3).
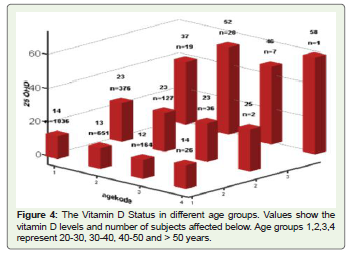
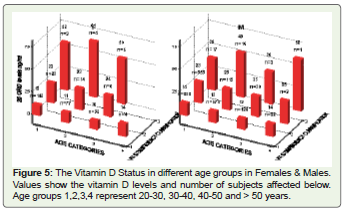
In the age group of 20 to 30 years, 1036 (72%) were deficient and 376 (26.2%) were insufficient and only 19 (1.5%) were having sufficient vitamin D levels. In the age group of 30 to 40 years, 651 (80.7%) were deficient and 127 (15.7%) were insufficient and the remaining 28 (3.5%) were sufficient. In the age group of 40 to 50 years, only 7 employees were having sufficient levels and 164 (79.2%) and 36 (17%) were deficient and insufficient respectively. In the population, more than 50 years’ age only 1 subject had sufficient levels of Vitamin D levels and the remaining 89.6% were deficient and others were insufficient (Figures 4,5).
Discussion
Over the decades it is clear that Vitamin D serves multiple functions. Its critical role in reducing the risk of cancer, multiple sclerosis and type 1 diabetes mellitus is being explored, over and above the established role in calcium absorption and metabolism for bone health. Maternal vitamin D is critical for the proper development of fetus and its tooth.
In our study, we wanted to analyze the Vitamin D levels in normal healthy office going people and know how many would be deficient, as they get minimum time for sun exposure.
India is a tropical country extending from large 8.4°N latitude to 37.6°N latitude. The larger part of the Indian population lives in areas where ample sunlight is received. Contrary to the belief, India is a Vitamin D deficient nation. In North India (27°N), 96% of neonates, 91% of healthy school girls, 78% of healthy hospital staff and 84% of pregnant women were found to have hypovitaminosis D. In South India (13°N), hypovitaminosis D is equally prevalent among different population groups [12,14,15].
In a study by Goswami R, et al. conducted on healthy subjects in Delhi who differed with respect to variables relevant to vitamin D and bone mineral metabolic status, such as direct sunlight exposure, season of measurement, skin pigmentation, etc [16]. The results show that the groups which had significantly lower exposure to sunlight and the group with depigmentation had significantly lower 25(OH)D concentrations. The groups which had lower sunlight exposure when restudied in summer had significantly higher 25(OH)D concentrations than in the winter, suggesting sunlight exposure playing very vital role in synthesis of Vitamin D.
In another study by Vu LH, et al. conducted in office workers of Australia, a subtropical climate zone, show the difference in serum levels of 25(OH)D concentrations in summer and winter [17]. The results reveal that in summer, 14% of participants were classed as “insufficient”, compared with 51% in winter. In this study, high 25(OH)D levels in summer were associated with time spent outdoors in nonpeak UV periods.
Inadequate synthesis in winter is seen as far south as Turkey and Israel [18].
Data from the European population shows that mean serum 25(OH)D levels of 20 to 30nmol/l (8 ng/mlto southern European centres to 40 to 50nmol/l in northern Europe among the elderly people [19]. This is relatively unusual as ultraviolet rays are more effective in the southern Europe than the northern Europe. Our study also shows similar results because though India is tropical country the vitamin D levels are lower in study subjects.
The results of our study are in concordance with the above mentioned studies. The Vitamin D levels were deficient in office going employees in south India. More than 90% of the individuals are either deficient or insufficient of Vitamin D. The vitamin D were measured in the last week of August, a month of rainy season. During this season the weather is cloudy and little UVB rays reaching the earth. The other possible risk factors could be less number of hours spent in sunlight and may be pollution playing its role as it prevents the UV B rays reaching the earth.
Although there is adequate sunshine in India high temperatures during daytime and sultry humid climate are deterrents to sun exposure [20].
The culture of clothing may also be one the reasons as Indians customarily wear cloths covering the entire body and exposing very little skin to UVB rays. Matsuoka LY, et al. study showed the significance of segmental body contributions to vitamin D3 production [21]. The study revealed that serum vitamin D3 levels were significantly higher in individuals exposing the trunk, legs and entire body to sunlight. In individuals exposing the head and neck or arms, the vitamin D3 level was higher than the basal level, but the difference was not significant. This may be one of the reasons for lower levels of vitamin D in our study subjects, as most of the office employees would be clothing covering the most of the body parts except for face and neck.
