Research Article
Evaluation of Lipid Profile of Type 2 Diabetic Patients Attending an Urban Tertiary Health Facility in Nigeria
Funmilayo Esther Omotoye* and Grace Tanimoowo Fadupin
Human Nutrition Department, Faculty of Public Health, University of Ibadan, Oyo State, Nigeria
Corresponding author: Funmilayo Esther Omotoye, Human Nutrition Department, Faculty of Public Health, Universityof Ibadan, Oyo State, Nigeria, Tel: 08039575579; E-mail:funmiomotoye2013@gmail.com
Citation: Omotoye FE, Fadupin GT. Evaluation of Lipid Profile of Type 2 Diabetic Patients Attending an Urban Tertiary Health Facility in Nigeria. Indian J Nutri. 2017;4(2): 159.
Copyright © 2017 Omotoye FE, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 4, Issue: 2
Submission: 04/02/2017; Accepted: 25/04/2017; Published: 17/05/2017
Abstract
Type 2 diabetes is associated with a marked increased risk of Cardiovascular Disease (CVD). A significant component of such risk can be attributed to diabetic dyslipidemia. This study aimed at evaluating the lipid profile of type 2 diabetics in an urban tertiary health facility in Nigeria.
Methods: A total of 50 consenting type II diabetic patients, aged 40-72 years were studied. Demographic characteristics and medical history of participants were assessed using semi-structured interviewer administered questionnaire. The serum lipids of participants (Total Cholesterol (TCHOL), Triglycerides (TRG), High Density Lipoproteins (HDL-C), and Low Density Lipoproteins (LDL-C) levels) for the last six months and the mean of their last four Fasting Blood Glucose (FBG) levels were assessed from their hospital records. Data was analyzed using descriptive statistics and chi-square. Difference in means was assessed using ANOVA. Significance was set at p<0.05.
Results: The mean age of respondents was 57.82 ± 3.3 years. A total of 68% had either secondary or tertiary education. According to our results, 70.0% of diabetic patients presented at least one lipid abnormality. Elevated LDL-C, TCHOL, TRG, and reduced HDL-C levels were noted in 34%, 36%, 12%, and 72% of the patients, respectively. Combination of elevated LDL and reduced HDL-C was the most prevalent of combined lipid abnormalities. There were no statistically significant differences in the levels of HDL-C, TCHOL, TRG, and FBG between men and women. However there was significant difference between Triglyceride and blood glucose.
Conclusion: Type 2 diabetic’s dyslipidemia was very common especially low HDL and raised Total cholesterol levels.
Keywords:
Type 2 diabetes; Lipid profile; Dyslipidemia
Introduction
Diabetes is characterized by chronic hyperglycemia and disturbances of carbohydrate, lipid and protein metabolism [1]. Dyslipidemia is one of the major risk factor for cardiovascular disease in Type 2 Diabetes mellitus, characterized by elevated Total cholesterol (TC), Triglycerides (TG), Low density lipoprotein (LDL) and decreased High density lipoprotein (HDL) [2]. Because detection and treatment of dyslipidemia is one means of reducing Cardiovascular Disease (CVD) risk, determination of serum lipid levels in people with diabetes is now considered a standard of care [3].
Diabetes causes about 5% of all deaths globally each year. The World Health Organization (WHO) report in 2010 estimates that the number of diabetic patients in Oman will increase up to 190% over the next 20 years, from 75,5000 in 2000 to 217,000 in 2025 [4]. Several previous studies have attempted to correlate blood glucose levels with serum lipid profile parameters [5]. Research findings show that mainly body fat is responsible for increase in prevalence of this disease among the body composition components [1,6].
