Review Article
Geriatric Nutrition: A Bird Eye View
Pallavi Kiradi*
* Medical & Research Consultant, SAMI Labs Ltd, India
Corresponding author: Pallavi Kiradi, Medical & Research Consultant, SAMI Labs Ltd, India; E-mail: drpallavigp@gmail.com
Citation: Kiradi P. Geriatric Nutrition: A Bird Eye View. Indian J Nutri. 2017;4(3): 164.
Copyright © 2017 Kiradi P. This is an open access article distributed under the Creative CommonsAttribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided theoriginal work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 4, Issue: 3
Submission:13/06/2017; Accepted: 30/06/2017; Published: 13/07/2017
Abstract
India’s older population will increase dramatically over the next four decades. The share of India’s population ages 60 and older is projected to climb from 8% in 2010 to 19% in 2050, according to the United Nations Population Division (UN 2011). Almost one-half (47%) of older Indians have at least one chronic disease such as asthma, angina, arthritis, depression or diabetes [1]. Rising numbers of older people will put new and increasing demands on the health caresystem. In India, there is dearth of comprehensive information on the nutritional status of elderly. There is, therefore, a need to develop database on the diet and nutritional status of the elderly from different parts of the country to enable the Government and NGOs to formulate policies and initiate strategies, which would contribute to the wellbeing of elderly population. The last study report is been during 1996-97 from NNMB which was the first large database on diet and nutritional status of the elderly in India. A 2012 study at Allahabad concludes from the study that as the age advances there is corresponding decline in the nutritional status. Mean nutrient intake of malnourished elderly is less than the RDA and that of the well-nourished elderly. Per capita income and self-view of educational status are strongly associated factors contributing to the nutritional status of elderly. Out of the total of 360 elderly persons, 15% were found to be malnourished and 55% were at risk of malnutrition. There is thus an urgent need to review current recommended daily nutrient allowances for this group. Awareness, education and training are the need of the hour with some precautions. Therefore, the elderly need nutrient-rich foods rich in calcium, micronutrients and fiber. Apart from cereals and pulses, they need daily at least 200-300ml of milk and milk products and 400g of vegetables and fruits to provide fiber, micro-nutrients and antioxidants. Inclusion of these items in the diet improves the quality of the diet and bowel function. Flesh foods and eggs add to the quality of diet. The present focus is on the phytochemicals of nutraceutical importance for the geriatric population. Apart from the isolated extracts of plant chemicals as nutrition, a wide range of botanical ingredients are used as geriatric supplement to maintain healthy lifestyle.
Keywords:
Geriatric nutrition; Nutraceuticals; RDA; Antioxidant; Phytonutrition
Introduction
India’s older population will increase dramatically over the next four decades. The share of India’s population ages 60 and older is projected to climb from 8% in 2010 to 19% in 2050, according to the United Nations Population Division (UN 2011). Almost onehalf (47%) of older Indians have at least one chronic disease such as sthma, angina, arthritis, depression or diabetes [1]. Rising numbers of older people will put new and increasing demands on the health care system.
Geriatric nutrition applies nutrition principles to delay effects of aging and disease, to aid in the management of the physical, psychological and psychosocial changes commonly associated with growing old [2].
Historically, it’s no wonder that the ageing is defined as Swabhavajavyadhi Jara in Ayurveda which means it’s a natural phenomenon in every living being [3]. The objective of geriatric medicine or nutrition which is in tune with the Indian philosophy is essentially “Longer Life with lesser disease and painless death” or a self-sufficient life followed by a peaceful death [4]. In the name of Rasayana or Jara chikitsa geriatrics was a well established geriatric care in ancient India which was meant to enhance health by revitalizing the tissues that are in the process of wear out.
Despite the facts that Indian tradition has an enormous potential of traditional way of food & living, older people are vulnerable to malnutrition for many reasons including physiological and functional changes that occur with age, lack of financial support and inadequate access to food. The functional status of the elderly is their ability to carry out their day to day activities including preparation of food and intake, thereby affecting nutritional status. In India, the problem of the health of the elderly is compounded by poor nutrition together with medical issues, including both communicable and noncommunicable diseases. Malnutrition and morbidity create a vicious cycle.