In previous study conducted in south India on Women of Reproductive (WR) and Postmenopausal (PMW) Age Groups have shown that in WR 25(OH)D deficiency, insufficiency and replete state was seen in 76%, 16.5% and 7.5% respectively and in the PMW 25(OH)D deficiency, insufficiency and replete states was seen in 70%, 23% and 7% respectively [22]. Our study also adds to the evidence that Women of Reproductive age group especially between 20 and 30 years of age are deficient in Vitamin D levels (67% were deficient of age group 20 and 40 years). Women in our study had higher prevalence of the deficiency (83% Vs 75%) when compared to men.
Vitamin D stores are depleted if the diet has high fiberin particular, phosphate and phytates, which is usually common in Indian food habit [23,24].
There is a possibility of role of genetics in the etiology of Vitamin D deficiency as Vitamin D levels have a significant hereditable component. The results from study by Awumey, EM et al. show that Asian Indians residing in the southern United States are at risk for developing vitamin D deficiency due to increased 25(OH)D-24- hydroxylase activity which degrades 25(OH)D to inactive metabolites [25]. This can be one of the possible reasons for vitamin D deficiency in our study as well.
Vitamin deficiency problem is not confined to India alone as it is widely prevalent in countries like China, Pakistan, Middle-East and Africa. The prevalence is less common in USA, Japan, northern Europe and Canada as they use the milk fortified with Vitamin D and Vitamin D supplements [18].
In northern Europe and Netherlands, the population have adequate levels of Vitamin D as there is high consumption of fatty fish and cod liver oil and have Vitamin D supplements [26].
Strategies to improve Vitamin D status [27,28]
National Institute for Health and Care Excellence (NICE) guidance classifies people who live or confined indoors for long period and South Asians as at risk group for developing Vitamin D deficiency. It has formulated certain guidelines for preventing Vitamin D deficiency among the population at risk. These include
Though food fortification might be one of the solutions for overcoming the problem of low vitamin D levels in general population, it has certain limitations. These could be, first the amount of vitamin D added to milk need to be adequate. Second, milk may not be consumed by all who are prone for deficient of Vitamin D. Third, only few products are fortified with vitamin D like yoghurt etc [29].
Strategies to improve food fortification may include fortifying new products such as calcium- and vitamin D-fortified orange juice, cheese and bread [30].
This is high time for public health policies to think of fortification of food with Vitamin D and about Vitamin D supplements. Dietary recommendation about Vitamin D and Calcium supplementation.
Conclusion
The study clearly brings forth the importance of exposure to sunlight in having the sufficient levels of Vitamin D. Office going people have minimal time to expose themselves to sunlight and hence are more prone for sunshine vitamin deficiency. Need of the hour is to increase the awareness about Vitamin D deficiency and importance of periodic Vitamin D screening. Also, emphasizing the importance of strategies for the prevention of Vitamin D deficiency like exposure to sunlight, fortification of food with vitamin D and Vitamin D supplements.
References
- Yin K, Agrawal DK (2014) Vitamin D and inflammatory diseases. J Inflamm Res 7: 69-87.
- Raman M, Milestone AN, Walters JR, Hart AL, Ghosh S (2011) Vitamin D and gastrointestinal diseases: inflammatory bowel disease and colorectal cancer. Therap Adv Gastroenterol 4: 49-62.
- Lange NE, Litonjua A, Hawrylowicz CM, Weiss S (2009) Vitamin D, the immune system and asthma. Expert Rev Clin Immunol 5: 693-702.
- Srinivasa PM, Harinarayan CV (2015) Vitamin D deficiency in India: fortify or let the sun shine in? J Clin Sci Res 4: 220-226.
- Rosen CJ, Abrams SA, Aloia JF, Brannon PM, Clinton SK, et al. (2012) IOM committee members respond to endocrine society Vitamin D guideline. J Clin Endocrinol Metab 97: 1146-1152.
- Harinarayan CV, Ramalakshmi T, Prasad UV, Sudhakar D (2008) Vitamin D status in Andhra Pradesh: a population based study. Indian J Med Res 127: 211-218.