The term diabetic dyslipidemia comprises a triad of raised triglycerides, reduced High Density Lipoprotein (HDL) and excess of small, dense Low Density Lipoprotein (LDL) particles. The lipid abnormalities are prevalent in diabetes mellitus because insulin resistance or deficiency affects key enzymes and pathways in lipid metabolism [1]. The causal association between atherosclerosis and dyslipidemia is well established. In diabetes the associated hyperglycemia, obesity and insulin changes highly accelerate the progression to atherosclerosis [7]. Type 2 diabetes is associated with a cluster of interrelated plasma lipid and lipoprotein abnormalities, including reduced HDL cholesterol, a predominance of small dense LDL particles, and elevated triglycerides [8]. These abnormalities occur in many patients despite normal LDL cholesterol levels. There is evidence that each of these dyslipidemic features is associated with increased risk of cardiovascular disease, the leading cause of death in patients with type 2 diabetes. [8].
The aims of our study were to find characteristics of lipid parameters in the population under study, to find gender differences in the parameters, and to determine the frequency and pattern of hyperlipidemia in patients with diabetes mellitus.
Methods
The study was descriptive cross sectional in design to evaluate the lipid profile of type 2 diabetic patients. Fifty type 2 diabetic patients attending the Medical Outpatient clinic (MOP) of the university college hospital Ibadan, Oyo State, Nigeria voluntarily participated in the study after obtaining their informed written consent and their age ranged from 40-72 years. The objectives of the present study were thoroughly explained to them. Clinical history was also documented.
A semi structured interviewer administered questionnaire was used to interview each patient that gave their consent to participate in the study and also had his/her lipid profile assessed within the last six months. Information with regards to the participants’ demographic data namely, age, sex, tribe, religion, occupation, and educational status were obtained with the aid of the questionnaire. In addition, medical history including family history of diabetes mellitus, information on duration of illness, diagnosis, and type of treatment given were obtained.
Records of their fasting blood glucose in form of means of the last four fasting blood glucose and record of their lipid profile level were obtained from their hospital records. Fasting blood glucose level <7.00 mmol/L (126 mg/dl) was regarded as controlled (good glycemic control) while the target lipid values were LDL<130 mg/dl, HDL >40 mg/dl, Triglyceride <150 mg/dl, and Total cholesterol <200 mg/dl.
By using the guidelines of the Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) for serum lipid profile reference level, hypercholesterolemia was defined as TC>200 mg/dl, high LDL-C when value is ≥130 mg/dl, hypertriglyceride as TG>150 mg/dl, and low HDL-C as <40 mg/dl. Dyslipidemia was defined by presence of one or more abnormal serum lipid concentration. Definition for Normal TC was <200 mg/dl, LDL-C was <130 mg/dl, TG was <150 mg/dl and HDL-C was ≥40 mg/dl [NCEP 2001] [9,10]. Diabetes was defined as per American Diabetes Association (ADA) criteria.
The current World Health Organization (WHO) diagnostic criteria for diabetes was fasting plasma glucose ≥ 7.0 mmol/l (126 mg/dl) or 2h plasma glucose ≥ 11.1 mmol/l (200 mg/dl) while normal FBG was <100 mg/dL (5.6 mmol/l) World Health Organization 2006, American Diabetes Association 2010 [10,11].
Data Analysis
The data were evaluated by Statistical Package for Social Sciences (SPSS) 16.0 version software. Data was analyzed using descriptive statistics and chi-square. Independent samples t-test (2-tailed) was used to compare means of different parameters between males and females. Frequency of dyslipidemia was evaluated while the pattern was determined by serum level for cholesterol, high density lipoprotein HDL-C, low density lipoprotein LDL-C and triglyceride. The results were considered statistically significant when P ≤ 0.05. For the descriptive and inferential statistics ANOVA was used.
Results
Table 1 shows the quantitative analysis of lipid profile of Type 2 diabetics and found that the mean total cholesterol was (167.24 ± 53.3 mg/dl), triglycerides (95.84 ± 39.9 mg/dl), HDL (50.16 ± 19.1 mg/dl), LDL (110.50 ± 41.9 mg/dl) & LDL / HDL ratio (2.24 ± 7.2). A total of 50 participants; 20 (40%) males and 30 (60%) females were recruited for the study. The mean age of the participants was 57.82 ± 3.3 years (60.85 ± 8.0 and 55.80 ± 8.6 male and female respectively) while their age ranges between 40 and 72 years. The participants were predominantly Yorubas (90.0%) and 94% were married. Duration of diabetic mellitus was more frequent within one to five years. Mean of the lipid profiles was not significant between male and female. However there was significant difference between the mean age of male and female. Also, there was significant difference between Triglyceride and blood glucose (P<0.05).