Nutritional Status of Elderly Indian
In India, there is dearth of comprehensive information on the nutritional status of elderly. There is, therefore, a need to develop database on the diet and nutritional status of the elderly from different parts of the country to enable the Government and NGOs to formulate policies and initiate strategies, which would contribute to the wellbeing of elderly population. The last study report is beenduring 1996-97 from NNMB which was the first large database on diet and nutritional status of the elderly in India.
The results of the study indicated that, the overall intake of variousfoods except cereals & millets was less than RDI in males. Similarly, the average intake of all the nutrients except calcium, thiamine and Vitamin C was less than RDI [5].
There is however, a need to conduct comprehensive surveys including information on diet related chronic diseases and behavioral and psychosocial aspects in addition to diet and nutritional status. The nutrition and health of the elderly is often neglected. Most nutritional intervention programs are directed toward infants, young children, adolescents and pregnant & lactating mothers. However, nutritional interventions could play a part in the prevention of degenerative conditions of the elderly and an improvement of their quality of life.
Defining the Specific Nutritional Needs of Elderly
The cornerstone of geriatric nutrition is a well-balanced diet. This provides optimal nutrition to help delay the leading causes of death: heart disease, cancer and stroke. In addition, ongoing research indicates that dietary habits, such as restricting one’s calorie intake and consuming antioxidants, may increase longevity. A 2012 study at Allahabad concludes from the present study that as the age advances there is corresponding decline in the nutritional status. Mean nutrient intake of malnourished elderly is less than the RDA and that of the ell-nourished elderly. Per capita income and self-view of educational status are strongly associated factors contributing to the nutritional status of elderly [6]. Out of the total of 360 elderly persons, 15% were found to be malnourished and 55% were at risk of malnutrition. The association between nutritional status and older age group, female gender, dependent functional status, dependent financial status and inadequate calorie intake was found to be significant [7].
In conclusion, current trends in demographics coupled with rapid urbanization and lifestyle changes have led to an emergence of a host of problems faced by the elderly in India. Although the focus is on the medical problems of the elderly and strategies for improving health care services, it must be remembered that improving the quality of life of the elderly calls for a holistic approach and concerted efforts by the health and health related sectors.
What are the Risk Considerations to OPT forNutrition?
Geriatric group is generally prone for infections, injuries, psychological problems, degenerative problems. There is an increased risk of morbidity, mortality and disability [8]. The common manifestations would be infection, fluid & electrolyte balance, malnutrition, diabetes, hypertension, dizziness, blackouts and falls, fractures & painful joints, immobility, incontinence & retention, confusional states, dementia & neurodegenerative diseases, heart failure.
The process of ageing also affects other nutrient needs. For example, while requirements for some nutrients may be reduced, some data suggest that requirements for other essential nutrients may in fact rise in later life. There is thus an urgent need to review current recommended daily nutrient allowances for this group. There is also an increasing demand worldwide for WHO guidelines which competent national authorities can use to address the nutritional needs of their growing elderly populations.
What needs to be done in Indian Scenario?
Awareness
Elderly subjects should be encouraged to include iron & micronutrient rich foods Consumption of fruits, vegetables, whole grains and good hydration of at least 1,000mL of fluids/day. Fat free and low fat free dairy products, legumes, poultry, fish at least once a week, supervised medications and ensuring the drug compliance in elderly. Government, NGO, community, families, medical & social science faculties need to give greater emphasis, to provide health care, societal support & nutrition services to the elderly [9].
Training
Elderly patients are particularly at risk because more than 30% of all the prescription drugs are taken by this population [10]. At present, most of the geriatric Outpatient Department (OPD) services are available at tertiary care hospitals in India. Since 75% of the elderly reside in rural areas, it is mandatory that geriatric health care services be made a part of the primary health care services. This calls for specialized training of medical officers and other paramedics in geriatric nutrition. The elderly population has longevity on one hand and compromised quality of life on the other. The probable solution is multidimensional approach that comprises not only curative, but also non-curative methods of care that are essentially preventive which starts from the nutritional advice.