- Szulc P, Meunier PJ (2003) Synergistic effect of vitamin D and calcium in preventing proximal femoral fractures in older patients. Joint Bone Spine 70: 157-160.
- Johnston CC, Miller JZ, Slemenda CW, Reister TK, Hui S, et al. (1992) Calcium supplementation and increases in bone mineral density in children. N Engl J Med 327: 82-87.
- Ghai B, Bansal D, Kapil G, Kanukula R, Lavudiya S, et al. (2015) High prevalence of hypovitaminosis D in Indian Chronic Low back patients. Pain Physician 18: E853-862.
- Cannell JJ, Hollis BW, Zasloff M, Heaney RP (2008) Diagnosis and treatment of vitamin D deficiency. Expert Opin Pharmacother 9: 107-118.
- Hollick MF (2007) Vitamin D deficiency. N Engl J Med 357: 266-281.
- Harinarayan CV, Joshi SR (2009) Vitamin D status in India--its implications and remedial measures. J Assoc Physicians India 57: 40-48.
- Harinarayan CV, Ramalakshmi T, Venkataprasad U (2004) High prevalence of low dietary calcium and low vitamin D status in healthy south Indians. Asia Pac J Clin Nutr 13: 359-364.
- Marwaha RK, Sripathy G (2008) Vitamin D and Bone mineral density of healthy school children in northern India. Indian J Med Res 127: 239-244.
- Harinarayan CV (2005) Prevalence of vitamin D insufficiency in postmenopausal South Indian women. Osteoporos Int 16: 397-402.
- Goswami R, Gupta N, Goswami D, Marwaha RK, Tandon N, et al. (2000) Prevalence and significance of low 25-hydroxyvitamin D concentrations in healthy subjects in Delhi. Am J Clin Nutr 72: 472-475.
- Vu LH, Whiteman DC, van der Pols JC, Kimlin MG, Neale RE (2011) Serum vitamin D levels in office workers in a subtropical climate. Photochem Photobiol 87: 714-720.
- WHO, Food and Agricultural Organization of the United Nations (2006) Guidelines on food fortification with micronutrients. pp. 1-346.
- van der Wielen RP, Löwik MR, van den Berg H, de Groot LC, Haller J, et al. (1995) Serum vitamin D concentrations among elderly people in Europe. Lancet 346: 207-210.
- Londhey V (2011) Vitamin D deficiency: Indian Scenario. J Assoc Physicians India 59: 695-696.
- Matsuoka LY, Wortsman J, Hollis BW (1990) Use of topical sunscreen for the evaluation of regional synthesis of vitamin D3. J Am Acad Dermatology 22: 772-775.
- Harinarayan CV, Sachan A, Reddy PA, Satish KM, Prasad UV, et al. (2011) Vitamin D status and bone mineral density in women of reproductive and postmenopausal age groups: a cross-sectional study from south India. J Assoc Physicians India 59: 698-704.
- Mithal A, Wahl DA, Bonjour JP, Burckhardt P, Dawson-Hughes B, et al (2009) Global vitamin D status and determinants of hypovitaminosis D. Osteoporos Int 20: 1807-1820.
- Goswami R, Mishra SK, Kochupillai N (2008) Prevalence & potential significance of vitamin D deficiency in Asian Indians. Indian J Med Res 127: 229-238.
- Awumey EM, Mitra DA, Hollis BW, Kumar R, Bell NH (1998) Vitamin D metabolism is altered in Asian Indians in the southern United States: a clinical research center study. J Clin Endocrinol Metab 83: 169-173.
- Brustad M, Sandanger T, Aksnes L, Lund E (2004) Vitamin D status in a rural population of northern Norway with high fish liver consumption. Public Health Nutr 7: 783-789.
- NICE (2017) National policy and strategy for preventing vitamin D deficiency.
- Calvo MS, Whiting SJ (2006) Public health strategies to overcome barriers to optimal vitamin D status in populations with special needs. J Nutr 136: 1135-139.
- Calvo MS, Whiting SJ, Barton CN (2004) Vitamin D fortification in the United States and Canada: current status and data needs. Am J Clin Nutr 80: 1710S-1716S.
- Tangpricha V, Koutkia P, Rieke SM, Chen TC, Perez AA, et al. (2003) Fortification of orange juice with vitamin D: a novel approach for enhancing vitamin D nutritional health. Am J Clin Nutr 77: 1478-1483.