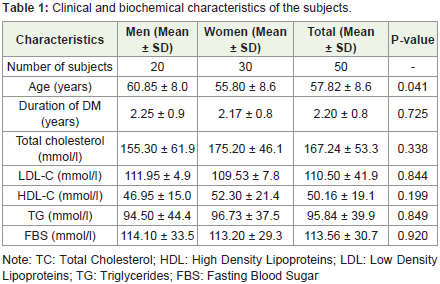
Table 1: Clinical and biochemical characteristics of the subjects.
As shown in Tables 2 and 3, 36% of the participant had high total cholesterol, 12% had high triglyceride, 72% had low HDL-C while 34% had high LDL. A total of 18 (36%) had very low HDL <40 mg/dl while 9 (18.0%) had very high LDL-C (≥160).
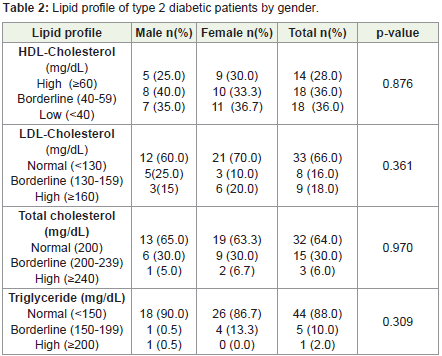
Table 2: Lipid profile of type 2 diabetic patients by gender.
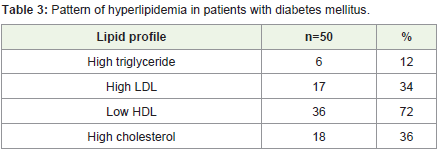
Table 3: Pattern of hyperlipidemia in patients with diabetes mellitus.
In Table 4 Low density lipoprotein (135.67 ± 39.0 male and 115.24 ± 46.6 female) and TG (115.50 ± 57.8 male, and 101.94 ± 39.1 female) were highest among 50-59 years age group respectively while TC was highest among 70-79 years in both male (180.25 ± 46.5) and female(200.50 ± 2.1) participants. HDL was lowest among 60-69 years male(43.50 ± 15.3) and 40-49 years female (44.67 ± 13.3).
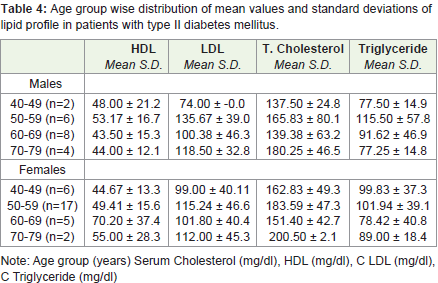
Table 4: Age group wise distribution of mean values and standard deviations of lipid profile in patients with type II diabetes mellitus.
Discussion
Dyslipidemia is a major risk factor for macrovascular complications in patients with type 2 diabetes [12]. We studied the evaluation of lipid profile of type 2 diabetic patients attending an urban tertiary health facility in Nigeria. Elevated Low-Density Lipoprotein Cholesterol (LDL-C) is a major risk factor for CVD. Management of LDL-C is the primary goal of therapy for diabetic dyslipidemia [12].
Our study showed that out of the 50 patients studied 35 (70%) had dyslipidemia. This was similar to a study by which showed that 72% of total patients had dyslipidemia [13]. Lipid abnormalities are common in diabetics and frequently seen in type-2 diabetics. Dyslipidemia make diabetics prone to develop CHD and other complications of atherosclerosis [13]. According to the CDC, 97% of adults with diabetes have one or more lipid abnormalities while the prevalence of diabetic dyslipidemia varies from 25% to 60% in other studies [14]. This variation in prevalence may be due to differences in BMI and possibly genetic variation [14].