Education
The adverse health consequences of malnutrition are impaired muscle function, decreased bone mass, immune dysfunction, anemia, reduced cognition, delayed wound healing and delayed recovery from surgery, increased risk of falls, disability and mortality. Anorexia and malnutrition lead to muscle wasting and loss of subcutaneous fat leading to weight loss in elderly people. Malabsorption, hyper metabolism, cancers, admission to elderly home, acute illness, hospitalization, depression, various drugs, dysphagia, oral infections, dental issues, GI conditions, endocrine conditions such as thyroid diseases, poverty, reduced access to food and dehydration contribute further to weight loss. Awareness in the patients, caregivers and physicians related to this often neglected issue is important [11].
Precautions
Elderly people are vulnerable group. The care of drug nutrient interactions in elderly people is essential. The purpose of review before recommending nutrition could be the presence of multiple diseases, polypharmacy, malnutrition and impaired metabolism in elderly individuals increases the risks of adverse events related to drugfood interactions [12]. When investigating pharmacokinetic and pharmacodynamic modifications in the elderly, other factors have to be considered, such as anorexia, dementia, depression, intolerance, gastrointestinal-tract disorders, social and economic factors, reduced abilities (visual and manual) and difficulties in chewing or swallowing. In order to develop a correct drug prescription plan and nutritional intervention to avoid any kind of undesirable drug food interaction effect, it is necessary to adequately diagnose the disease and often re-evaluate the chosen treatment, identify disease stages and the ecessary therapies to minimize the number of drugs administered, and select a reasonable nutritional assessment.
Essential Nutrients required in Elderly
A Report of the Expert Group of the Indian Council of Medical Research 2009 from NIN (National Institute of Nutrition) guideline 15 recommends including micronutrient rich foods in the diets of elderly people to enable them to be fit and active [13]. Therefore, the elderly need nutrient-rich foods rich in calcium, micro-nutrients and fiber. Apart from cereals and pulses, they need daily at least 200- 300ml of milk and milk products and 400g of vegetables and fruits to provide fiber, micro-nutrients and antioxidants. Inclusion of these items in the diet improves the quality of the diet and bowel function. Flesh foods and eggs add to the quality of diet. There is no compelling evidence that suggests that protein requirements for the elderly are increased. There have been suggestions that the elderly require more protein intake, owing to a reduced absorptive capacity, but N balance studies do not provide enough evidence to make a recommendation for an increased protein intake. However, protein and energy are inter-related. In an elderly person whose activity is maintained, there is sufficient energy intake to ensure adequate protein intake. In the sedentary elderly person, with reduced energy requirement, there is a need to consider the protein energy ratio of the diet, since protein intake can reduce if the total diet is reduced.
The dietary guidelines also mentions importance of Riboflavin in elderly quoting to the study involving elderly subjects in Guatemala in which measurement of urinary riboflavin excretion and EGRAC were used, it was concluded that the requirement of healthy individuals aged above 60 years probably does not differ from that for individuals below 51 [14]. WHO recommends the below table of essential nutrients for the elderly (Table 1) [15].
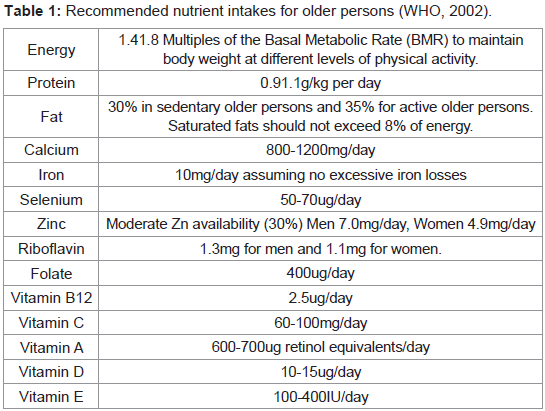
Table 1: Recommended nutrient intakes for older persons (WHO, 2002).
Phytonutrition or Nutraceuticals: - Much more than only Nutrition
Plant foods contain thousands of natural chemicals. These are called phytonutrients or phytochemicals.”Phyto” refers to the Greek word for plant. These chemicals help protect plants from germs, fungi, bugs and other threats. More than 25,000 phytonutrients are found in plant foods. These plant compounds have beneficial effects working with other essential nutrients to promote good health.
As Nutritional status is one of the chief variables that explains differences in both the incidence and pathology of infection. Elderly people are at increased risk for micronutrient deficiencies due to a variety of factors including social, physical, economic and emotional obstacles to eating. Thus there is an urgent need to shift priorities to increase our attention on ways to prevent chronic illnesses associated with aging. Individually, people must put increased efforts into establishing healthy lifestyle practices, including consuming a more healthful diet. The present focus is on the phytochemicals of nutraceutical importance for the geriatric population.