This study showed that the mean total cholesterol (175.20 ± 46.1 vs 155.30 ± 61.9), High Density Lipoprotein C (HDL-C) (52.30 ± 21.4 vs 46.95 ± 15.0), triglyceride (96.73 ± 37.5 vs 94.50 ± 44.4) were higher among the female subjects, while Low Density Lipoprotein C (LDL-C) was higher among the male subjects (111.95 ± 4.9 vs 109.53 ± 7.8). The most frequent lipid combination was LDL + HDLC. It is important to realize that hyperlipidemia can develop even in the ‘prediabetes phase’ of type 2 DM. Hence, early detection and correction of dyslipidemic state is essential in the management of diabetic patients. This finding was consistent with that by which states that males had higher levels of LDL-C as compared to females, 19% diabetic males had LDL-C >160 mg/dl [13]. Our results are partly consistent with a study by, who reported that adverse effects of diabetes mellitus on dyslipidemia are more marked in women than men [15]. This explains why diabetes eliminates or attenuates a woman’s protection against IHD.
The present study also analyzed the prevalence rate of hypercholesterolemia, hypertriglyceridemia, low HDL and high low density lipoproteinaemia among type 2 diabetics. It was found that 36% Type 2 diabetics in this study had hypercholesterolemia, 12% Hypertriglyceridemia, 72% Low HDL and 34% abnormal LDL levels. In 36% of Type 2 diabetics, the HDL was less than 40 mg/dl. Thus, the results of the present study shows that in Type 2 diabetics the dyslipidemia is the most common abnormality and it was found in the level of HDL-C value. These findings were similar to that of which showed that Elevated LDL-C, elevated TCHOL, elevated TRG, and reduced HDL-C levels were noted in 28.37%, 36.37%, 39.01%, and 30.12% of the patients, respectively [16]. The combination of elevated TRG and reduced HDL-C was the most prevalent of the combined lipid abnormalities. In this study, 18% type 2 diabetics had HDL-C <35 mg/dl. Low HDL-C was a common associated finding with raised serum TG, serum cholesterol and LDL-C this was similar to the study by 14% type 2 diabetics had HDL-C <35 mg/dl. The percentages of dyslipidemia in our study were lower than the findings of another study of Lipid Profile in Type 2 Diabetic Punjabi Population which showed that 98% of Type 2 diabetics had high LDL levels and 59% showed hypercholesterolemia [13,17]. This observation further confirms that patients with Type 2 diabetes had co-incidence of several abnormal lipid profiles. It further confirms that dyslipidemia could have impact on the development of insulin resistance in type 2 diabetes mellitus [17]. This present study showed that dyslipidemia was common with type 2 diabetics. This was similar to the findings of which showed that type 2 diabetics were either overweight or type I obese and dyslipidemia was very common [17].
Low density lipoprotein and TG were highest among 50-59 years age group while TC was highest among 70-79 years in both male and female participants. HDL was lowest among 60-69 years male and 40-49 years female. A similar study showed that Median and upper range of total cholesterol, HDL-C and LDL-C were found to be higher in women than in men in all the age groups. However triacylglycerol and VLDL-C concentrations were observed to be higher in the men than women except in age group of 61-70 years. [18]. In another study, all lipid levels except LDL were higher among 41 to 60 years age group while LDL was higher among participants aged >60 years [19].
Conclusion
It is concluded from the results of the present study that dyslipidemia was very common among type 2 diabetic patients. Overall 70% participants had abnormal lipid profile. Higher percentage of women than men had abnormal lipid profile. Diabetes mellitus occurs with dyslipidemia. Results strongly suggest that further investigations should relate the effects of dyslipidemia and abnormalities of insulin resistance in type 2 diabetics. Common lipid abnormalities in diabetes are patterns of lipid profile in type- 2 diabetics and non raised triglycerides, LDL-C serum cholesterol and low diabetics. Therefore good glycaemic control can prevent development and progression of lipid-abnormalities among patients with diabetes mellitus.
There is enough evidence in literature to support the beneficial effect of lowering of serum lipids in retarding macro-vascular disease. Hence, early detection and correction of dyslipidemic state is essential in the management of diabetic patients.
Outcome of this study showed that majority of type 2 diabetes mellitus had uncontrolled blood sugar levels and most had their lipid levels deranged.
References
- Ozder A (2014) Lipid profile abnormalities seen in T2DM patients in primary healthcare in Turkey: A cross-sectional study. Lipids Health Dis 13: 183.
- Reddy AS, Meera S, William E, Kumar JS (2014) Correlation between glycemic control and lipid profile in type 2 diabetic patients: HbA1c as an indirect indicator of dyslipidemia. Asian J Pharm Clin Res 7: 153-155.
- Kayode JA, Adediran OS, Agboola S, Adebisi SA, Idowu A, et al. (2010) Lipid profile of type 2 diabetic patients at a rural tertiary hospital in Nigeria. J Diabetes Endocrinol 1: 46-51.
- Al-Alawi SA (2014) Serum lipid profile and glycated hemoglobin status in Omani patients with type2 diabetes mellitus attending a primary care polyclinic. Biomed Res 25: 161-166.
- Habiba NM, Fulda KG, Basha R, Shah D, Fernando S, et al. (2016) Correlation of lipid profile and risk of developing type 2 diabetes mellitus in 10-14 year old children. Cell Physiol Biochem 39: 1695-1704.
- Unalacak M, Kara IH, Baltaci D, Erdem O, Bucaktepe PG (2011) Effects of Ramadan fasting on biochemical and hematological parameters and cytokines in healthy and obese individuals. Metab Syndr Relat Disord 9: 157-161.
- Matheus AS, Tannus LR, Cobas RA, Palma CC, Negrato CA (2013) Impact of diabetes on cardiovascular disease: An update. Int J Hypertens 2013: 653789.
- Krauss RM (2004) Lipids and lipoproteins in patients with type 2 diabetes. Diabetes Care 27: 1496-1504.
- NCEP (2001) Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert panel on detection, Evaluation, and Treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA 285: 2486-2497.
- American Diabetes Association (2010) Diagnosis and classification of diabetes mellitus. Diabetes care 33: S62-S69.
- World Health Organization (2006) Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia: Report of a WHO/IDF Consultation. International Diabetes Federation, pp. 1-41.
- Vijayaraghavan K (2010) Treatment of dyslipidemia in patients with type 2 diabetes. Lipids Health Dis 9: 144.
- Uttra KM, Devrajani BR, Shah SZ, Devrajani T, Das T, et al. (2011) Lipid profile of patients with diabetes mellitus (A Multidisciplinary Study). World Appl Sci J 12: 1382-1384.
- Hidron AI, Edwards JR, Patel J, Horan TC, Sievert DM, et al. (2008) NHSN annual update: Antimicrobial-resistant pathogens associated with healthcare-associated infections: Annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control Prevention, 2006-2007. Infect Control Hosp Epidemiol 29: 996-1011.
- Firdous S, Khan MZ (2007) Comparison of patterns of lipid profile in type-2 diabetics and non diabetics. Ann King Edward Med Coll 3: 84-87.
- Stamouli M, Pouliakis A, Mourtzikou A, Skliris A, Panagiotou I, et al. (2014) Evaluation of the lipid profile in type 2 diabetes mellitus patients in Greece. Clin Lab 60: 1593-600.
- Singh G, Kumar AK (2012) A study of lipid profile in type 2 diabetic Punjabi population. J Exercise Sci Physiother 8: 7-10.
- Das M, Saikia M (2009) Estimation of reference interval of lipid profile in assamese population. Indian J Clin Biochem 24: 190-193.
- Limbu YR, Rai SK, Ono K, Kurokawa M, Yanagida JI, et al. (2008) Lipid profile of adult Nepalese population. Nepal Med Coll J 10: 4-7.