Some of the most essential Nutraceuticals are:-
1. Antioxidants
2. Plant polyphenols and catechins: Turmeric, green tea, grapeseed etc.
3. Carotenoids: Lutein, zeaxanthin, and lycopene
4. Plant phenols/sterols (phytosterols)
5. Omega-3 fatty acids
6. Glucosamine, chondroitin, collagen and quercetin
7. Prebiotics and probiotics
8. Coenzyme Q10
Dietary Botanicals as Geriatric Nutrition
Apart from the isolated extracts of plant chemicals as nutrition, a wide range of botanical ingredients are used as geriatric supplement to maintain healthy lifestyle. The common examples being Ginkgo biloba for neuroprotection, Vaccinium corymbosum (blueberry) for lifespan extension, Cranberry and oregano for longevity promotion,Nectarine and acai for life span extension, Rosa damascena for life span extension, Green tea as health supplement, Cocoa polyphenols and longevity effect, Olive oil as a phenolics supplement, Quercetin and tannic acid as health supplement. Curcumin (diferuloylmethane) is the pharmacologically active substance in turmeric (Curcuma longa), and has been widely used as an herbal medicine in Asia. It is well documented that curcumin possesses many biological activities, such as antioxidative, anti-inflammatory, anticancer, chemopreventive and anti-neurodegenerative properties. With its pleiotropic activities, curcumin has been considered as a potentialaging intervention compound.
Demographic evidence and statistical data support the fact that the population in the developing countries is growing older. India is evincing it. Dietary requirements change in elderly people.
A multidisciplinary approach may assist in managing this class. Tailoring nutritional advice to these individuals is very essential. Assessment and treatment of nutritional risk should be part of routine care for the elderly, just as assessment and management of cardiovascular risk factors are standard practice in adults.
References
- Scommegna P (2012) India’s aging population. Population Ref Bur.
- Jacqueline L Longe (2006) The gale encyclopedia of nursing & allied health, (2nd edn). Thomson Gale, USA, 4: pp. 3093.
- Warrier PR (1982) Problems of aging jara cikitsa - The ayurvedic treatment for preventing and curing senility. Anc Sci Life 1: 210-215.
- Vijayaraghavan K, Venkaiah K, Damayanthi K, Uma nayak M (2000) Special report on nutritional status of elderly & adolescents, food & nutrient intakes of individuals. Natl Nutr Monit Bur pp. 1-95.
- Neelam Yadav, Ravindra R, Sharma S, Singh A, Mishra M, et al. (2012) Dietary habits and nutritional status of elderly living in urban areas of Allahabad district. Indian J Prev Soc Med 43: 81-86.
- Ingle GK, Nath A (2008) Geriatric health in India: Concerns and solutions. Indian J Community Med 33: 214-218.
- Gheno R, Cepparo JM, Rosca CE, Cotten A (2012) Musculoskeletal disorders in the elderly. J Clin Imaging Sci 2:39.
- Agarwalla R, Saikia AM, Baruah R (2015) Assessment of the nutritional status of the elderly and its correlates. J Family Community Med 22: 39-43.
- Genser D (2008) Food and drug interaction: Consequences for the nutrition/health status. Ann Nutr Metab 52(Suppl 1): 29-32.
- Santosh B Salagre (2013) Health issues in geriatrics, Section 26, Chapter 177. Volume 23.
- Akamine D1, Filho MK, Peres CM (2007) Drug-nutrient interactions in elderly people. Curr Opin Clin Nutr Metab Care 10: 304-310.
- Krishnaswamy K (2011) Dietary guidelines for Indians-A manual. National Institute of Nutrition, ICMR, Hyderabad, pp. 1-123.
- Boisvert WA, Mendoza I, Castaneda C, De Portocarrero L, Solomons NW, et al. (1993) Riboflavin requirement of healthy elderly humans and its relationship to macronutrient composition of the diet. J Nutr 123: 915- 925.
- Gupta C, Prakash D (2015) Nutraceuticals for geriatrics. J Tradit Complement Med 5: 5-14.
- Maryann Tomovich Jacobsen (2014) Diet & Weight Management Phytonutrients.